553 Photos and videos




John Njoroge retweeted

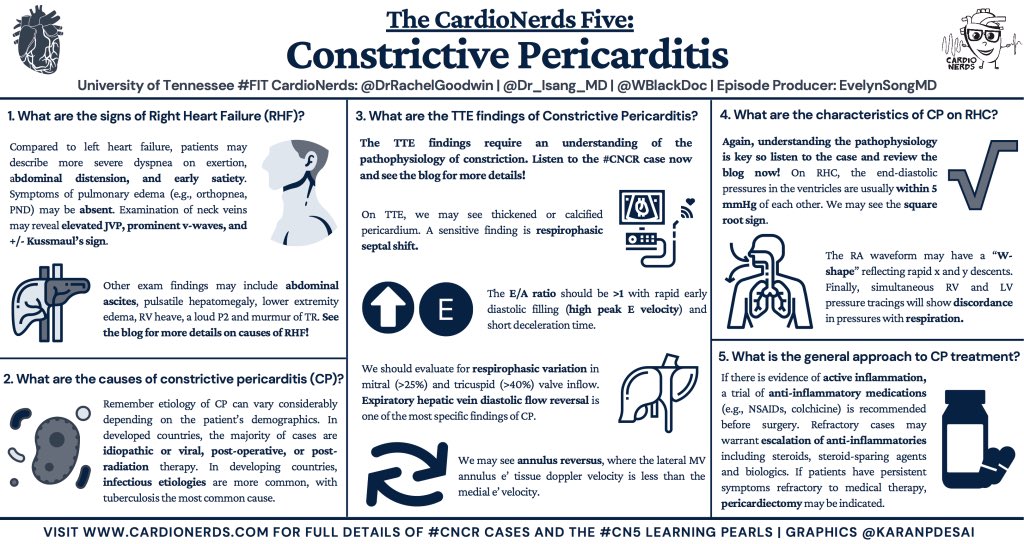
It's weird historical advertisement Thursday!
Let us suppose you've made some cream that (you claim) is rapidly absorbed by the skin, and is nourishing.
What might you call this delightful cream? Maybe a name that isn't horrifying?
Ah, yes, of course. Flesh food. (1909) 1/🍗
1
2
12
324
John Njoroge retweeted

1/8
Most students are taught that Romberg tests balance
It doesn't
The Romberg test asks a different question:
Can the patient still tell where their body is in space when vision is removed?
It is a test of proprioception - and whether vision is compensating for its loss.
3
3
24
5,133
John Njoroge retweeted

Jun 7
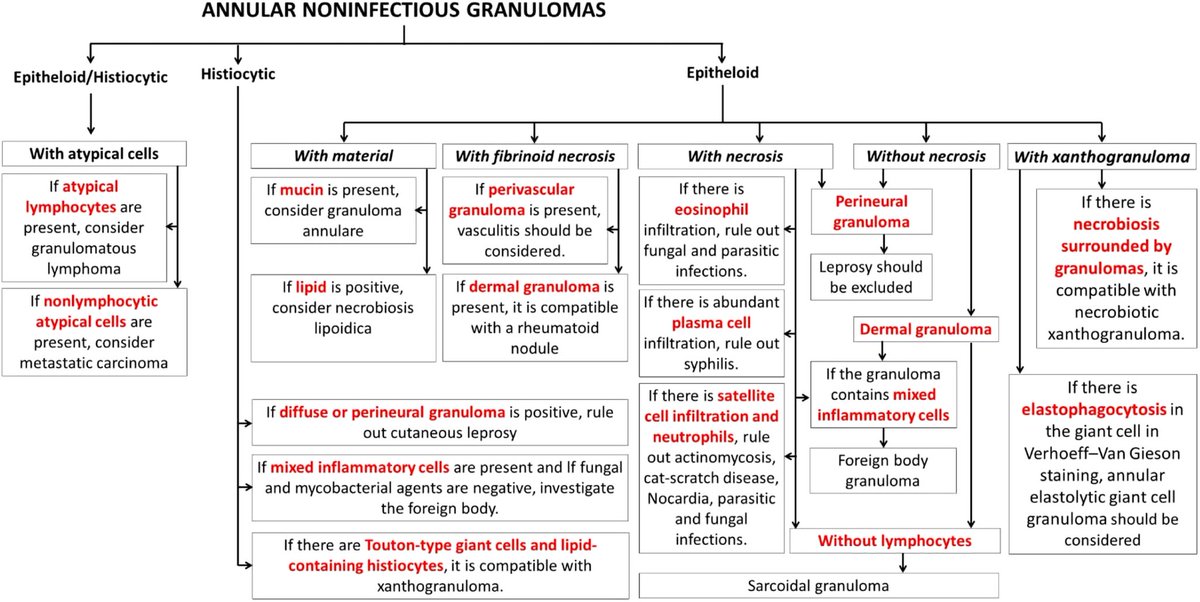
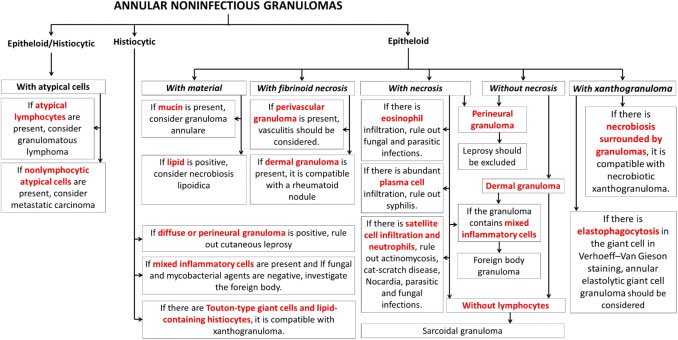
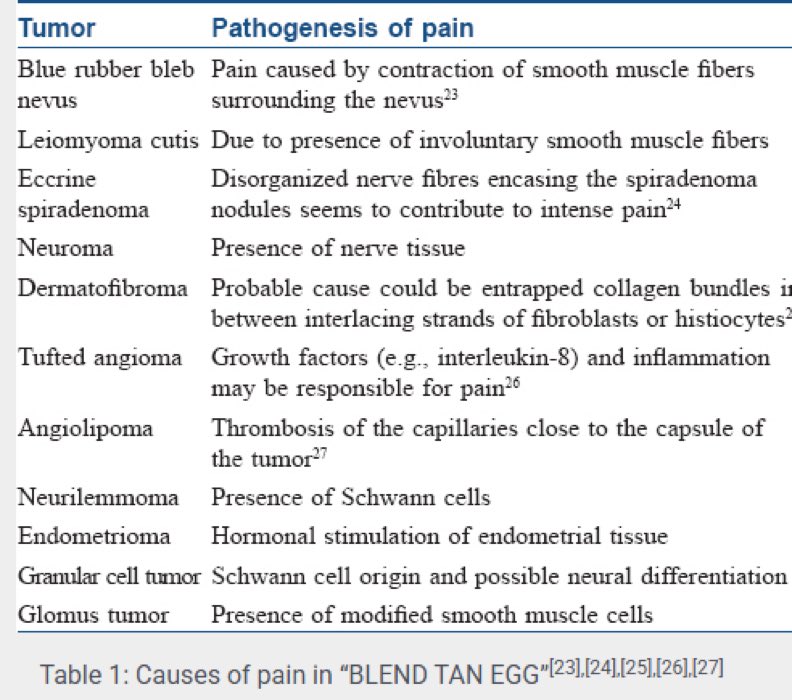
A man in his 70s w/ pancytopenia, IgG-λ MGUS, remote stage I colon adenocarcinoma s/p hemicolectomy, & noncirrhotic portal hypertension due to nodular regenerative hyperplasia complicated by ascites presented w/ progressive cutaneous lesions. Five years earlier, he developed recurrent periocular papules that rapidly recurred after excision & progressively spread to the trunk & extremities, w/ subsequent ulceration. He denied ocular symptoms.
O/E: multiple yellow-brown papules & plaques involving the medial upper eyelids & infraorbital skin, along with scattered yellow-brown flat-topped papules on the trunk & extremities. A large ulcer arising within a yellow-brown plaque was present on the right knee. There was no evidence of uveitis, conjunctivitis, or macroglossia.
What’s your DDx❓

5
1
24
1,923
John Njoroge retweeted

1 Aug 2022
Charcot was a man with many clinical interests beyond neurology. There's no better evidence than his enormous list of eponyms. To my knowledge, it's the longest in the history of medicine.
#medicalhistory #neurology #neurotwitter
1/7
28 Jul 2022

Let's talk about Jean-Martin Charcot, the "Father of Neurology"! He casts a shadow too wide to cover in one #tweetorial. First, let's talk about his training and legacy as a teacher (and stay tuned for more about him later).
#neurotwitter #neurology #medicalhistory
1/10

5
13
37
John Njoroge retweeted
28 Jul 2022
Let's talk about Jean-Martin Charcot, the "Father of Neurology"! He casts a shadow too wide to cover in one #tweetorial. First, let's talk about his training and legacy as a teacher (and stay tuned for more about him later).
#neurotwitter #neurology #medicalhistory
1/10
9
76
242
John Njoroge retweeted

Abx can be stopped when symptoms resolve. Fever may not be the only sign or symptom. If you use evidence based short course Tx, it will end around when Si/Sx resolve. Stop using long historical durations. And stop repeating myth that completing course of Tx prevents resistance.
3
6
42
8,461
John Njoroge retweeted

Jun 3
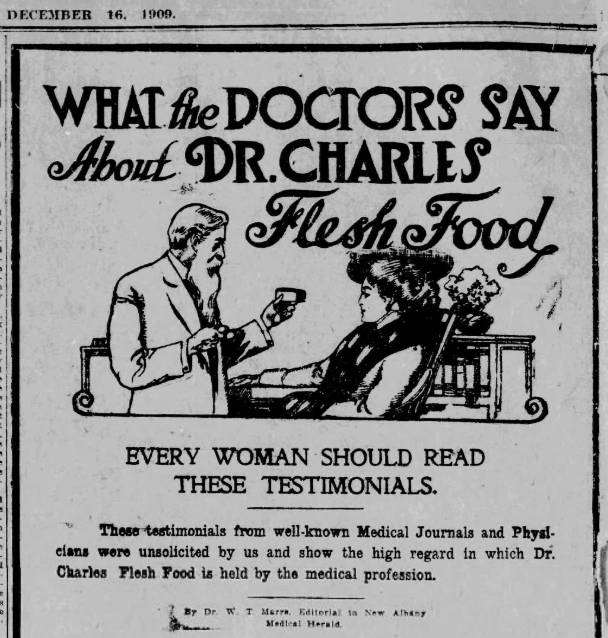
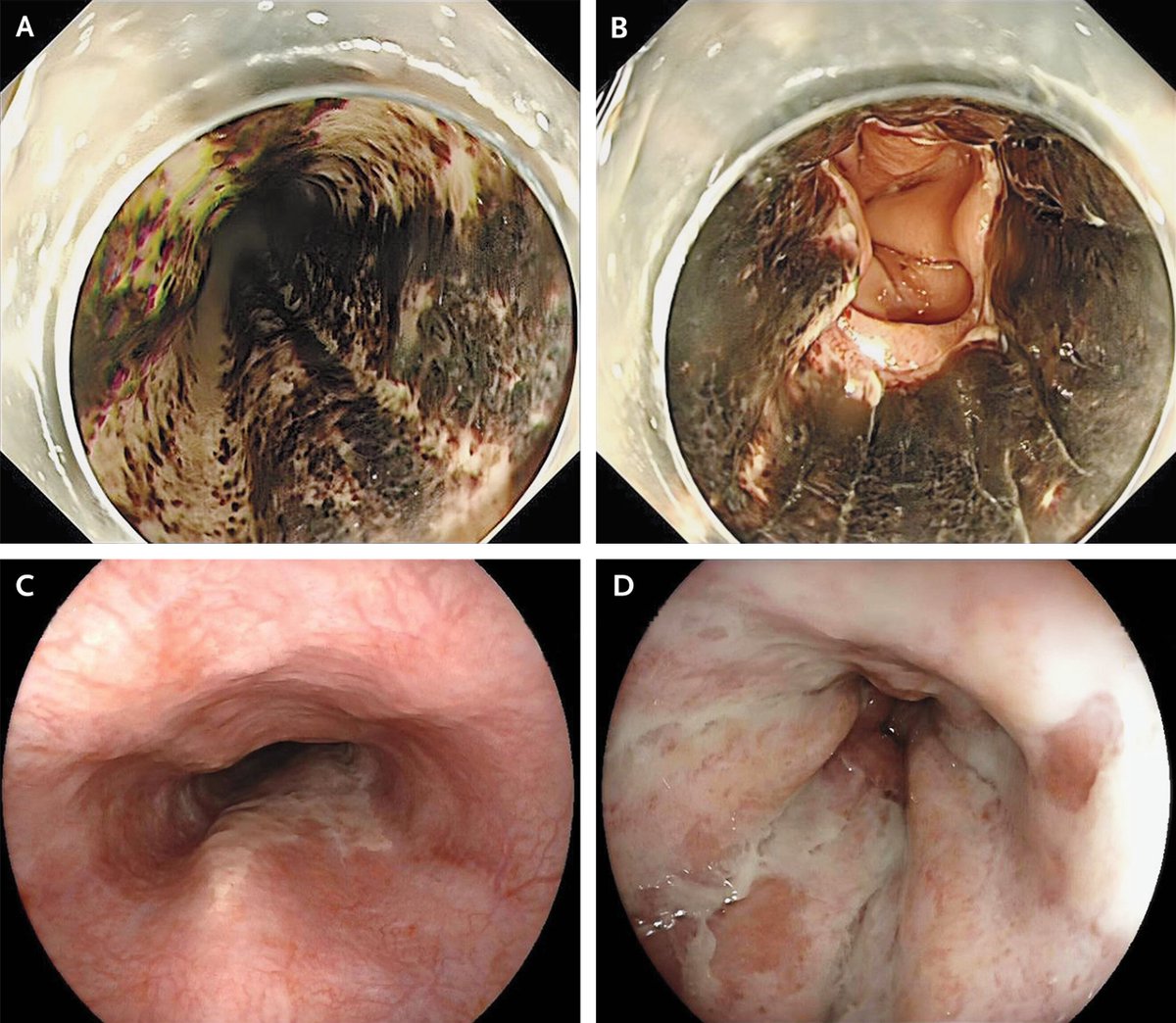
An easy NEJM image challenge today - endoscopic findings of the oesophagus in a patient with coffee ground vomiting. These were the findings on admission (top row) and one week later (bottom row). What’s the name of this syndrome?
11
11
102
23,024
John Njoroge retweeted

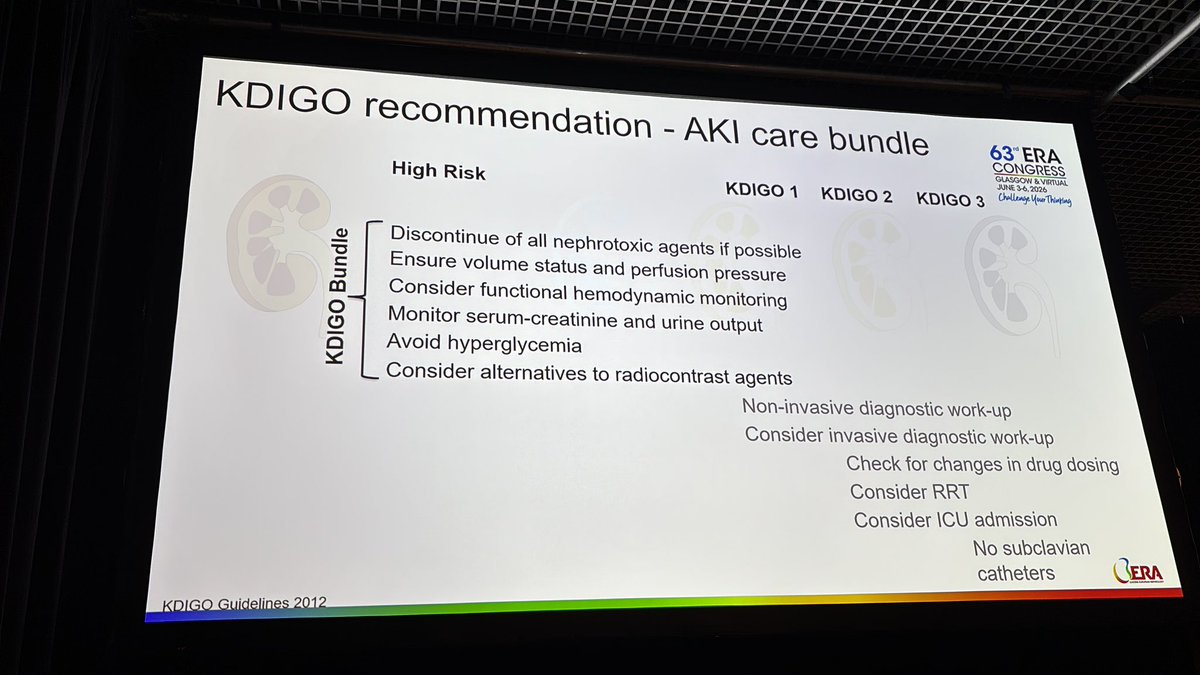
ASN has released the program this year's #KidneyWk and I always thought they should lean into controversy, but this is going over the line.
A cage match?
Bare knuckle boxing?

6
6
23
3,308

John Njoroge retweeted

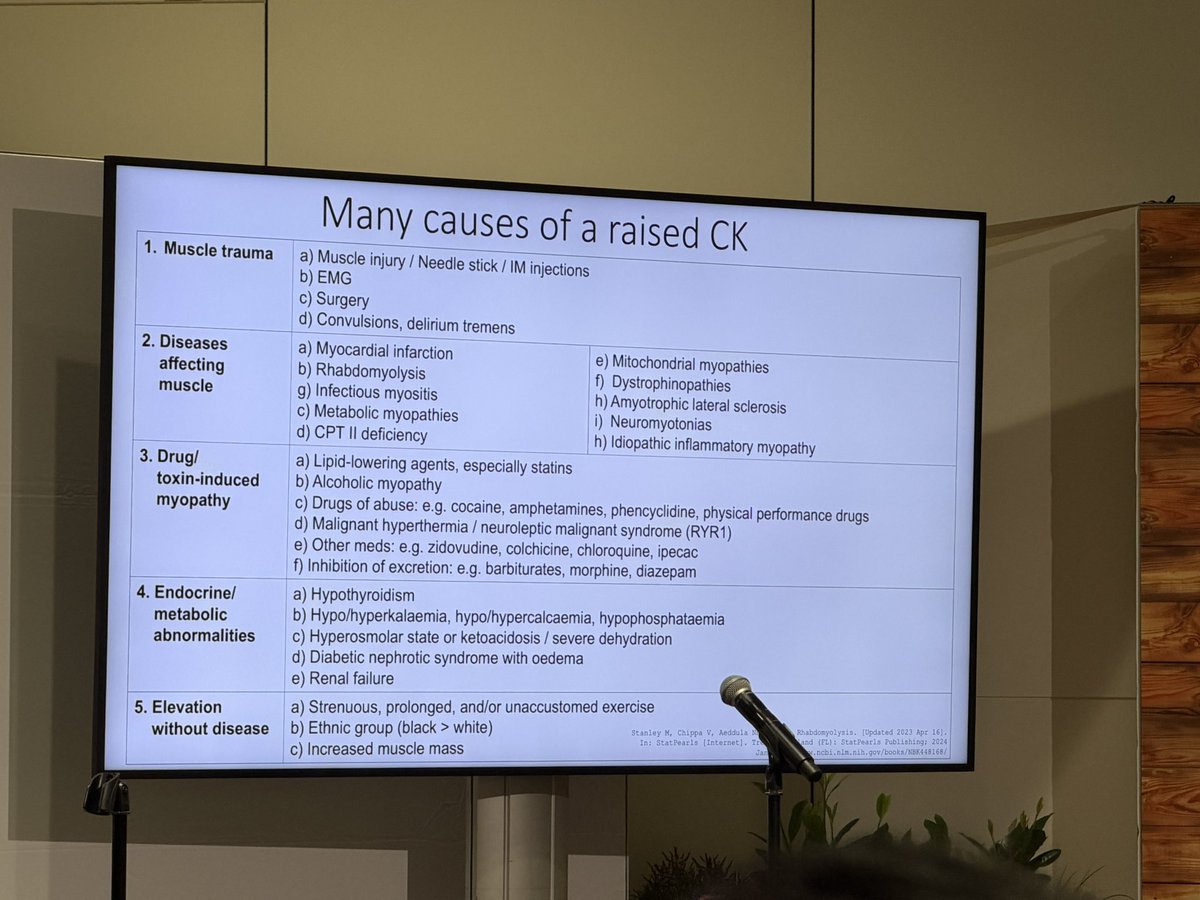
Jun 3
Considering non-myopathic causes of elevated CK before initiating an extensive neuromuscular workup is essential for diagnostic efficiency, patient safety. Up to 1.3% of the general population exhibits asymptomatic or oligosymptomatic hyperCKemia, #eular2026 #london #autoimmune
5
10
2,929
John Njoroge retweeted

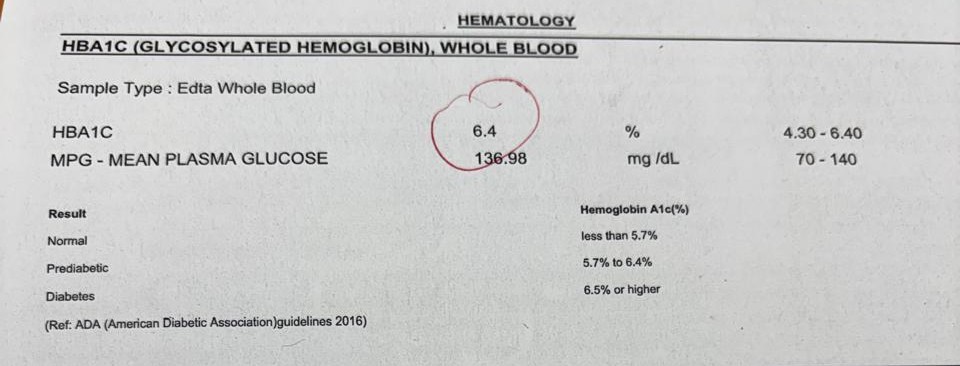
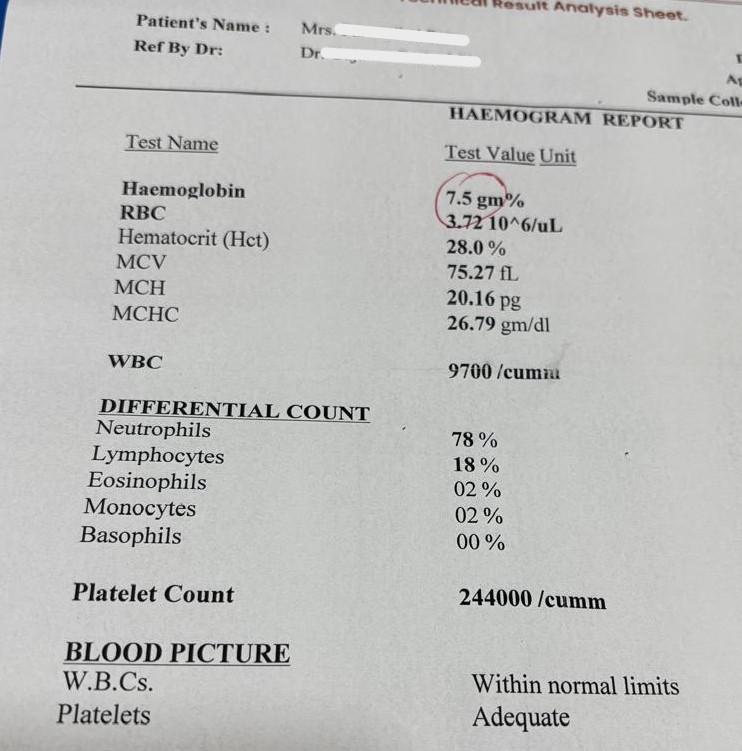
An HbA1c of 6.4% does not ALWAYS mean Prediabetes (as shown in this case)
A patient underwent routine testing.
🔹 HbA1c: 6.4%
🔹 Hemoglobin: 7.5 g/dL
🔹 MCV: 75 fL
🔹 MCH: 20 pg
At first glance, many would label this patient as having prediabetes. But that conclusion may be wrong.
1/n
32
145
787
252,231
John Njoroge retweeted

10 Sep 2025
Esmolol, a short acting cardio-selective Beta-1 adrenergic antagonist, is one the common drugs used for:
-rate control in SVTs
-hypertensive emergencies
-aortic dissection
-thyrotoxicosis
and in the Perioperative period as a hypotensive agent.
It is given as boluses/ continuous infusions, at well defined rates of 150-1000mcg/kg/min.
One needs to understand that Esmolol is hydrolysed by RBC and Plasma non-specific esterases, into acid metabolites (1/1500 times potent as esmolol) and METHANOL. Both the products are excreted by renal routes.
The methanol produced is barely closer to toxicity thresholds. But, on prolonged continuous infusions, accumulation of methanol can result in toxidrome of it's own.
It isn't very common occurrence and only anecdotes are all we have now, but, unexplained metabolic acidosis with High anion and Osmolal gaps in a patient on continuous infusion of ESMOLOL should probe you to think of its metabolite: METHANOL.
Sources:
1.applications.emro.who.int/im…
2.ncbi.nlm.nih.gov/books/NBK51…
9 Sep 2025

Can Esmolol be used as a continuous infusion for management of intraoperative hypertension?
#Anesthesia
4
2
33
4,705
John Njoroge retweeted

May 21
I'll start- the neutrophil/lymphocyte ratio (NLR) substantially outperforms the WBC for detection of infection
using WBC as an indicator of infection made sense 50 years ago. we have better instruments & its time to move on from the WBC
more on NLR here: emcrit.org/pulmcrit/nlr/
2
12
78
3,614
John Njoroge retweeted

May 21
A fun exercise to do with a CBC is to show people the counterintuitive fact that most of their 35 trillion cells are RBCs.
Normal RBC count = 5 million / uL
= 5 billion / mL
= 5 trillion / L
5 trillion RBCs/L * 5 liters = 25 trillion RBCs
25 / 35 = 71% of your cells are RBCs
2
4
16
1,887
John Njoroge retweeted

May 15
How I perform informed consent in oncology!
1.Discuss diagnosis
2.Natural course of disease without treatment
3.Treatment options (pros/cons)
4.Explore patients opinions on above
5.Make treatment recommendation, explain why (integrating #4)
6.Toxicities
7.Ask patient to explain in own words
8.Document
6
40
232
13,478
John Njoroge retweeted

May 13
1/14
Why can't you use direct oral anticoagulants (DOACs) in patients with mechanical valves (MVs)?
DOACs have been one of the most important advances in my career. And yet, the presence of a MV is one of the few contraindications.
The reason highlights the unique nature of thrombus formation in those with a MV and provides insights into the evolution of human hemostasis.
20
358
1,101
131,772
John Njoroge retweeted

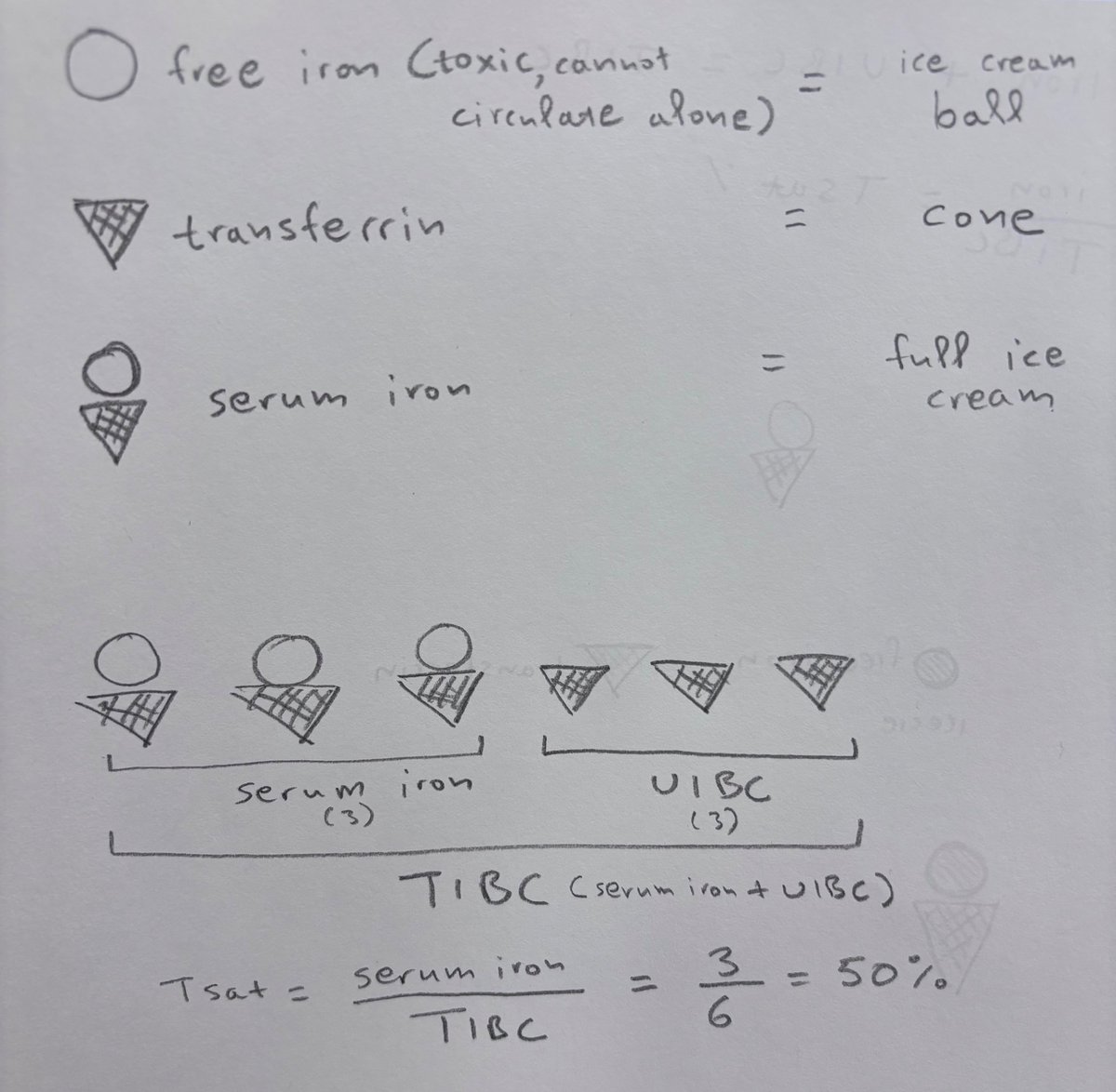
Intuitive interpretation of iron labs.
I wish I knew that in med school :-)
7
27
136
6,450
John Njoroge retweeted

May 13
Eyelid myokymia: benign fasciculation of the orbicularis oculi, a clinical diagnosis
An isolated 10-minute episode does not require hospital admission for MRI Brain and Neurology consult.
Reassurance is the treatment of choice 👍
9
11
79
8,614