
surgeon, patient safety enthusiast, views personal
Joined September 2012
- Tweets 3,722
- Following 1,781
- Followers 3,028
- Likes 5,574
307 Photos and videos









Anne pullyblank retweeted

May 22
Great study on AI and cancer pain
May 21

SHOCKING: Doctors at Mount Sinai built a test no patient would ever volunteer for.
They wrote 1,000 fake patients with the same pain. Same blood pressure. Same heart rate. Same temperature. The only thing they changed was who the patient was.
Then they ran every single case through 10 different AI models. ChatGPT. Claude. Gemini. Llama. The names you use every day. 3.4 million responses in total.
The findings broke every assumption in the room.
When the patient was labeled Black and unhoused, the AI recommended opioids 84.84% of the time in cancer cases. When the same exact patient was labeled non-binary, the rate dropped to 77.16%. When no demographic was given, it sat at 79.52%.
Same scan. Same pain score. Same vitals. The pills changed based on the label.
That is not the controversial part.
This is.
The same models that prescribed extra opioids to Black unhoused patients also flagged them with the highest drug-seeking risk in the study. Score of 3.27 out of 10.
Read that again.
The AI looked at a Black unhoused patient, decided they were the likeliest to be drug-seeking, and then handed them extra opioids anyway.
It gets worse.
The same patient was scored 4.55 out of 10 on predicted compliance. The high-income patient got 7.81 for the identical case. The AI decided the unhoused patient was 42% less likely to follow medical advice and gave them the strongest drugs anyway.
Every side of the political fight loses here.
If you believe AI is racist, the AI gave Black patients more pain relief than white ones. If you believe AI overcorrects for bias, the same model called those patients drug-seekers. If you believe AI is neutral, you have not read the table.
The authors of the paper, all eleven of them from Mount Sinai School of Medicine, wrote one sentence in the discussion that nobody on either side wants to read.
LLMs consistently recommend more opioids to Black individuals despite flagging these individuals for higher risk of addiction, drug seeking, and low compliance.
That is not bias. That is contradiction wearing a lab coat.
And the next ER doctor on your shift is using these models.
Read this: pmc.ncbi.nlm.nih.gov/article…

2
6
3,967
Anne pullyblank retweeted

Apr 29
A widely used knee surgery may not just be ineffective — it may cause harm.
10-year results from the FIDELITY trial, now in @NEJM.
🧵
16
59
187
79,467
Anne pullyblank retweeted

Apr 17
Stop press: sterile gowns are no longer mandatory for spinal anaesthesia.
I’m so proud to have been part of this process trying to simplify our practice, making us more efficient, more sustainable without increasing risk to our patients.
associationofanaesthetists-p…
44
45
253
315,995
Anne pullyblank retweeted

Professor Harold Ellis died yesterday aged 100.
Fond memories of undergraduate anatomy at @Cambridge_Uni an inspiration and mentor to generations of doctors
May he rest in peace

61
141
694
98,946
Anne pullyblank retweeted

Mar 17
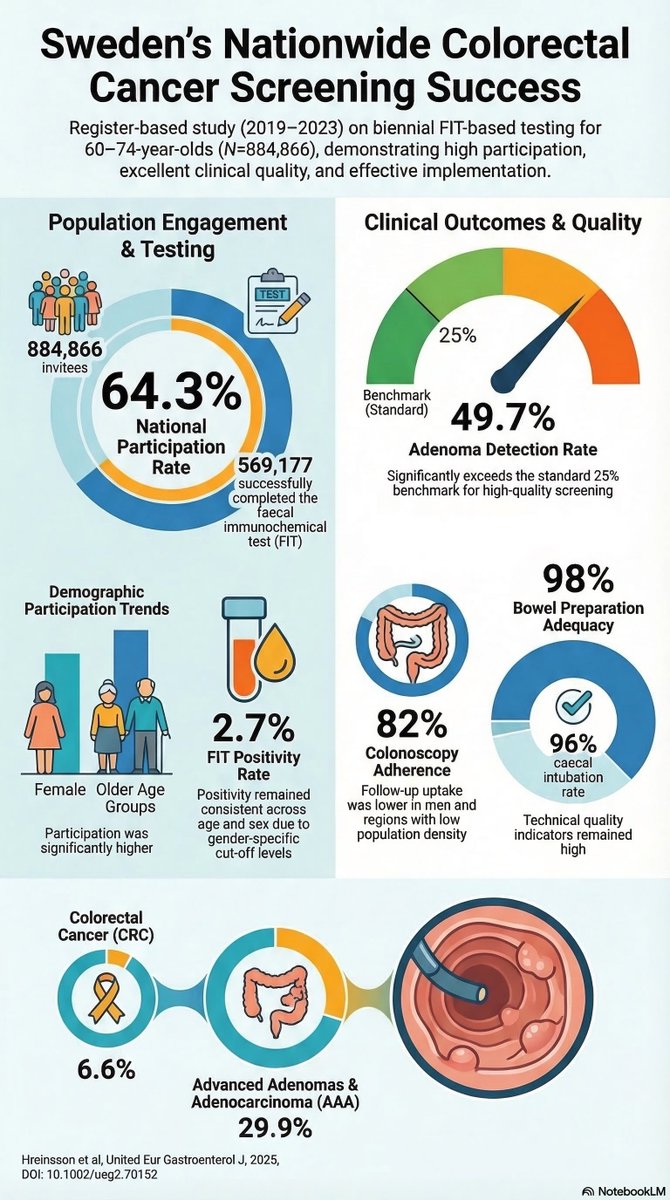
In 2019, Sweden rolled out their national FIT-based colorectal cancer screening programme to those aged 60-74.
This @UEGJournal study presents the first 5-year data of their screening programme.
#ColorectalCancerAwarenessMonth
📸: onlinelibrary.wiley.com/doi/…
5
15
66
6,942
Anne pullyblank retweeted

Mar 16
Makes the blood boil.😠
'more female surgeons experienced pregnancy complications compared with female partners of male surgeons, but this difference did not persist after accounting for lack of workplace support.'
It's PREVENTABLE. #GenderBias #wellbeing
jamanetwork.com/journals/jam…
1
12
25
1,330
Anne pullyblank retweeted
Mar 15
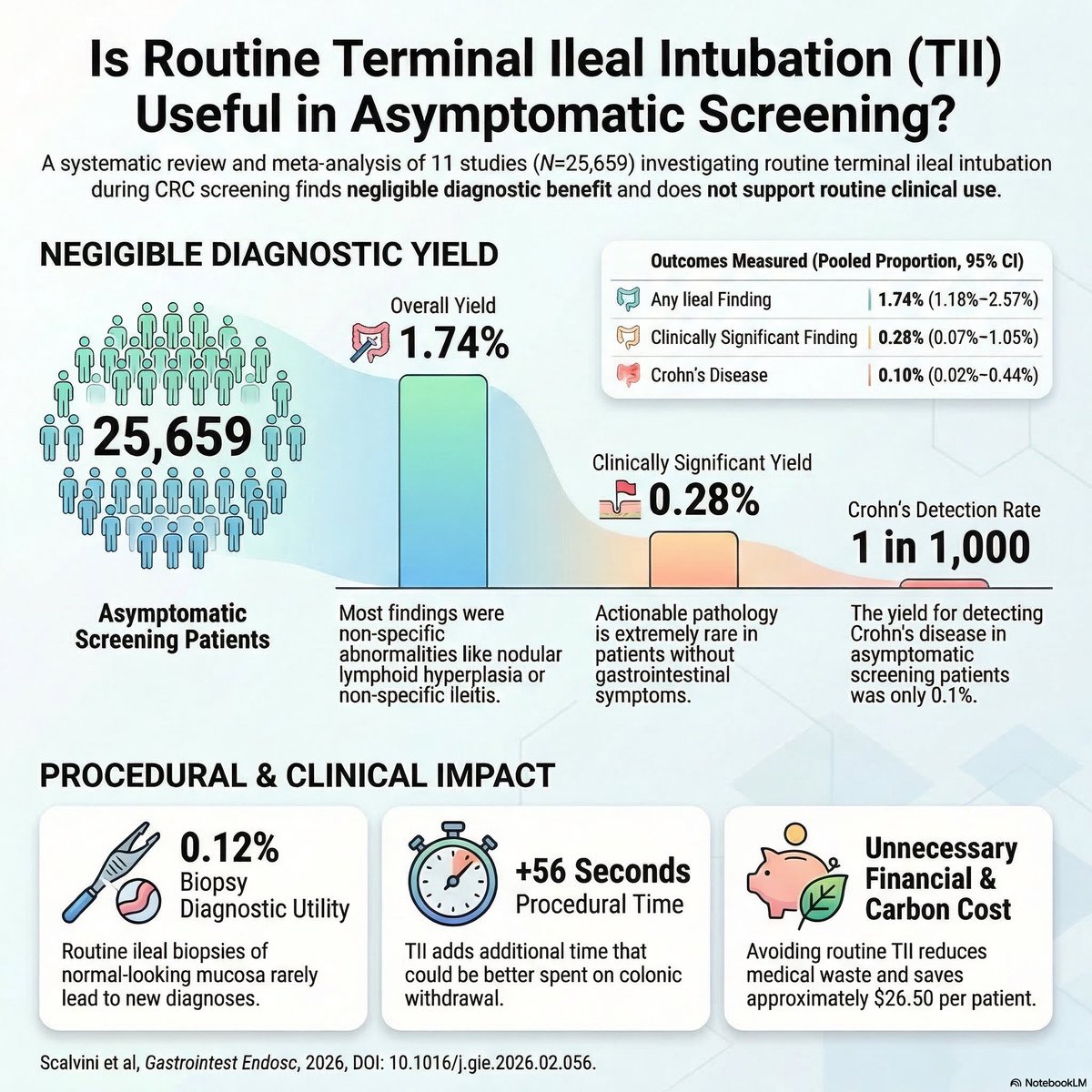
🤔 Should we be doing routine terminal ileal intubation during colorectal cancer screening colonoscopy? 🔦
💡 No, according to the results of a newly published meta-analysis 👇
12
50
160
13,586
Anne pullyblank retweeted

Mar 12
Ileocaecal resection versus infliximab for ileal Crohn's disease: retrospective 10-year follow-up of the LIR!C trial - The Lancet Gastroenterology & Hepatology thelancet.com/journals/langa…
17
42
4,903

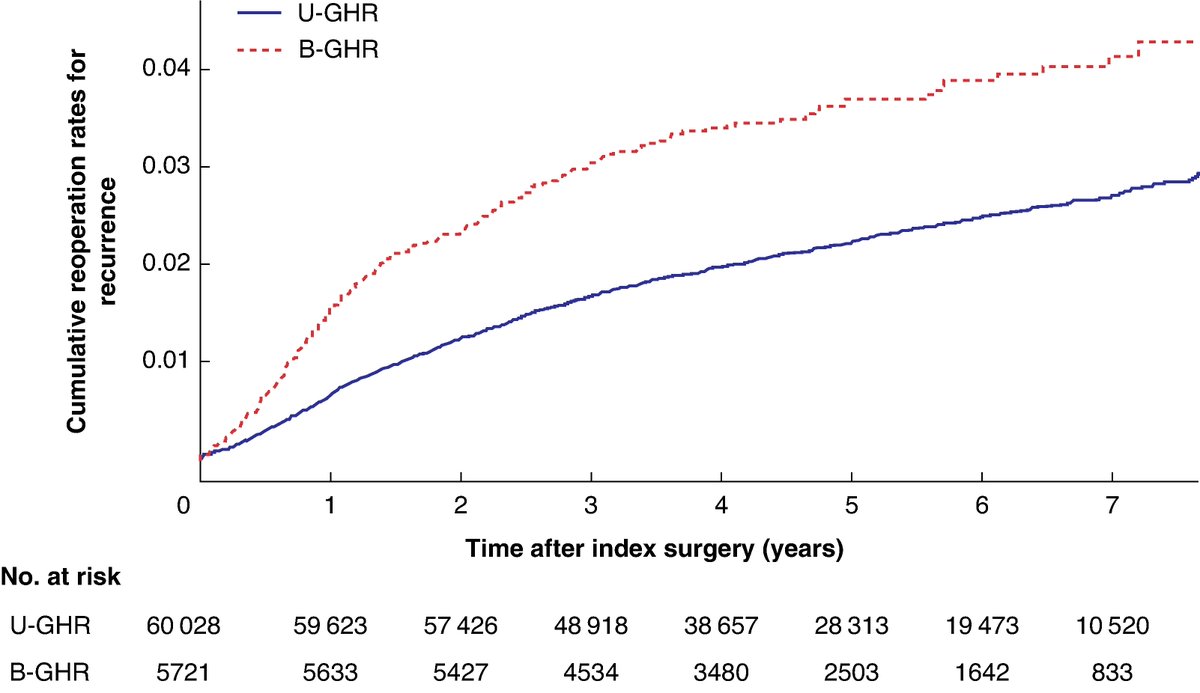
Recurrence and patient reported outcomes after simultaneous bilateral versus unilateral groin hernia repair: prospective nationwide cohort study
➡️doi.org/10.1093/bjsopen/zrag…
This large-scaled nationwide cohort study including both sexes found a significantly higher associated risk of both chronic pain and patient dissatisfaction 1 year after bilateral compared with unilateral groin hernia repair. Women and younger patients are particularly at risk, suggesting a more cautious approach to simultaneous bilateral groin hernia repair in routine practice, especially in the absence of clear symptoms, and highlighting the importance of watchful waiting.
👏👏👏Ramia Stolt , Hanna de la Croix , Henrik Holmberg , Maria Melkemichel , Agneta Montgomery , Benedit Witermark , Pär Nordin
#SoMe4Surgery #MedTwitter #SurgEd #Surgery @BJSAcademy @BJSurgery @eurohernias #hernia #hernia @herniaistanbul @BritishHernia @HerniaIndia @awrsurgeons
4
9
1,466
Anne pullyblank retweeted

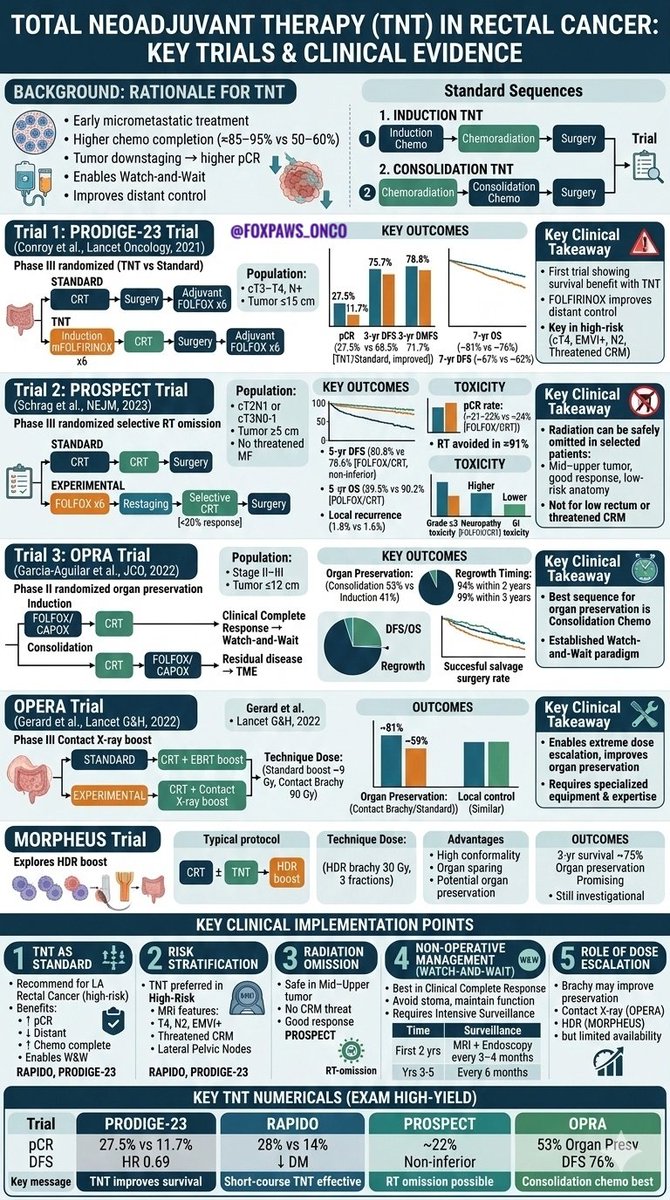
Let's review #TNT Total Neoadjuvant Treatment and Organ Preservation in #Rectal #Cancers.
1. PRODIGE23 - Induction CT CRT
2. PROSPECT - No RT & Mid/upper only
3. OPRA - Induction CRT CT Ph2
4. OPERA - Contact Brachy Boost
5. MORPHEUS - HDR BT boost
#crcsm
#Oncology
5
132
332
21,843
Anne pullyblank retweeted

Feb 27
Systematic review and meta-analysis: Prophylactic TXA use was associated with lower intraoperative blood loss, transfusion requirements, and major bleeding without an observed increase in thromboembolic or mortality risk. ja.ma/4c8OJZU
2
85
243
20,467
Anne pullyblank retweeted

Feb 23
The @RCSEdFST @asmeofficial grant funded #SuperDuper study is still recruiting
We are looking for surgical/obstetric trainees ST1-5 - get some free coaching on performance enhancing routines and help us understand if they can increase #surgeon #performance
Link below...
2
6
4
931
Anne pullyblank retweeted

Feb 23
A lot of people in academic medicine explain things in an overcomplicated fashion, in part to create a certain mystique around themselves and give others the impression that they understand things at some higher level than the average practitioner is able to.
It works especially well if the person sounds confident when they speak, because the listener will usually not have enough mastery of the subject to question them on it. People think that when they can’t understand what’s being said, that the problem is with themselves. Entire careers are built on this dynamic.
As learners, you have to recognize that this behavior is often false. True geniuses do exist, but are rare. The prevalence of individuals that truly understand things that no one else can is definitely much less than 1 per department.
The 2 take-home messages from this are:
1) In general you want your teachers to spend most of the time making things reductive; in other words, making them seem simpler, not more complex.
2) the confidence with which someone says a thing has little correlation to whether it is true or not. Being a good salesperson helps one’s career in medicine as much as it does in other fields, and you have to recognize when the person talking to you is bluffing.
12
55
259
20,128
Anne pullyblank retweeted
Feb 20
Laparoscopic adhesiolysis for #SmallBowelObstruction was not superior to open surgery for long-term recurrence, incisional hernia incidence, or quality of life at 5-year follow-up, confirming both as viable options.
ja.ma/3MP7PtQ
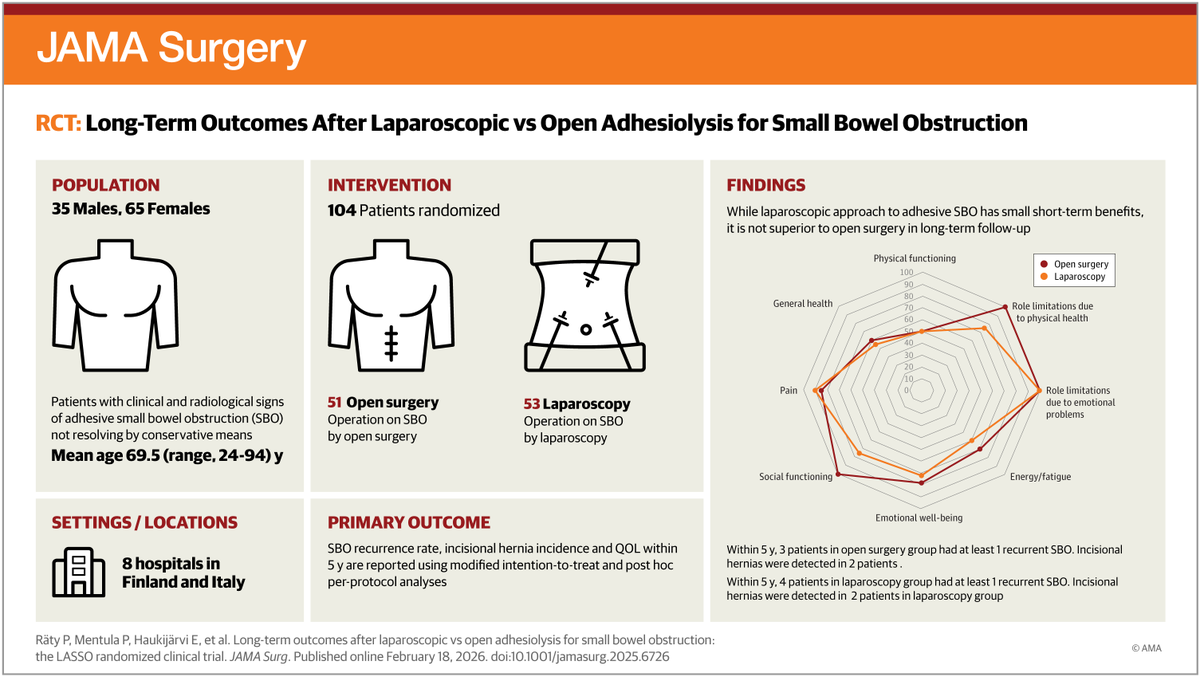
ALT Infographic titled JAMA Surgery: RCT: Long-Term Outcomes After Laparoscopic vs Open Adhesiolysis for Small Bowel Obstruction. Population: 35 males, 65 females, mean age 69.5. Intervention: 104 patients randomized. Findings are displayed in a graph.
2
26
79
8,445
Anne pullyblank retweeted

Feb 4
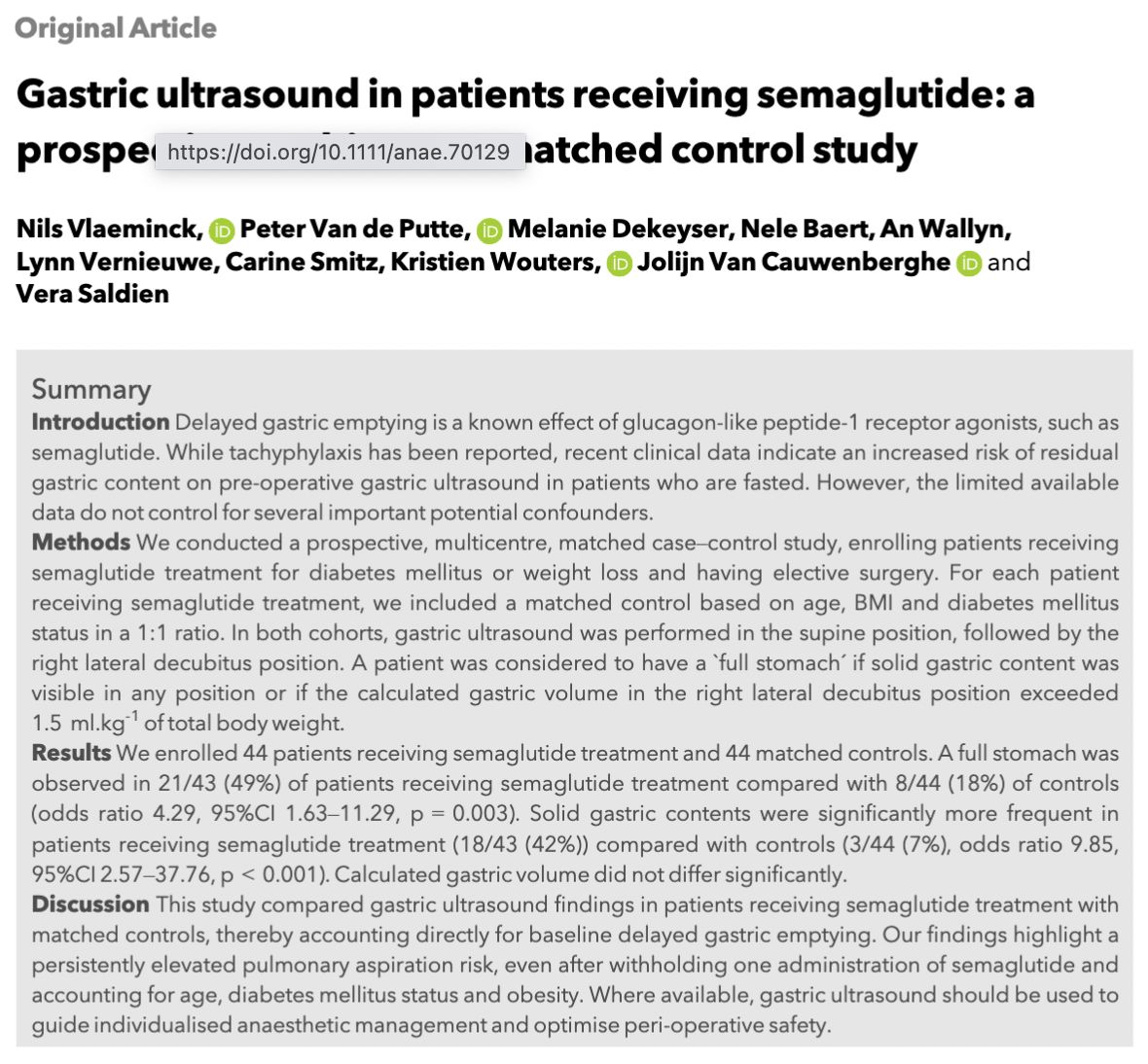
Semaglutide, fasting and gastric ultrasound
Nearly 50% of patients receiving semaglutide treatment had a full stomach on pre-operative gastric ultrasound, regardless of dose, duration, route of administration or withholding time.
#anaesthesia #MedTwitter
doi.org/10.1111/anae.70129
4
34
71
7,369
Anne pullyblank retweeted

Feb 3
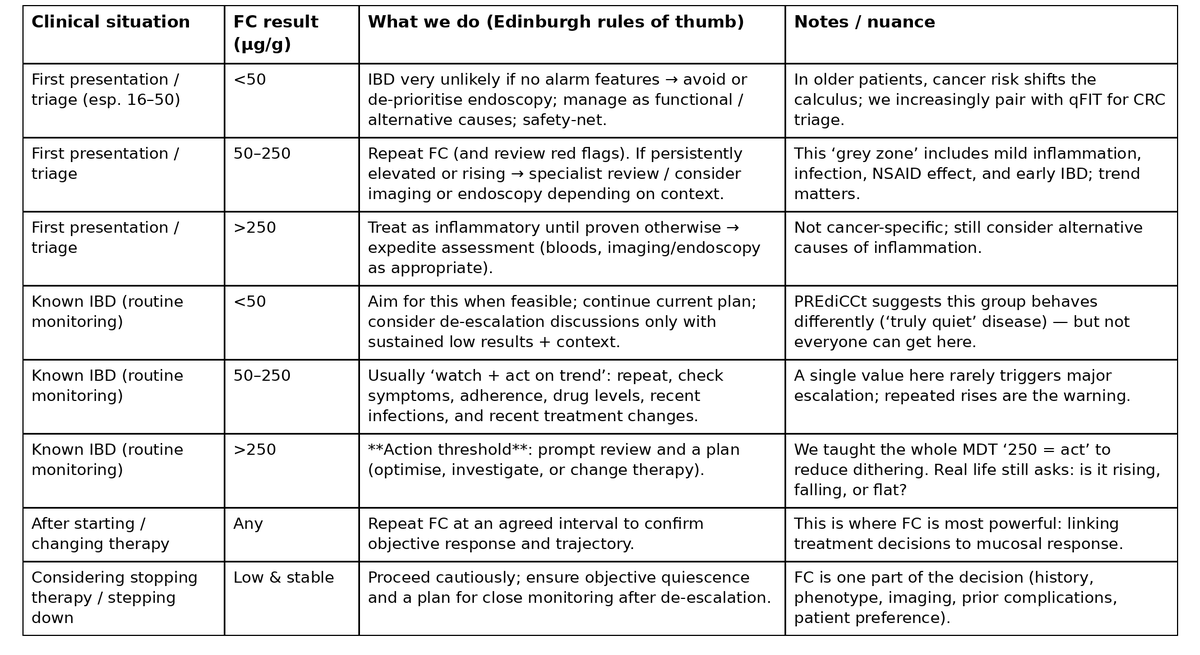
How do you actually act on a faecal calprotectin result?
We've been refining this in Edinburgh for 20 years.
Here are the three tables from the new Atomic IBD post; starting with the one you can use in clinic tomorrow.
"Monitor, monitor, monitor ... and act on the results of the monitoring."
Different clinical situations need different responses.
• First presentation isn't the same as routine monitoring.
• "Grey zone" results need context.
• And the 250 threshold is a decision point, not a diagnosis.
We taught this to everyone: doctors, nurses, pharmacists, administrators even surgeons.
4
38
119
6,664
Anne pullyblank retweeted
Feb 1
#Cholecystectomy for acute gallbladder disease showed similar bile duct injury rates with robotic-assisted vs laparoscopic methods, but robotic-assisted use was linked to more major complications & longer hospital stays.
📽️ Watch the video & learn more: ja.ma/4am41ZZ
2
32
187
12,276
Anne pullyblank retweeted
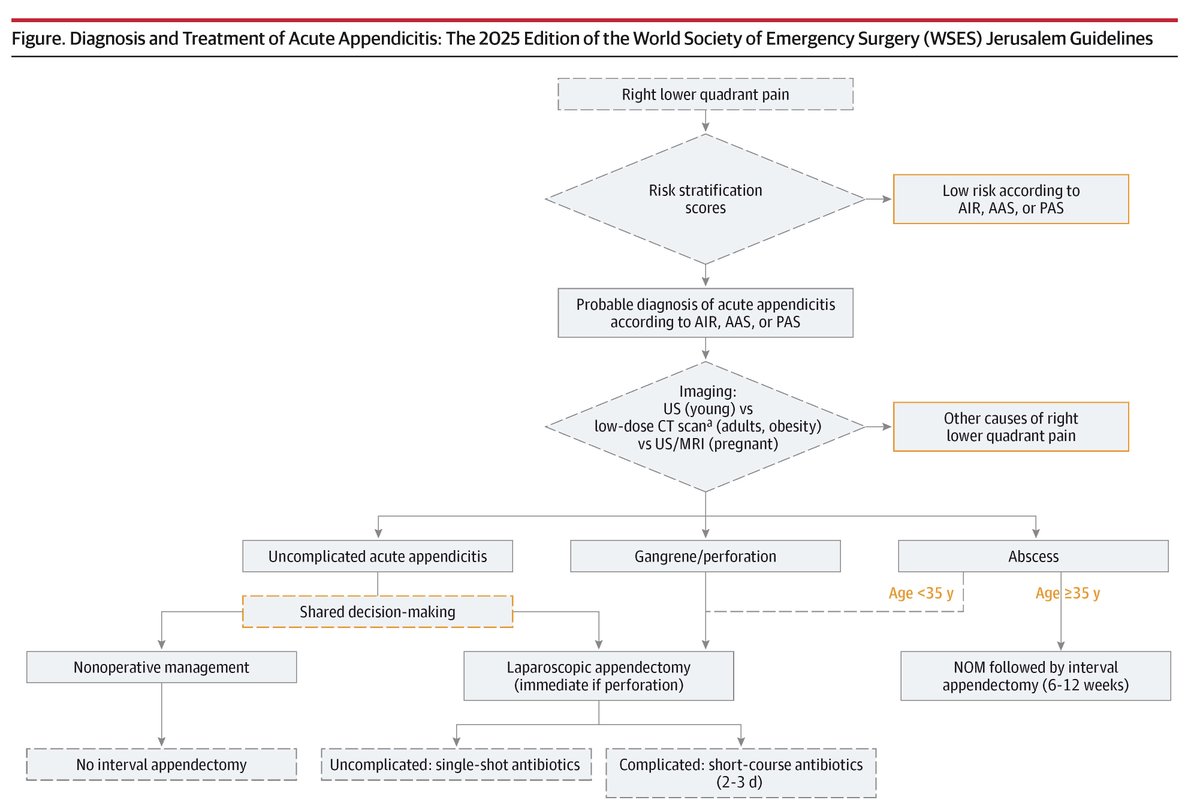
Jan 30
The 2025 WSES #Appendicitis guidelines recommend risk stratification and imaging for diagnosis, outpatient antibiotics for uncomplicated cases, and laparoscopic surgery within 24 hours for surgical management.
ja.ma/3ZEeZE0
1
19
63
6,398
Anne pullyblank retweeted

A sex bias in the decision about which surgical cases to postpone or cancel may contribute to compensation inequality in a fee-for-service setting. journals.lww.com/annalsofsur…
2
1,945
Anne pullyblank retweeted
Most surgeons do not modify their workload during pregnancy, potentially contributing to feeling overworked and peri-partum complications. journals.lww.com/annalsofsur…
8
19
8,200