
224 Photos and videos















Pinned Tweet

27 Dec 2025
2025 has been an amazing year for our family!
Some highlights:
✨Had a blast in Portugal 🇵🇹 for baby moon 🌙
✨The arrival of our 1st baby 👶🏼
✨ Matched at 1st choice for Advanced Imaging Fellowship 🩻
✨Aced Echo boards (95 percentile)
Looking forward to another great year!


5
3
128
16,732
Proud to share that I graduated from CVD Fellowship at @BCMHeart with the Outstanding Fellow in Academic Excellence Award. I’m incredibly grateful for the unwavering support of my wife and family throughout this journey. My dream of becoming a cardiologist has finally come true!


2
1
24
3,178


Jun 13
3 years flew right by with a blink of an eye! Today I’m a proud graduate of Cardiovascular Disease Fellowship at Baylor College of Medicine, Class of 2026 👨🎓
Jun 13

Wonderful evening for BCM CVD Graduation! 7 amazing fellows completed their journey in general cardiology. @GrahamRector @BryanTanMD @olamideMD @MVarugheseMD Maria Tinsay @WanLuxi @DrHaloot. Bringing together family, fellows and faculty across our 3 pavilions. Congratulations!!



3
20
2,180
May 26
Honored to received the Trainee Excellence Award 🏅from the Academy of Resident and Fellow Educators at @bcmhouston. I’m thankful to my wife & family, program director @arunima_misra and my mentors at @BCMHeart for their unwavering support in my career and in life 😇 #ACCFIT



6
5
63
5,467
Bryan E. Tan, MD retweeted

May 18
Special issue this week in @JNCjournal on cardiovascular imaging in amyloidosis!
Congratulations @mdicarli on putting together this essential guide for all things amyloidosis and to @premsoman123 for leading the paper we wrote on state of the art imaging with technetium-labeled tracers like PYP, DPD, HMDP.
sciencedirect.com/science/ar…
sciencedirect.com/journal/jo…

11
32
2,344
May 15
Thank you, Dr. Goyal! That was an incredible talk. Really enjoyed the discussion about Ikigai and growth mindset!
May 14

It was a privilege to share ideas with this extraordinary group of @bcmhouston fellows about "Finding Meaning, Fulfillment, and Financial Freedom in Medicine".
We discussed Ikigai, personal finance, joyfulness, the wheel of life, and so much more. Greateful to @DrHaloot & @arunima_misra for the invitation.


1
2
694
Bryan E. Tan, MD retweeted

Academic publisher Elsevier's profit margin compared to Apple, Google, and Microsoft
Apple: 28%
Google: 25%
Microsoft: 34%
Elsevier: 37% with a revenue of $3.9 billion.
Elsevier's payment to academic authors and reviewers: $0
64
919
3,487
198,775
Apr 26
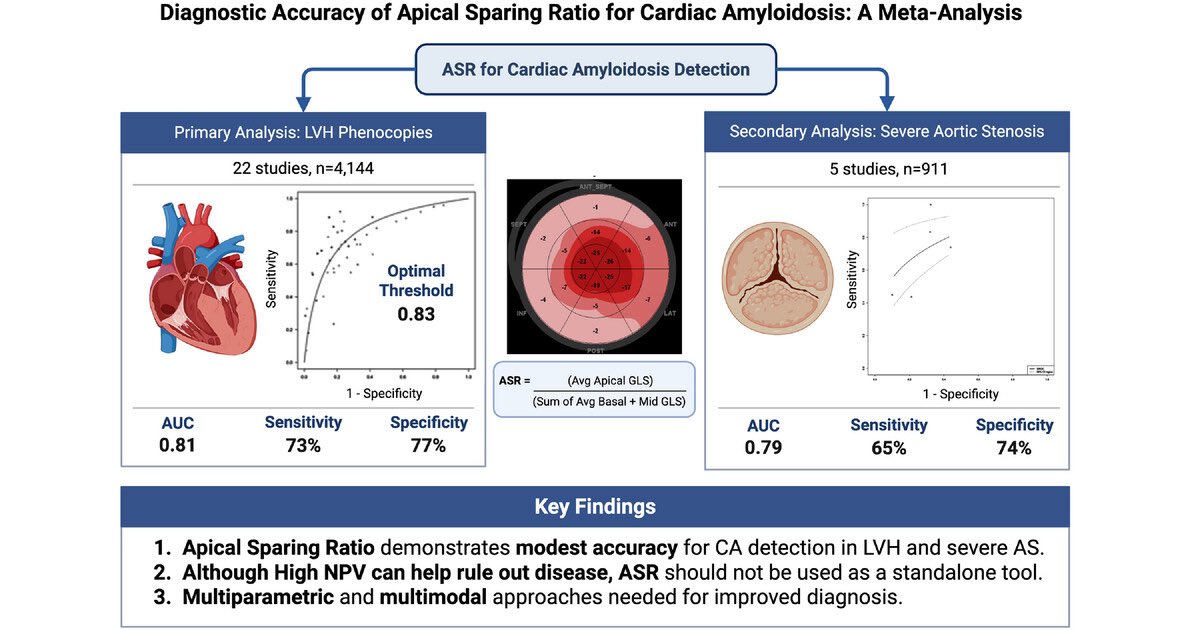
Hot off the press! 🔥🔥 Meta-analysis exploring diagnostic accuracy of ASR for 🫀 Amyloidosis now out in Echocardiography! Congratulations to all co-authors on this important work!onlinelibrary.wiley.com/doi/… @JSlivnickMD @UCCardsFellows @BCMHeart @BCMDeptMedicine @BCM_CVRI #ACCFIT
3
4
32
2,796
Bryan E. Tan, MD retweeted

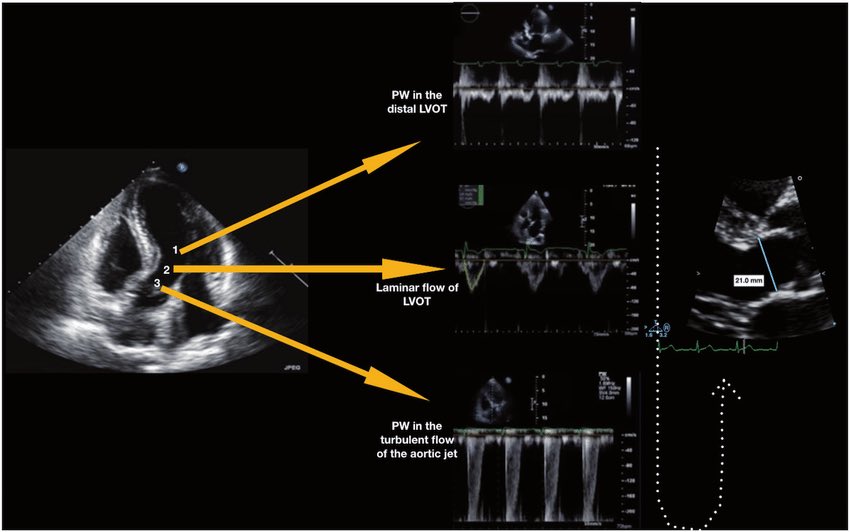
🫀 Did you know where the recommendation to place the pulsed wave Doppler sample volume 0.5–1 cm from the aortic valve to measure LVOT VTI comes from?
The answer is more interesting than it seems. It doesn’t come from a single study or an experiment designed for that purpose. It comes from a historical chain spanning nearly 40 years:
🔬 1982–1984 — The physical foundation
Pasipoularides and Murgo demonstrated using invasive catheters and mathematical models that in aortic stenosis there is a real zone of flow acceleration in the LVOT, just proximal to the valve, without any second anatomic obstruction. Pure hemodynamics — no Doppler yet.
👉 Bird et al. Circulation 1982 → doi.org/10.1161/01.CIR.66.4.…
👉 Pasipoularides et al. Am J Physiol 1984 → doi.org/10.1152/ajpheart.198…
📐 1984 — The apical 5-chamber view
Lewis, Kuo and Quinones were the first to validate cardiac output measurement using pulsed wave Doppler from the cardiac apex. They described placing the sample volume “immediately proximal to the aortic valve leaflets” — but without specifying any distance in centimeters.
👉 Lewis et al. Circulation 1984 → doi.org/10.1161/01.CIR.70.3.…
📏 1985 — The first numerical distance
Skjaerpe, Hegrenaes and Hatle (the Norwegian group) were the first to quantify this in Doppler: they empirically observed that flow acceleration began 0.5 to 1.5 cm proximal to the valve, and placed the sample volume just proximal to that zone. They directly cited Pasipoularides as supporting evidence. This was the first time a numerical distance appeared in the technique.
👉 Skjaerpe et al. Circulation 1985 → doi.org/10.1161/01.CIR.72.4.…
📊 1986–1988 — Practical consolidation
Otto et al. used ~1.0 cm. Oh, Tajik and the Mayo Clinic group explicitly established the range of 0.5 to 1.0 cm in 100 patients, justifying it as necessary to avoid the subvalvular acceleration zone. This is the figure we all recognize today.
👉 Otto et al. JACC 1986 → doi.org/10.1016/S0735-1097(8…
👉 Zoghbi et al. Circulation 1986 → doi.org/10.1161/01.CIR.73.3.…
👉 Oh et al. JACC 1988 → doi.org/10.1016/0735-1097(88…
📋 2002 — It becomes “official”
Quinones, Otto, Zoghbi and colleagues codified it in the ASE guidelines as “~5 mm proximal to the aortic valve”… but without citing any specific study to support it. It had already become expert consensus.
👉 Quiñones et al. JASE 2002 → doi.org/10.1067/mje.2002.120…
⚔️ 2017 — The debate reopens
Baumgartner et al. (EACVI/ASE) maintained the 0.5–1 cm recommendation. However, Hahn and Pibarot responded with a critical letter pointing out that the original articles from the 1980s measured at the aortic annulus, not 0.5–1 cm below it, and that moving away from the annulus introduces errors due to the elliptical and irregular shape of the subannular LVOT.
👉 Baumgartner et al. Eur Heart J Cardiovasc Imaging 2017 → doi.org/10.1093/ehjci/jew335
👉 Hahn & Pibarot. JASE 2017 → doi.org/10.1016/j.echo.2017.…
💡 Bottom line:
The 0.5–1 cm figure was never experimentally validated as the optimal distance. It emerged from empirical observations in the 1980s aimed at avoiding a flow acceleration zone that had been demonstrated with invasive catheters. It was adopted through accumulated clinical practice and later elevated to a formal recommendation by consensus. The debate over whether to measure at the annulus or 0.5–1 cm below it remains open to this day.
One of those recommendations we all follow but few know where it actually came from 🙂
Dr Benigno Valderrábano Salas
@MDBeni
@JaeKOh2 @ottoecho @WilliamZoghbi @ASE360 @EACVIPresident @NephroP @iamritu @PPibarot @hahn_rt @MAecocardio @SISIACOficial @SONECOM_AC @VazyurVasquez @Cardiotweets83 @HEARTof_echo @echobasics
17
133
411
54,332
Bryan E. Tan, MD retweeted

Especial médicos🩺⚕️🏥👨🏻⚕️👩🏻⚕️.
Os dejo esta carta en JAMA. Se la pondré a mis alumnos en la próxima clase:
He elegido estas frases :
👇🏻⏰
«La medicina puede tener un significado extraordinario. Pero no puede sustituir el estar presente en tu propia vida. El mundo puede necesitarnos como médicos. Pero las personas que nos aman nos necesitan como nosotros mismos. Y ese es el rol que nadie más puede llenar.»
«La residencia refuerza la lección de que las instituciones están diseñadas para perdurar más allá de los individuos. En cambio, las familias no.»
«Creo en formar a la próxima generación. Creo en el significado de este trabajo. Lo que ha cambiado es mi disposición a absorber el desgaste sin cuestionarlo.»
«Ya no estoy dispuesta a seguir posponiendo la vida. La medicina exige mucho. Y nosotros damos profundamente. Pero no puede tomarlo todo.»
«El significado de mi trabajo es profundo. El significado de mi presencia en casa es irremplazable.»

42
1,681
3,792
217,597
Bryan E. Tan, MD retweeted

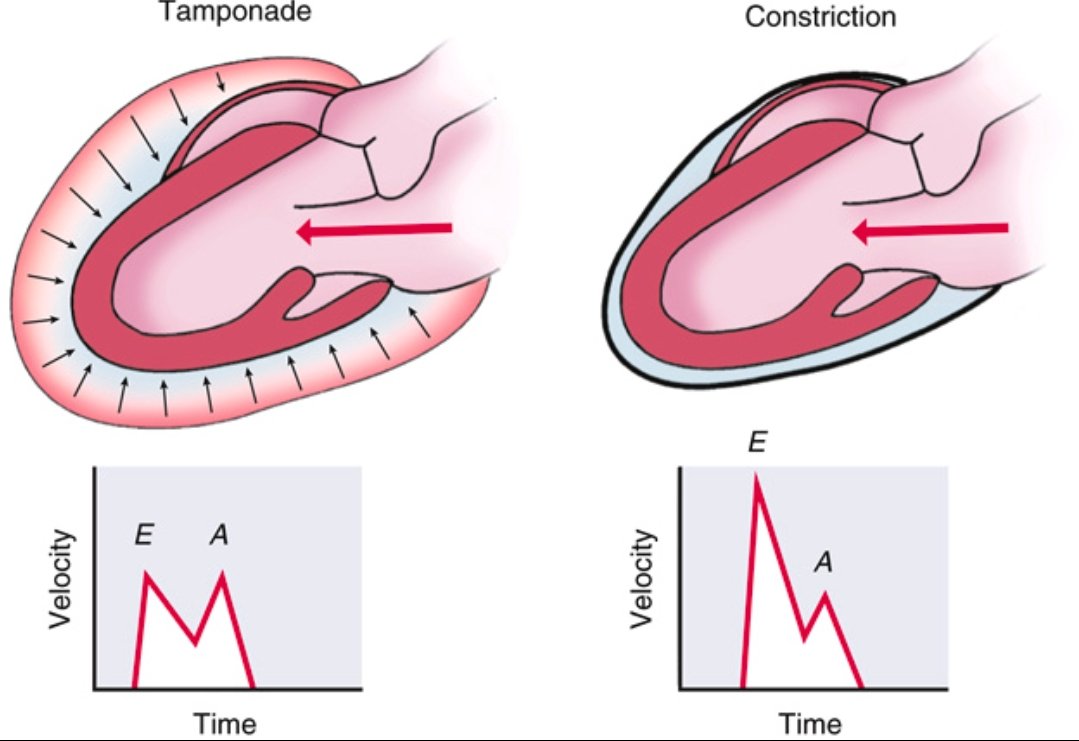
Pericardial Tamponade vs Constrictive Pericarditis ➡️Spot the Difference
Tamponade
⬇️
Accumulation of fluid in the pericardial space
⬇️
↑ intrapericardial pressure
⬇️
impairs diastolic filling throughout the cardiac cycle (early and late diastole).
Doppler shows blunted E and A waves due to restricted filling.
Constrictive Pericarditis
⬇️
Thickened, non-compliant pericardium
⬇️
rapid early diastolic filling that abruptly halts once volume limit is hit.
Doppler shows prominent E wave, reduced A wave, classic for constriction.
Recognizing the echocardiographic filling patterns is essential for diagnosis.
Ref: Catherine M. Otto, Textbook of Clinical Echocardiography
1
69
235
11,855
Bryan E. Tan, MD retweeted

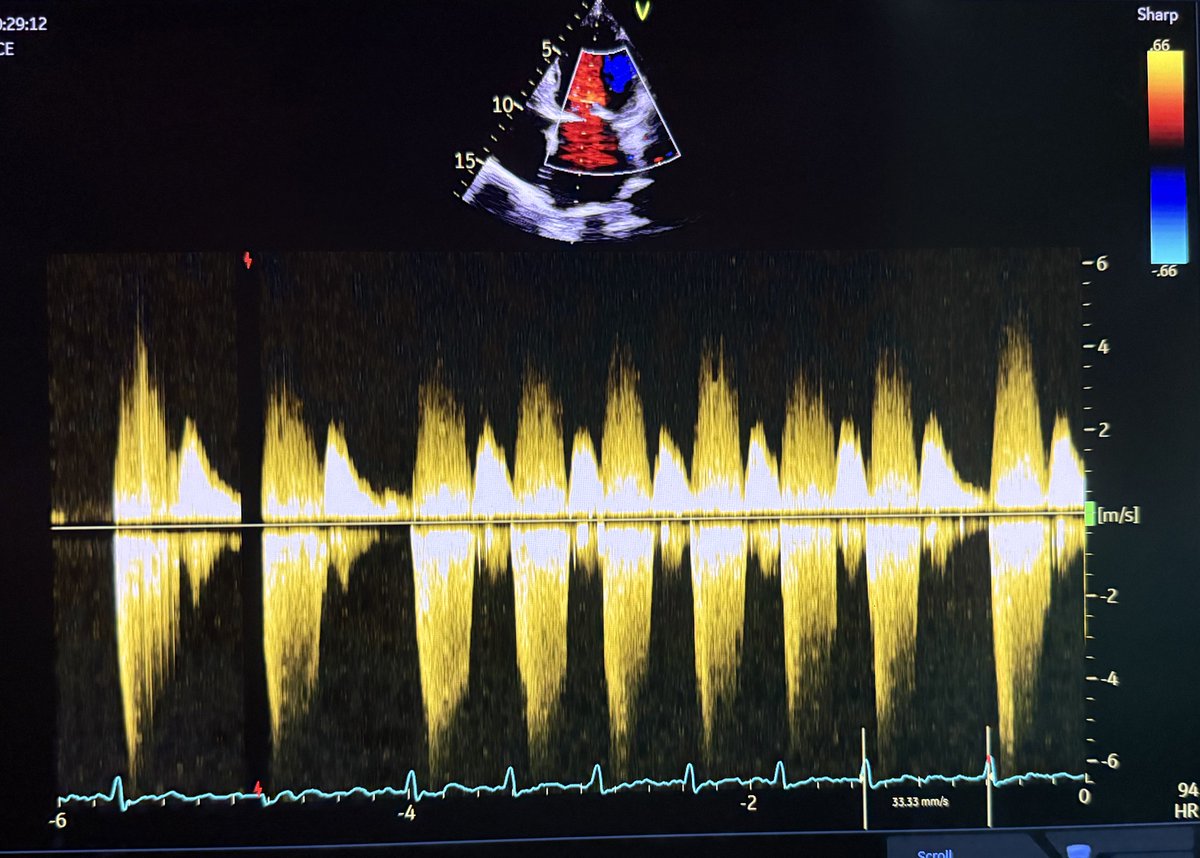
CWD through mitral valve in a patient with mitral regurgitation is shown. Why the MR signal is seen both above and below the baseline in CWD? @argulian @CASivaram1 @iamritu
9
13
70
11,815
Bryan E. Tan, MD retweeted

12 Apr 2024
Interesting #echofirst image. Looks like a pleural effusion (but it's not)!
🔗cvcasejournal.com/article/S2…
#POCUS #FOAMed #FOAMcc
2
68
260
25,529
Bryan E. Tan, MD retweeted

Apr 6
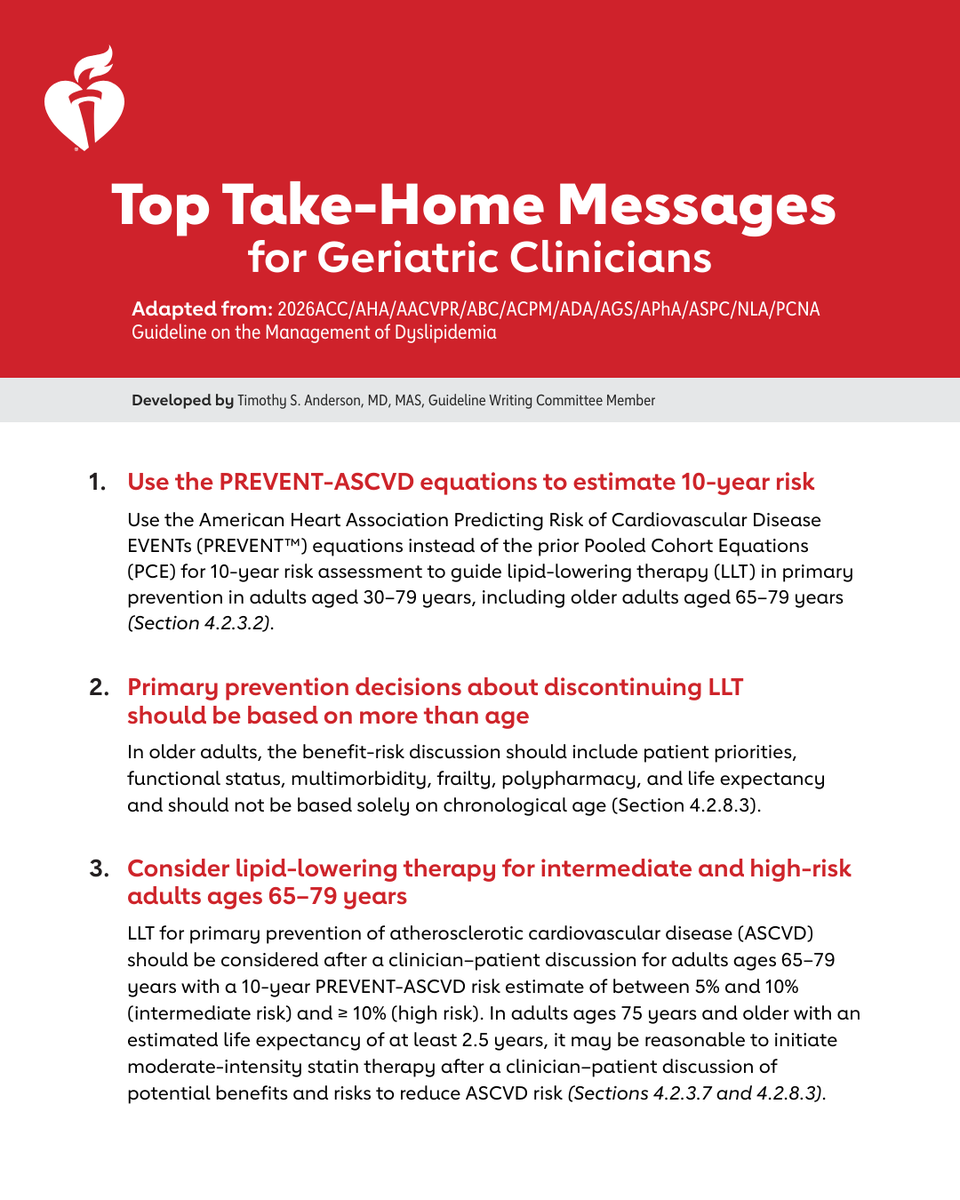
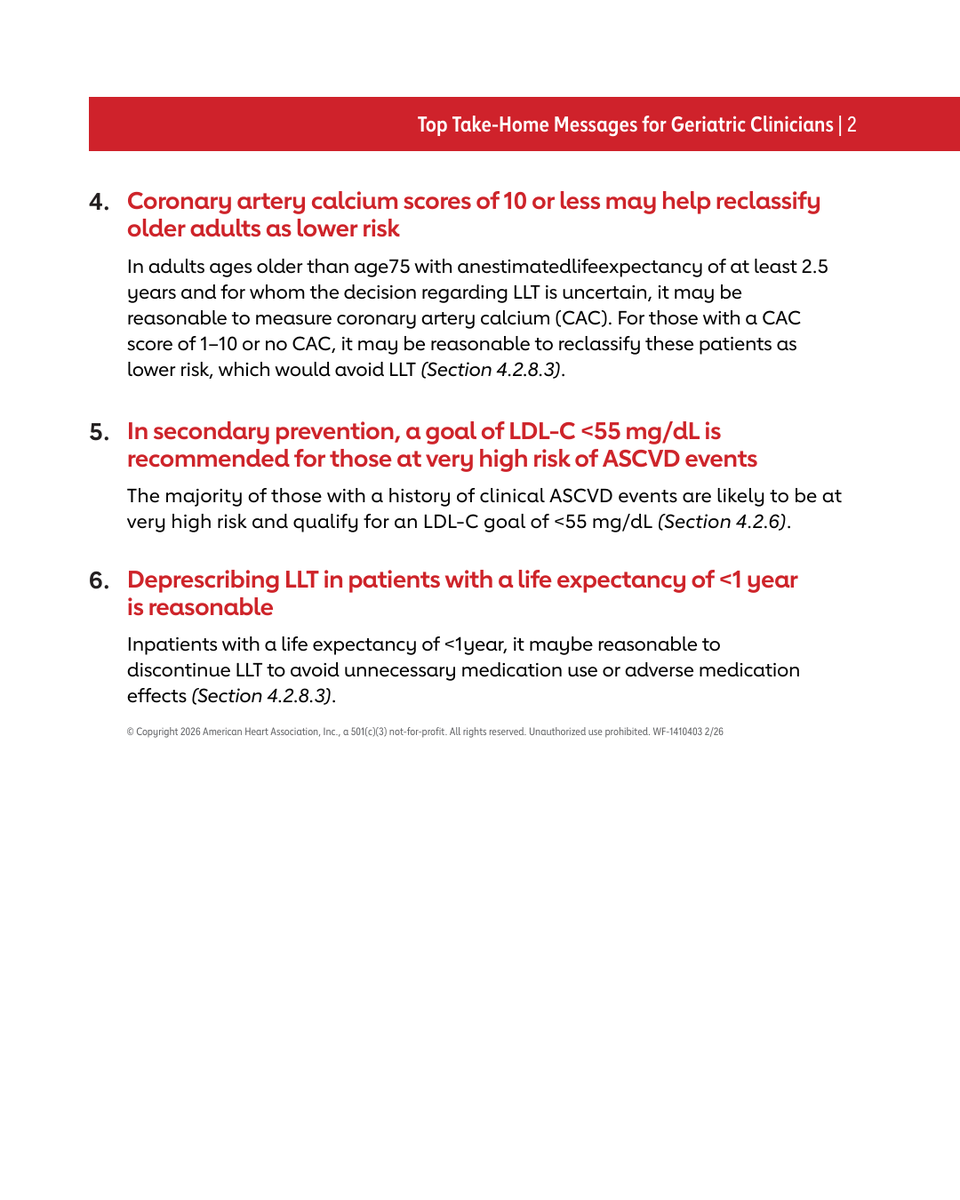
The 2026 Guideline on the Management of Dyslipidemia was recently published. Here are the top things for geriatric clinicians to know.
3
85
240
17,424
Bryan E. Tan, MD retweeted

Apr 3
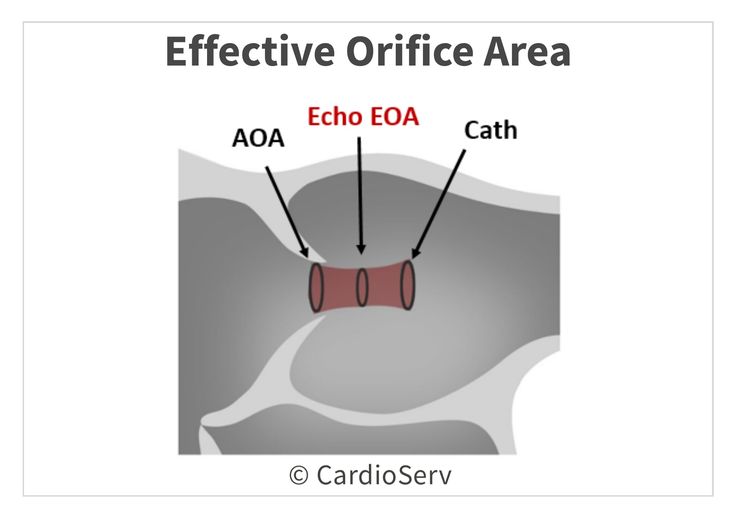
Anatomic vs Effective orifice area of aorta
■ AOA (Anatomic Orifice Area)
▪︎ The true anatomical opening of the valve (largest area).
▪︎ Measured directly by imaging (e.g., planimetry).
■ Echo EOA (Effective Orifice Area by echocardiography)
▪︎ The functional orifice where blood actually flows.
▪︎ Located at the vena contracta (narrowest flow region).
▪︎ Smaller than AOA due to flow convergence and contraction.
▪︎ Calculated using the Continuity Equation.
■ Cath (Catheter-derived valve area)
▪︎ Measured invasively using pressure gradients.
▪︎ Based on the Gorlin Equation.
▪︎ Typically slightly different from Echo EOA due to flow assumptions and hemodynamics.
🧠 Clinical Pearl:
Echo EOA is the most clinically relevant for grading severity (e.g., in Aortic Stenosis).
Always interpret values in context (flow state, gradients, LV function).
👉 In short:
“What matters is not how big the hole looks, but how much blood can actually pass through it.”
22
86
4,641
Bryan E. Tan, MD retweeted

Mechanism of diastolic mitral regurgitation in complete heart block
pmc.ncbi.nlm.nih.gov/article…
2
45
145
10,495
Mar 28
Representing @BCMHeart at ACC 2026 in NOLA. This is my first and last ACC during cardiology fellowship! 🫀🫀

2
4
28
1,884
Bryan E. Tan, MD retweeted

Mar 12
⚠️ Important concept
In 2025 ASE Diastology Guidelines, “LV filling pressure” generally refers to mean LAP or its correlates:
🔹 Mean PCWP
🔹 Mean LAP
🔹 LV pre-A pressure
But LVEDP and LAP are not the same.
✔️ Elevated LAP → elevated LVEDP
❗ Elevated LVEDP can occur with normal LAP in early diastolic dysfunction.
#ASEchoJC #EchoFirst @ASE360
1
9
25
4,927