
Joined April 2018
- Tweets 1,521
- Following 3,076
- Followers 2,333
- Likes 20,474
618 Photos and videos
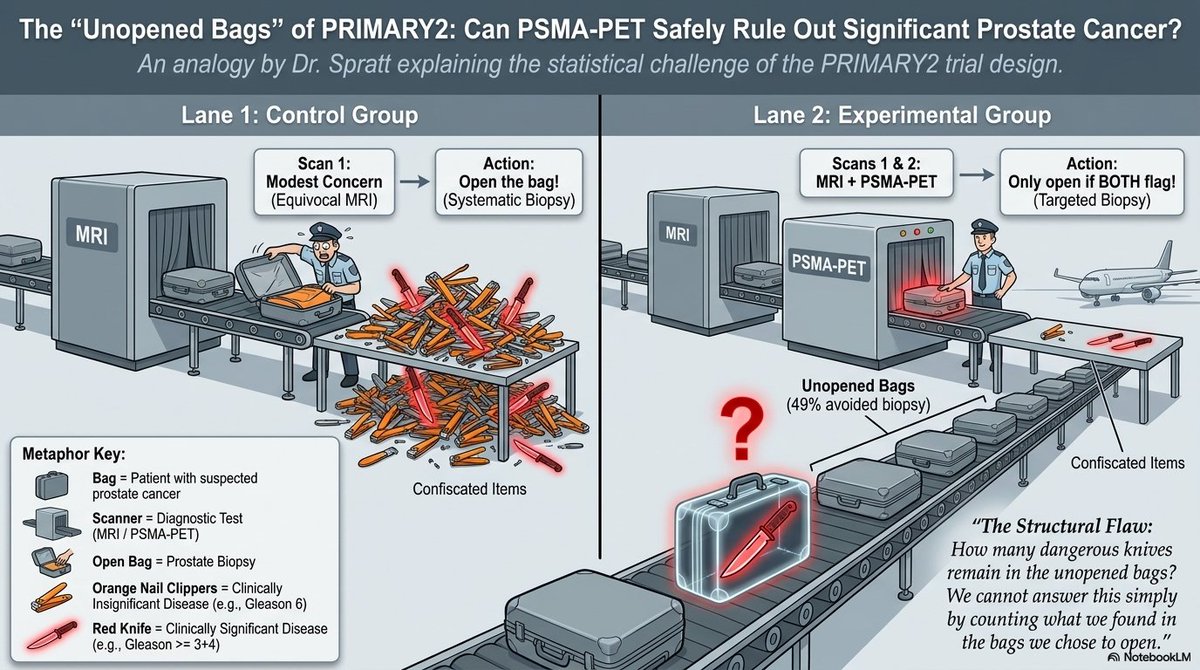




In @DrSpratticus editorial accompanying the PRIMARY2, there is a very effective metaphor that prompts us to pause before claiming that these data can already be considered a paradigm shift. A longer follow-up is needed for patients managed through the PSMA PET–based path. #radonc
1
7
20
1,813
A bit rough around the edges, but it effectively conveys the importance of the PRIMARY2 study in press on #radonc @TheLancetOncol @NotebookLM
5
9
893
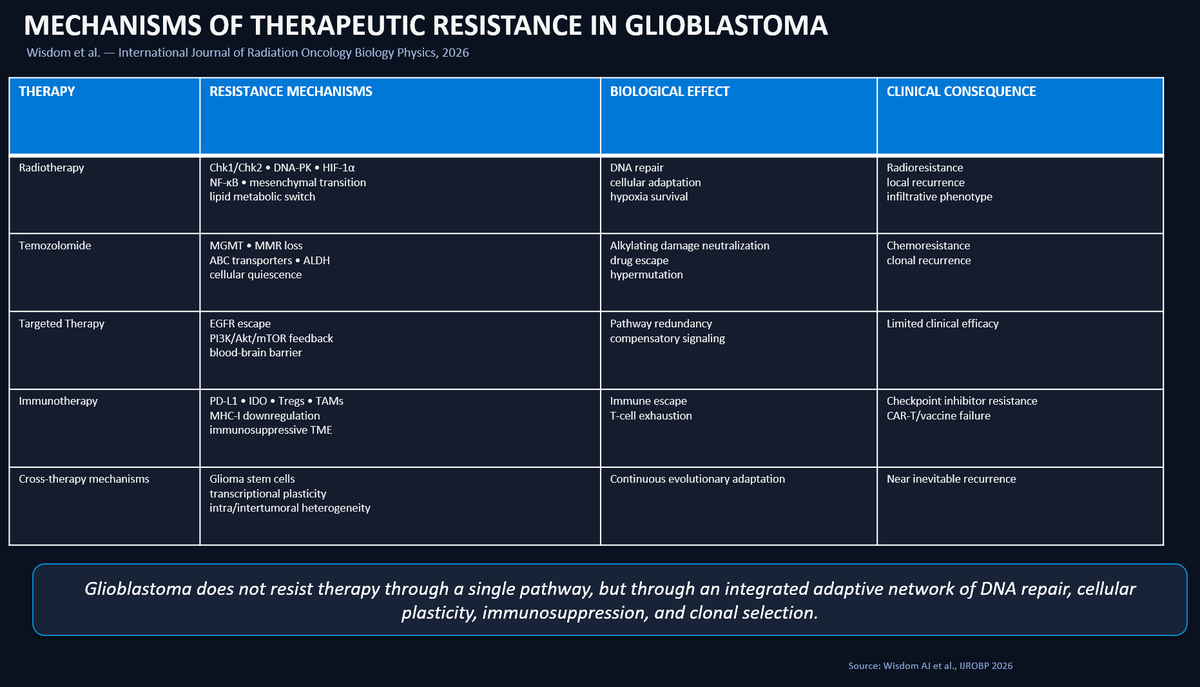
Very deep review in press in @IJROBP about mechanism of resistance in #Glioblastoma (@AmyWisdom8 et. al DOI :doi.org/10.1016/j.ijrobp.202…) .This table provides an at-a-glance overview of the main resistance mechanisms discussed in the paper. #radonc
1
12
31
2,240
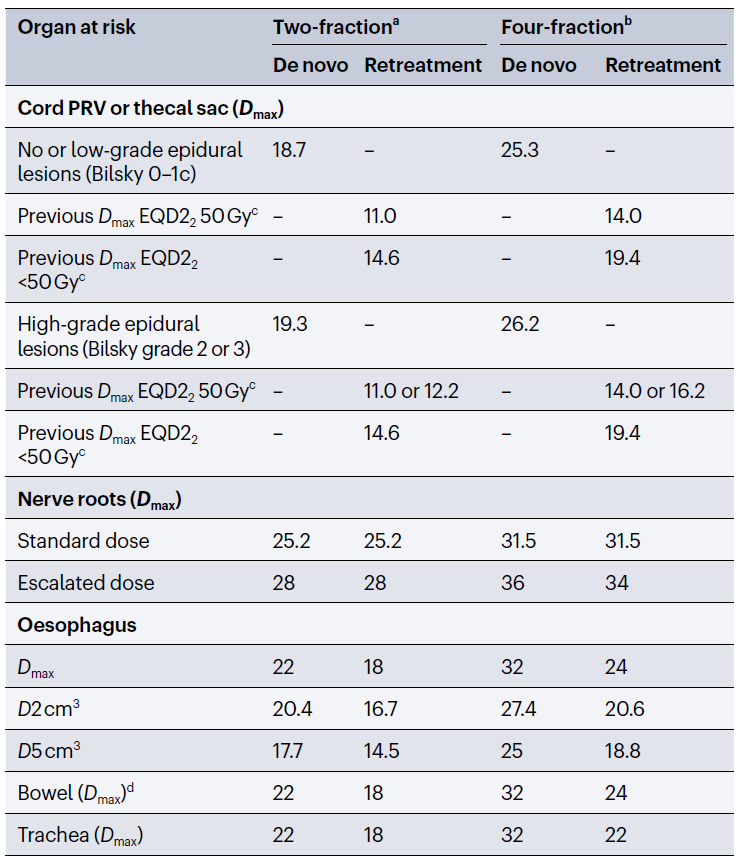
More than a review: a mini-treatise on spinal oncology.
Two crucial lessons for #radonc:
• SBRT patient selection must be driven by SINS stability criteria;
• the thecal sac may represent a “natural PRV” for spinal cord constraints.
Outstanding clinical insights !
1
15
51
2,552
We should stress the need to implement an intelligent strategy for spinal cord constraints, considering a safety structure that the Sunnybrook school identifies with the thecal sac — essentially a sort of natural PRV.
3
175
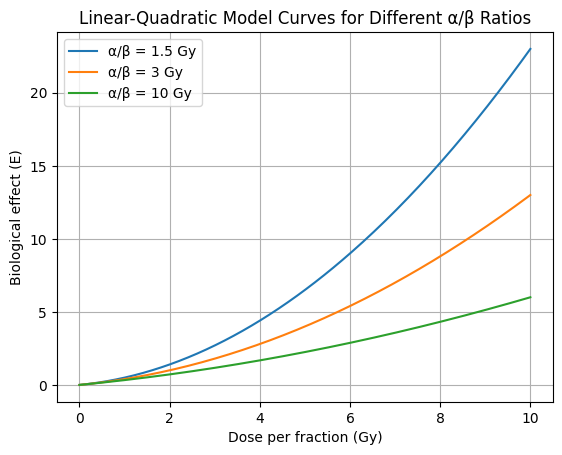
What is the real α/β in Prostate Cancer?
In this meta-analysis in the 🟢 Journal on regard BRFS :
α/β = 1.5 → no correlation
α/β = 3 → everything changes (R² 68%)
Practical translation : we don't know the real α/β value
#radonc
3
24
61
4,423
EQD2 captures dose, not biology. And modern RT is increasingly biological with not homogeneous dose distributions. There are many things these curves are unable to catch. α/β = 1.5 should give us a better BRFS with hypo schemes,but this meta-analysis data don't demonstrate it.
1
6
337
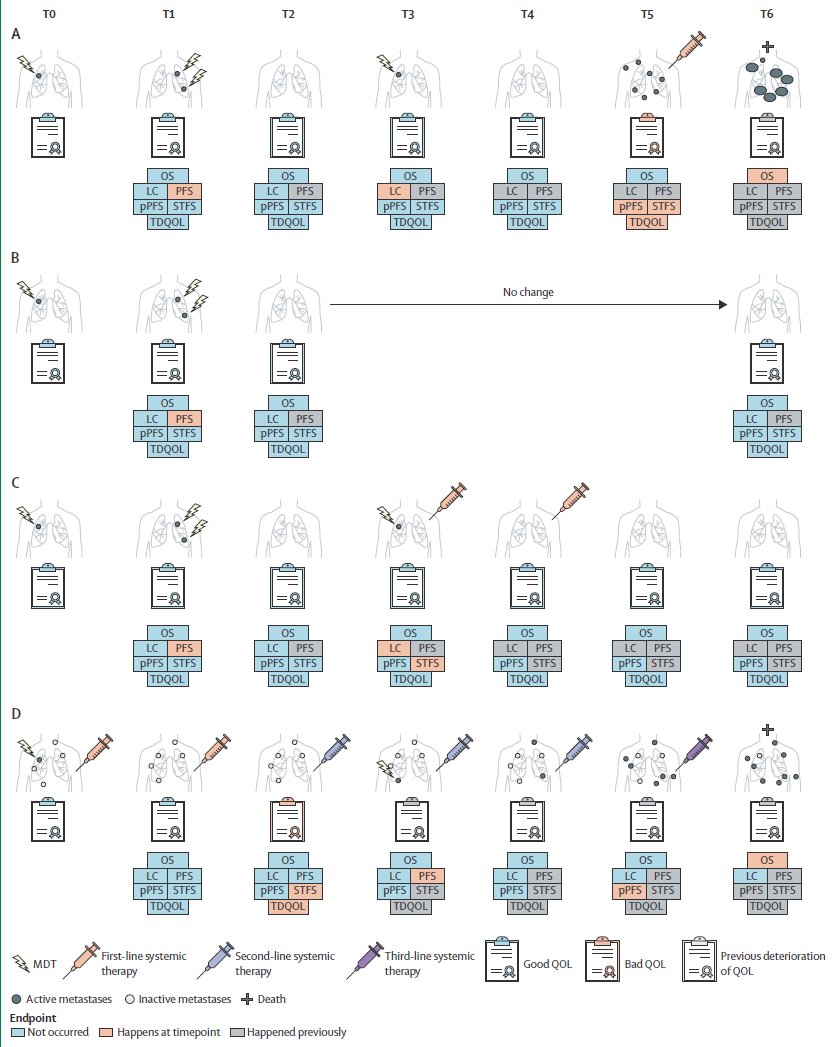
In OMD, traditional endpoints are no longer enough.
PFS ≠ failure of MDT.
We need endpoints that reflect clinical reality:
👉 STFS = time without systemic therapy
👉 pPFS = transition to widespread disease
👉 QoL = the patient’s lived experience
#radonc @TheLancetOncol
1
4
6
416
MDT doesn’t interrupt the natural history—it reshapes it.
Our endpoints should capture that.
Kudos to the authors for this thoughtful papepr
1
87
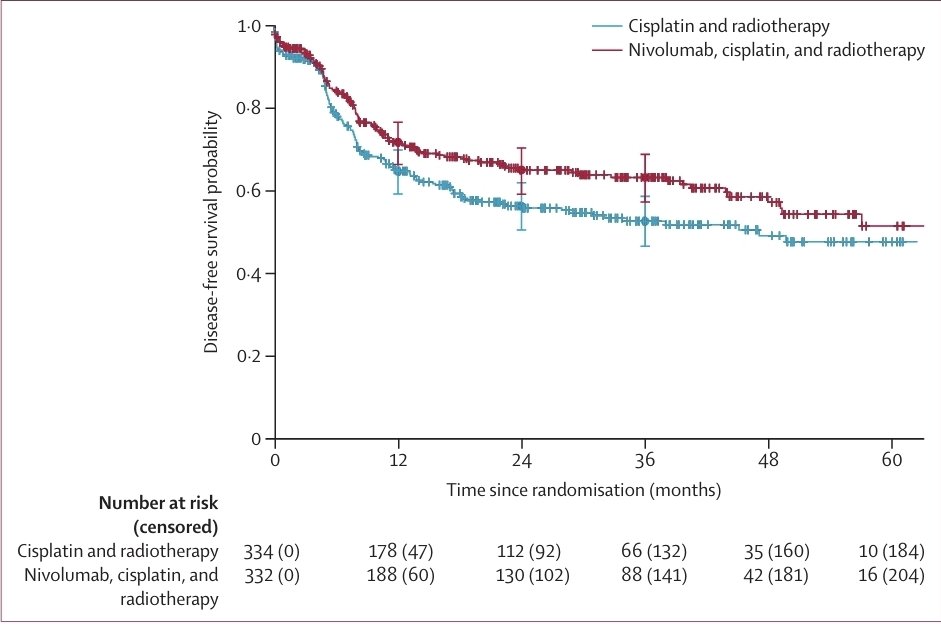
What about supportive care with corticosteroids for these patients in the concomitant setting 🤔. Coud this affect the efficacy of Nivolumab; is there a precise threshold of steroids that investigators permitted to use? Any author around ? #radonc
1
1
234

6 Dec 2025
A symptomatic vertebral hemangioma treated with decompressive laminectomy stabilization post-op RT (45 Gy/25 fx).
Excellent MRI response and recovery from paraparesis—another reminder of the value of RT in select benign conditions. #radonc ⚡



1
5
520
30 Nov 2025
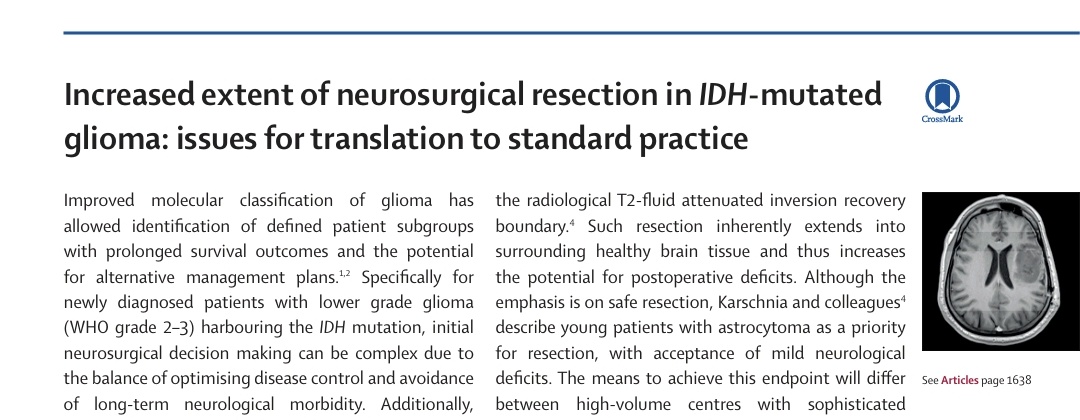
The new RANO resection classes redefine IDH-mutant grade 2 gliomas: every cm³ of residual tumor reshapes prognosis. Supramaximal surgery isn’t just technique — it’s biology. @TheLancetOncol
#radonc
1
4
17
990
30 Nov 2025
This figure tells the whole story: in IDH-mutant grade 2 gliomas, every cm³ matters. Residual T2-FLAIR volume shows a clean, continuous HR gradient — and supramaximal resection stands apart with striking survival separation.
1
3
205
30 Nov 2025
The accompanying editorial adds a layer: supramaximal surgery may change biology, but its real-world impact depends on anatomy, expertise, and system-level quality. A powerful reminder that maximal resection is not just evidence — it’s context, capability, and responsibility.
2
164
9 Nov 2025
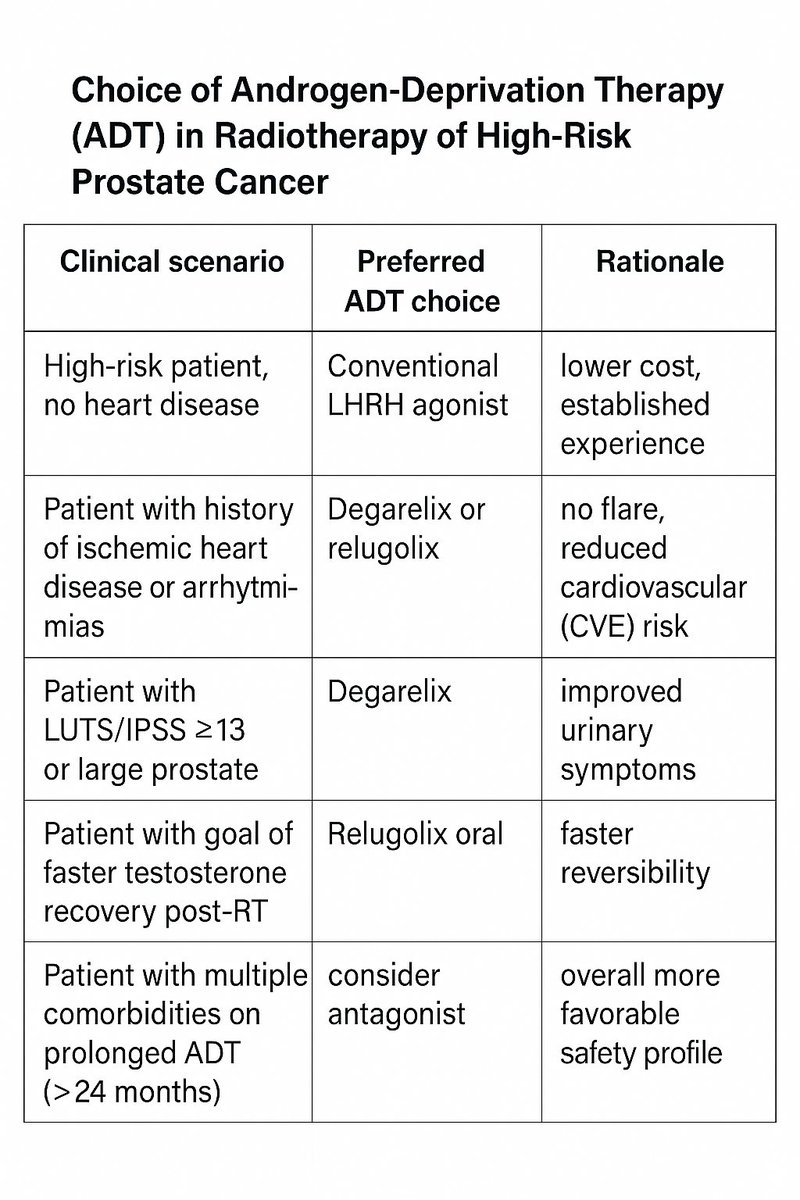
The EORTC GUCG-1414 study (@ZilliThomas et al., Eur Urol Oncol 2025) represents an important contribution—though with structural limitations—to the understanding of the clinical impact of different types of androgen deprivation therapy combined with radiotherapy in very high-risk or locally advanced prostate cancer.
The following table provides a concise and pragmatic synthesis that may be useful in daily clinical practice.
9
533
1 Nov 2025
Every ray that illuminates can also burn.
Every instrument of healing can become a weapon.
What saves, if used without measure, destroys.
And yet, for more than a century, light has remained our ally.
We have learned to modulate it, to measure it, to give it form.
Sometimes it enters the body like an invisible blade; at other times, it moves around the tumor like a breath of energy.
It is the same light that once burned in Grubbe’s hands — the same that made Edison’s bulb shine — and that now flows silently through the bunkers of radiotherapy, within the precise beams of the accelerators.
There is no contradiction here, but a paradox:
radiation kills, and precisely for that reason it can heal.
As if life, in order to continue, had to learn to live with its own opposite.
It is on this fragile, luminous frontier that medicine and physics meet.
And in that meeting — between measure and abyss — hope still shines.
2
208
12 Oct 2025
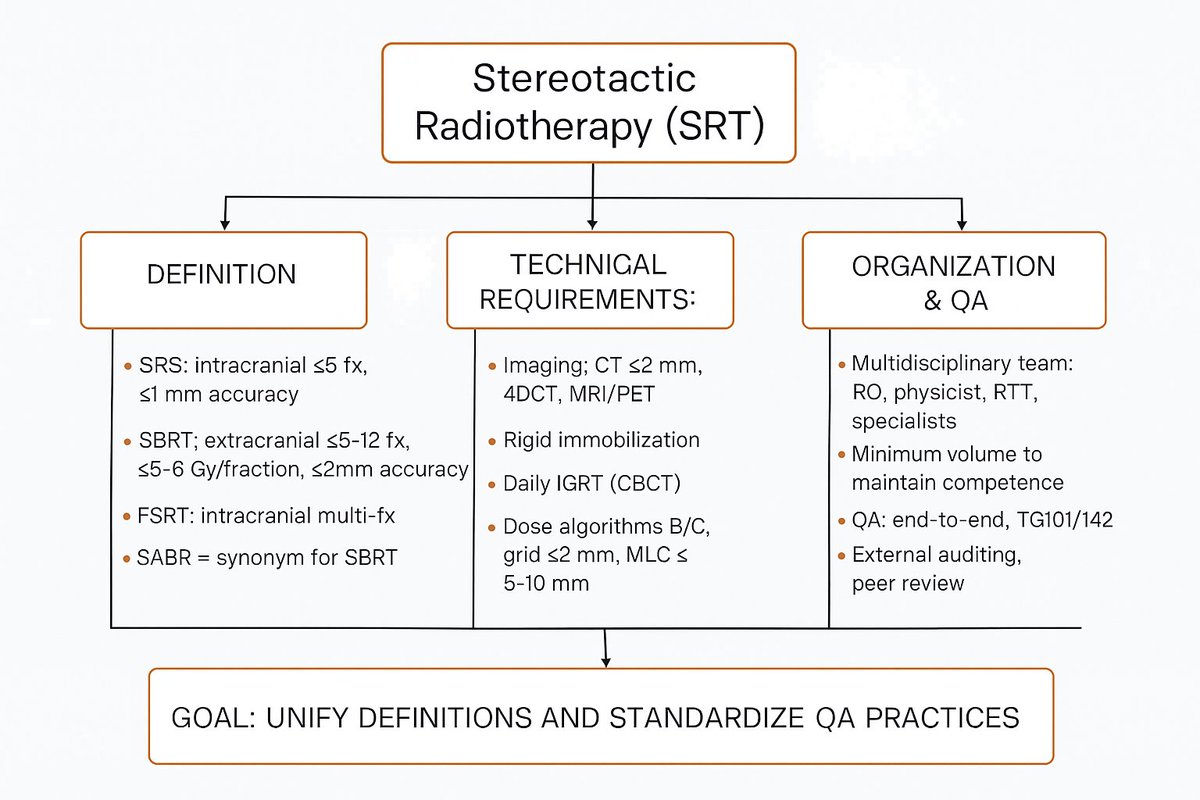
A few years ago, @rweichselbaum posed—ironically, but not entirely so—the question: what is the difference between radiotherapy and radiosurgery?
In some ways, this review attempts to answer that very question.
This table provides a synopsis of its contents. #radonc
thegreenjournal.com/article/… #radonc
4
10
21
7,774
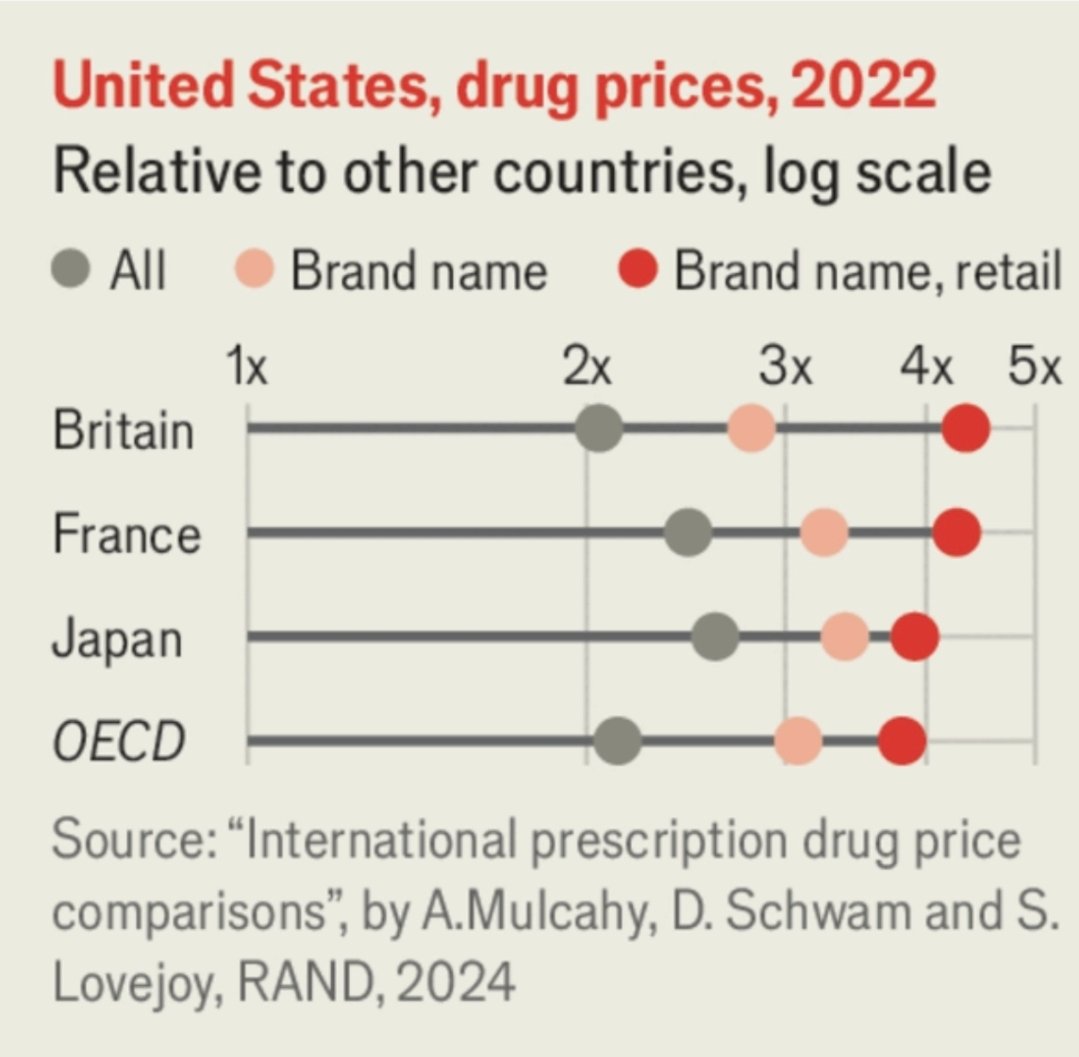
5 Oct 2025
Grafico tratto da un articolo del The Economist. Gli Americani, per avere un accesso più rapido alle terapie con nuovi farmaci, le pagano da 2 a 5 volte in più rispetto alla media dei paesi OCSE. Questo è il risultato di un Sistema Sanitario affaristico, in cui non vige il principio di universalità. Speriamo in Italia questo non avvenga. I tempi grami in cui versa il #SSN non mi inducono all' ottimismo. @Cartabellotta
2
215