
Radiation Oncology, IOSI - Oncology Institute of Southern Switzerland, EOC, Switzerland
Joined September 2018
- Tweets 2,822
- Following 990
- Followers 1,975
- Likes 6,123
66 Photos and videos








Thomas Zilli retweeted

Delighted that our STAMPEDE paper on abiraterone therapy selection with MMAI in high risk M0 HSPC now out. kwnsfk27.r.eu-west-1.awstrac…
4
25
83
11,191
Thomas Zilli retweeted

Jun 3
The #PROTEUS trial contributes important knowledge to the evolving evidence on high-risk #prostatecancer treatment options. ASTRO’s new summary document from @NehaVapiwala and @AmarUKishan is a member resource for discussions with your #multidisciplinary colleagues and patients.
ow.ly/2nBj50Z7kZj
5
15
31
21,916
Thomas Zilli retweeted

🚨CAN-2409 RT: not just delaying PSA failure, reducing residual tumor in the gland.🚨
@TheLancetOncol
👉Phase 3, double-blind RCT
🧑🤝🧑745 pts w/ int/high-risk localized #prostatecancer
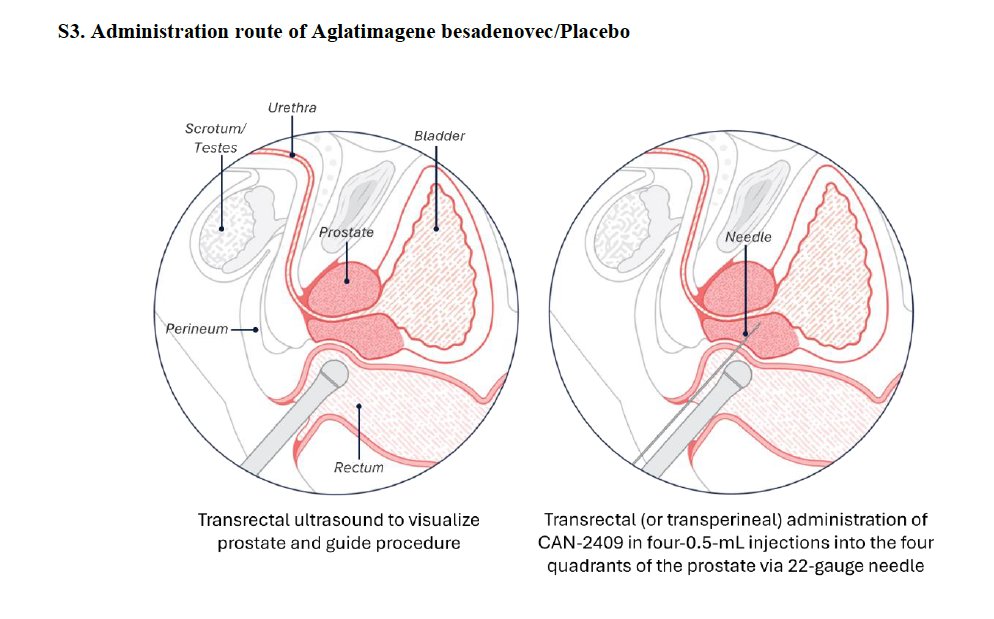
⚖️EBRT intraprostatic CAN-2409/valacyclovir vs placebo.
💉CAN-2409 is a replication-defective adenoviral HSV-tk gene therapy injected into the prostate.
💊Valacyclovir acts as the prodrug to drive local tumor-cell kill immune priming
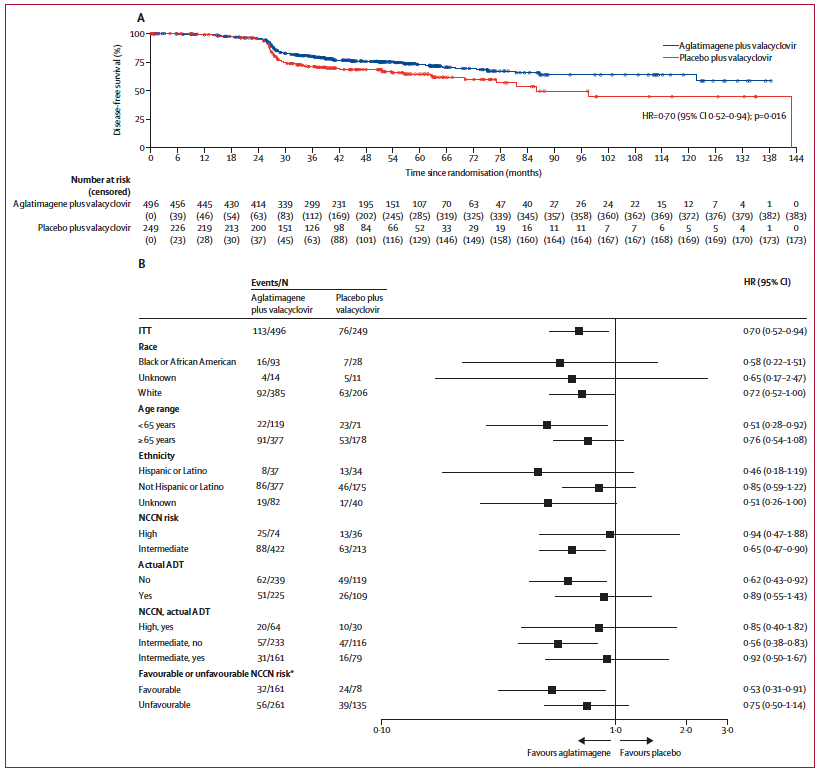
📉 DFS improved: HR 0.70; median NR vs 86.1 mo.
🔬 Key nuance: DFS included local failure by centrally reviewed positive prostate biopsy, protocol biopsy ~2 yrs post-EBRT.
🎯 At 22–26 mo: positive biopsies 20% vs 36%; pCR 80% vs 63%.
🛡️ No major toxicity penalty: grade ≥3 TEAEs 8% vs 7%; no treatment-related deaths.
🔑CAN-2409 may not just suppress biochemical recurrence, it may deepen local tumor eradication after RT.
@PCFnews @PCF_Science @urotoday @UrologyTimes
🔗shorturl.at/o3ZUq
4
22
46
11,150

ESTRO welcomes the #PROTEUS findings at #ASCO2026, which may expand options for high-risk #prostatecancer. Alongside definitive #radiotherapy ADT, these results reinforce the value of #multidisciplinary tumour boards in guiding patient-centred care.
👉bit.ly/49xYKxL

8
17
1,025
Thomas Zilli retweeted

Jun 3
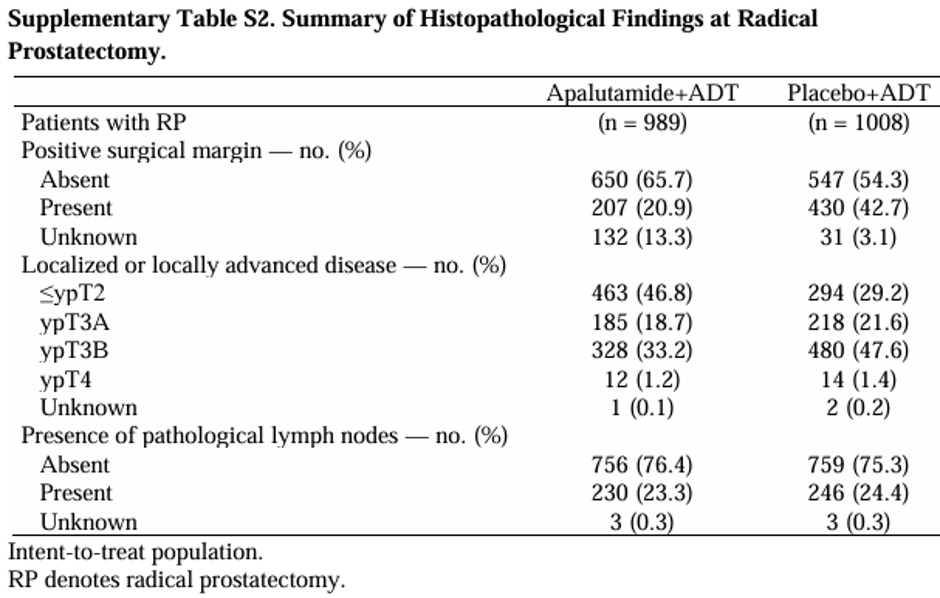
Can you help with an issue I can't grasp? If the primary endpoint of local pathological complete response or minimal residual disease is potentially clinically significant why was there no difference in histopathological lymph nodes? Is this typical of neoadjuvant trials?

5
6
16
5,522
Thomas Zilli retweeted

🚀 Virtual Grand Round in Radiation Oncology
Latest results of the EXTEND trial
🎤 Dr. Chad Tang
Addition of MTD to SoC for Oligometastatic Solid Tumors: Primary Analysis of EXTEND
📅 2. June 2026, 17:00–17:30 CEST
💻 Join us virtually here: lnkd.in/eiPx5WhQ
2
8
47
2,409
Thomas Zilli retweeted

Jun 3
This is so cool!!! Thanks @TheLancetOncol #radonc
Jun 2

Kidney SABR on the front cover of @TheLancetOncol. A well-deserved recognition for @_ShankarSiva for his work and efforts over the past 10 years.
thelancet.com/journals/lanon…
7
38
205
11,464
Thomas Zilli retweeted
Maybe cite our data - we have the largest series! pubmed.ncbi.nlm.nih.gov/3557…. It’s a made up
criterion to help get urologists to buy into referral by making them do extra stuff. No proven benefit and possible harm eg perforation.

In clinical practice I still see a lot of push back if you downplay the role of TURB as part of treatment. Some clinicians view it as an integral part of bladder sparing. No (maximal) TURB, no chemorads.
2
9
26
6,573
Thomas Zilli retweeted

This!
May 31

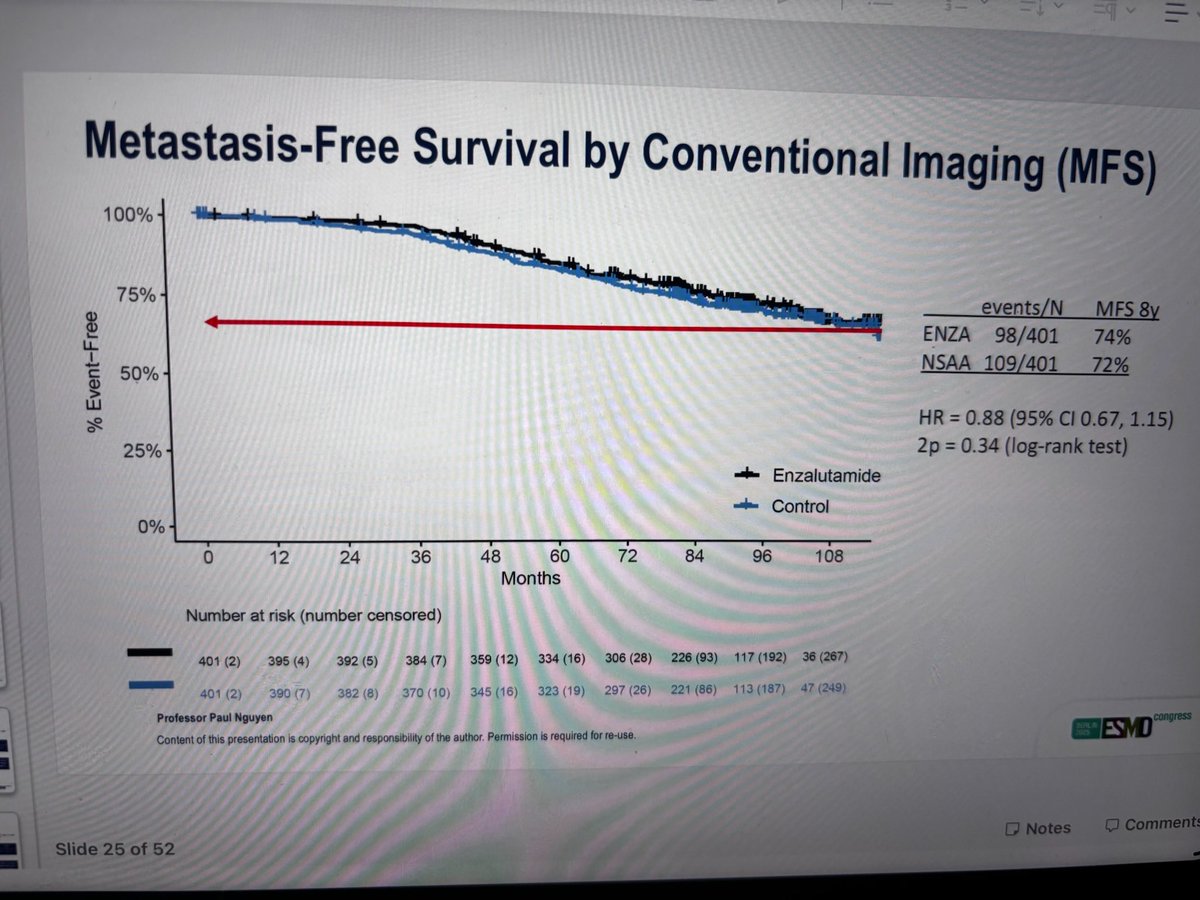
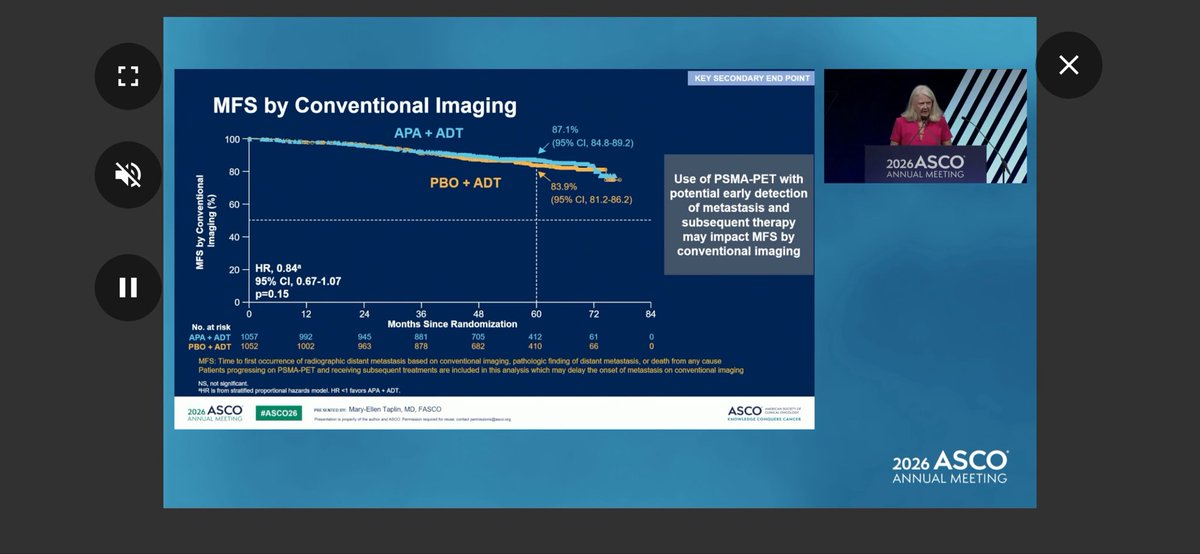
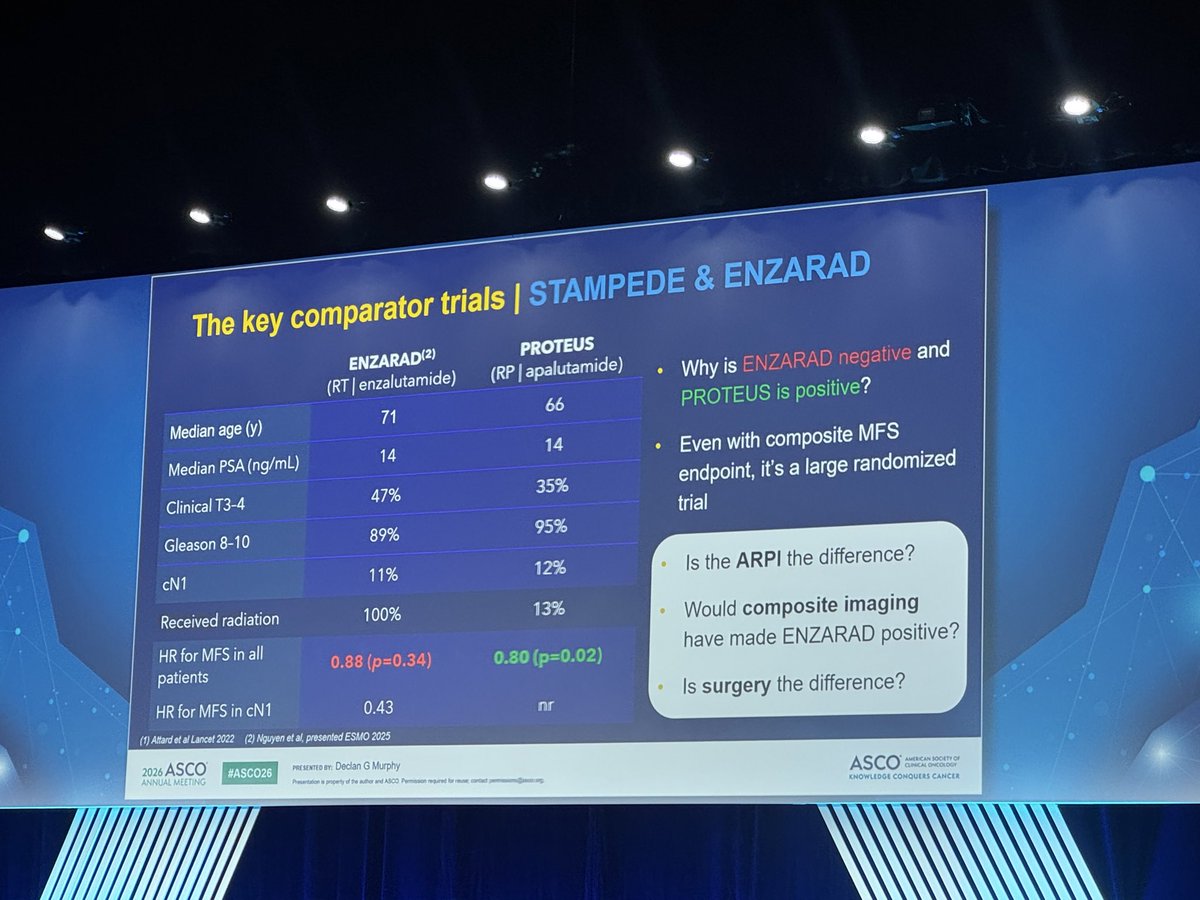
MFS by conventional imaging identical between ENZARAD and PROTEUS at 5 y and both trials negative for addition of ARPI. This was the initial primary in PROTEUS and hard to see why should be viewed as positive. PET imaging triggered by PSA >0.2 hence PROTEUS MFS = PSA PFS
2
20
2,553
Thomas Zilli retweeted

May 31
COMPPARE landed where its design pointed: proton and photon look equivalent for early toxicity and 3-year freedom from PSA progression, and both are reasonable standard of care. But the population may have been predicted to find no difference.
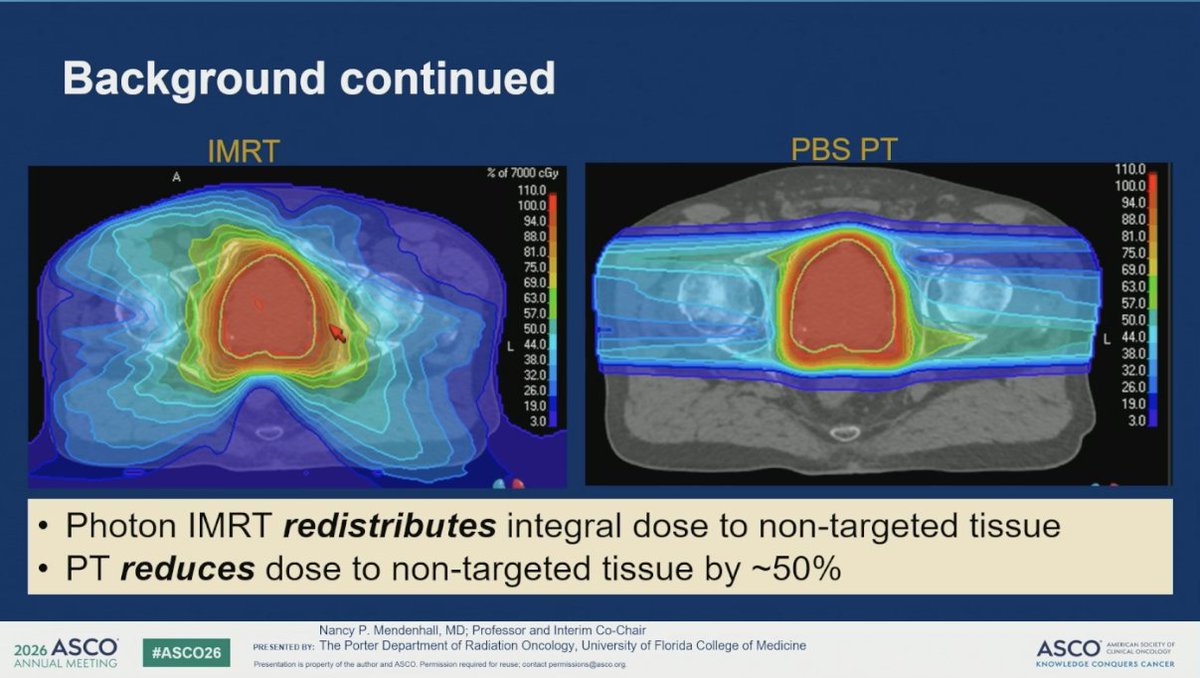
🔍 The case for protons is lower integral dose to non-target tissue. That matters most when you treat large volumes, like whole-pelvis nodal RT in high-risk or node-positive disease
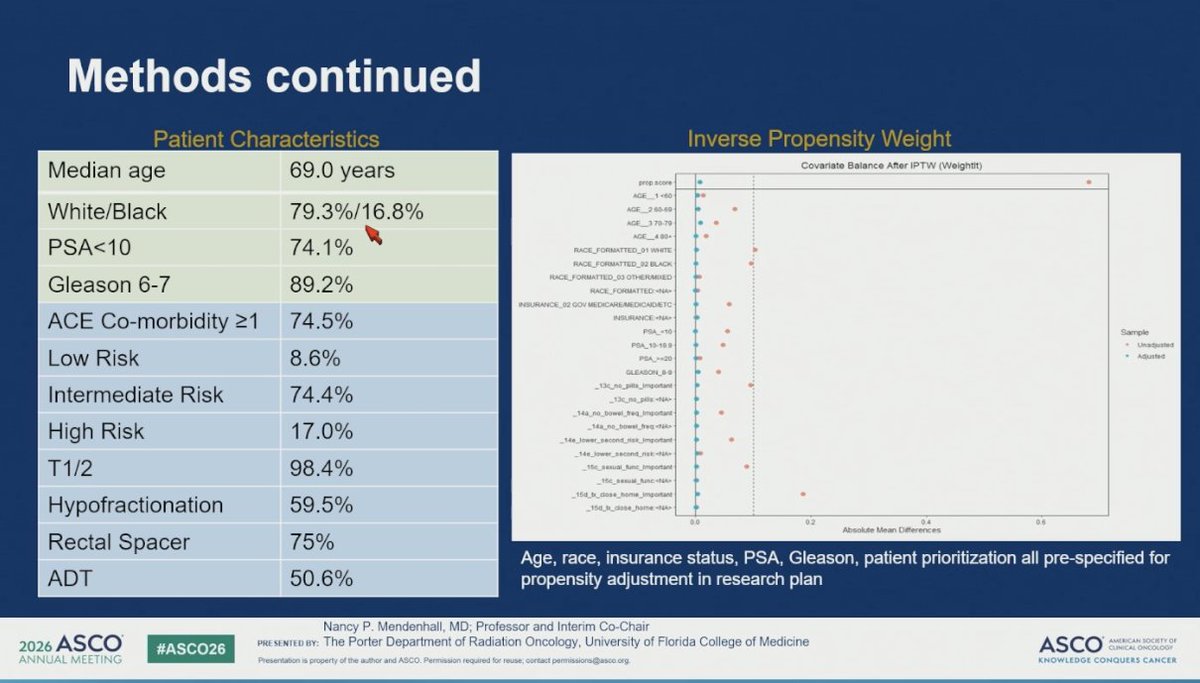
🔍 COMPPARE was 74% intermediate risk, 98% T1/2, mostly prostate-only fields, and excluded very high risk and metastatic. Small target, little room for protons to separate
🔍 75% got rectal spacers, which lowers rectal dose in both arms and narrows any modality gap
🔍 Bowel urgency was about 6% in both arms. At that event rate, equivalence is hard to interpret
The cleaner test is the patient you actually irradiate widely: high-risk, cN1, PSMA-PET node-positive, getting whole-pelvis treatment. That is where reduced integral dose could show up as less GI toxicity and, over time, fewer second malignancies.
The cleaner test is the patient you actually irradiate widely: high-risk, cN1, PSMA-PET node-positive, getting whole-pelvis treatment. That is where reduced integral dose could show up as less GI toxicity and, over time, fewer second malignancies. Hope we can see this study to come!
The patients most likely to benefit from protons were the ones this trial left out.
#ProstateCA #GUonc #ASCO26 @OncoAlert #RadOnc #ProtonTherapy

3
10
17
2,080
Thomas Zilli retweeted

IMHO, the sole advantage of surgery for these high risk pts would be the possibility of avoiding long-term ADT. With perioperative ADT, not only is this advantage lost, but we also forfeit critical data, such as accurate surgical staging and postoperative PSA🤷🏻♂️
May 31

4/n #ASCO26
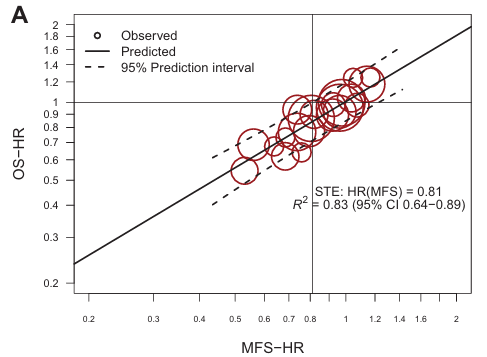
The ICECaP group (@ChrisSweens1) showed using semi-newer trials than the original publication, a slightly weaker treatment effect correlation of MFS and OS, with a surrogate threshold effect (STE) of 0.81 (more on this shortly!). Notably almost none of these trials are surgery trials. The only surgery trial of RP /- systemic therapy included was CALGB90203.
Surrogacy is treatment and disease state specific.
Ignoring this, MFS was based on conventional imaging.
@AmarUKishan @I_Migowski @TylerSbrt
3
5
34
4,784
Thomas Zilli retweeted

May 31
#ASCO26 🧬
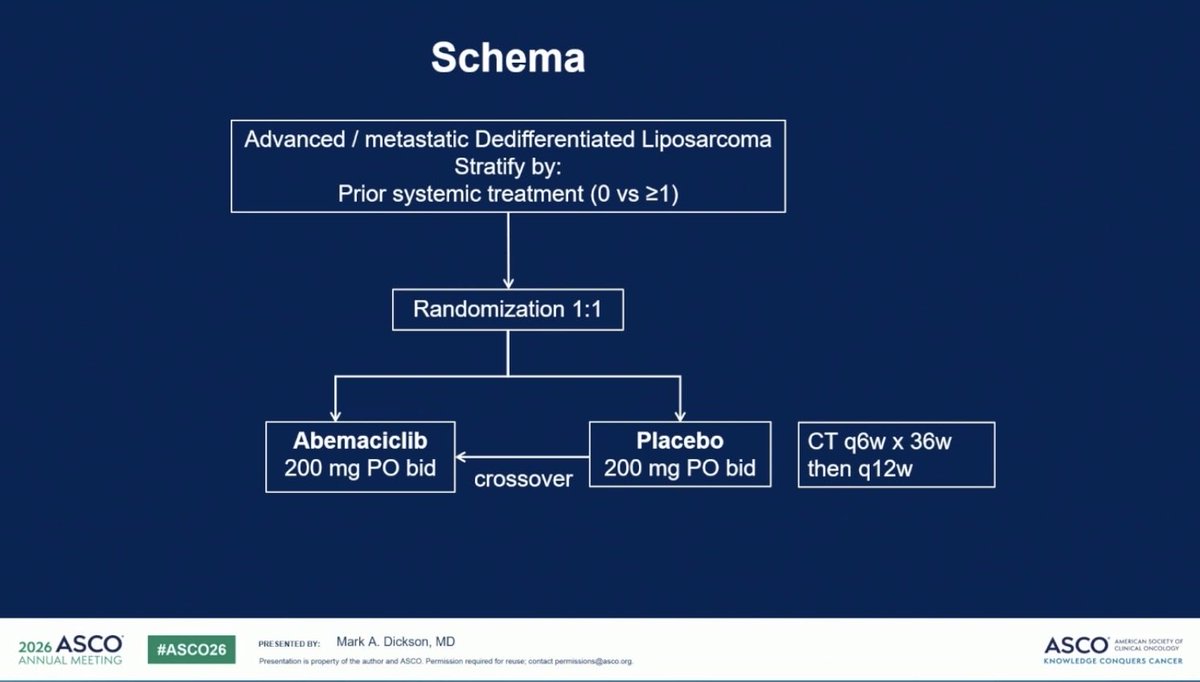
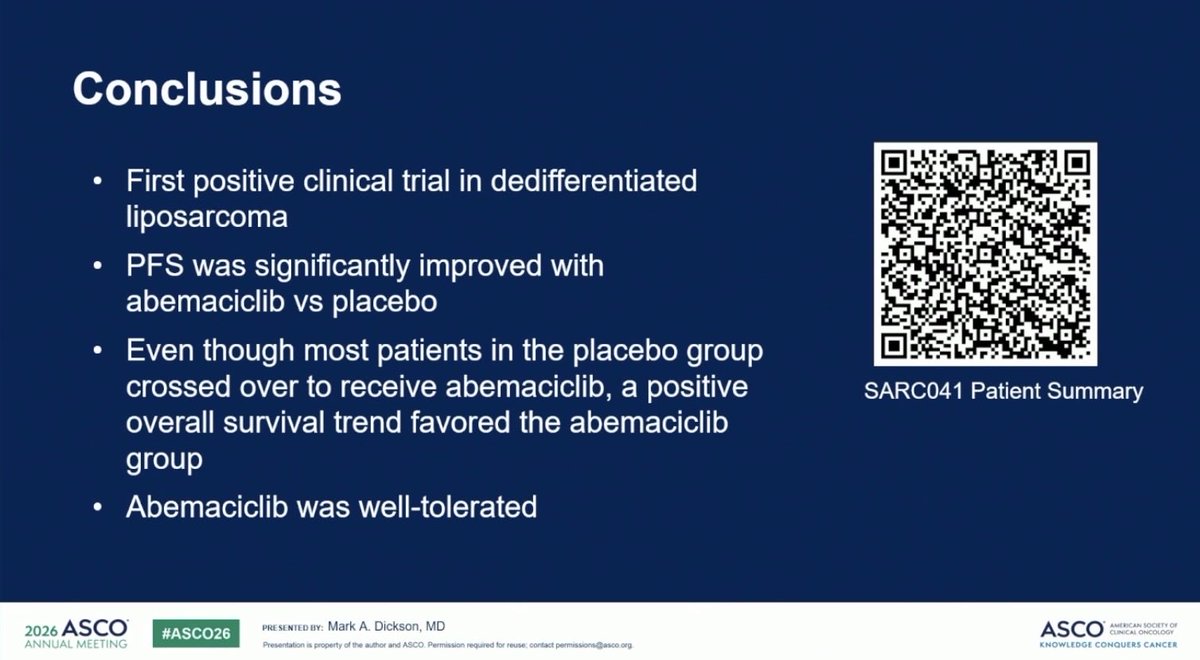
A rare positive phase III sarcoma trial.
SARC041 showed abemaciclib significantly improved PFS in advanced dedifferentiated liposarcoma.
👥 108 patients
Abemaciclib vs placebo
85% crossover allowed
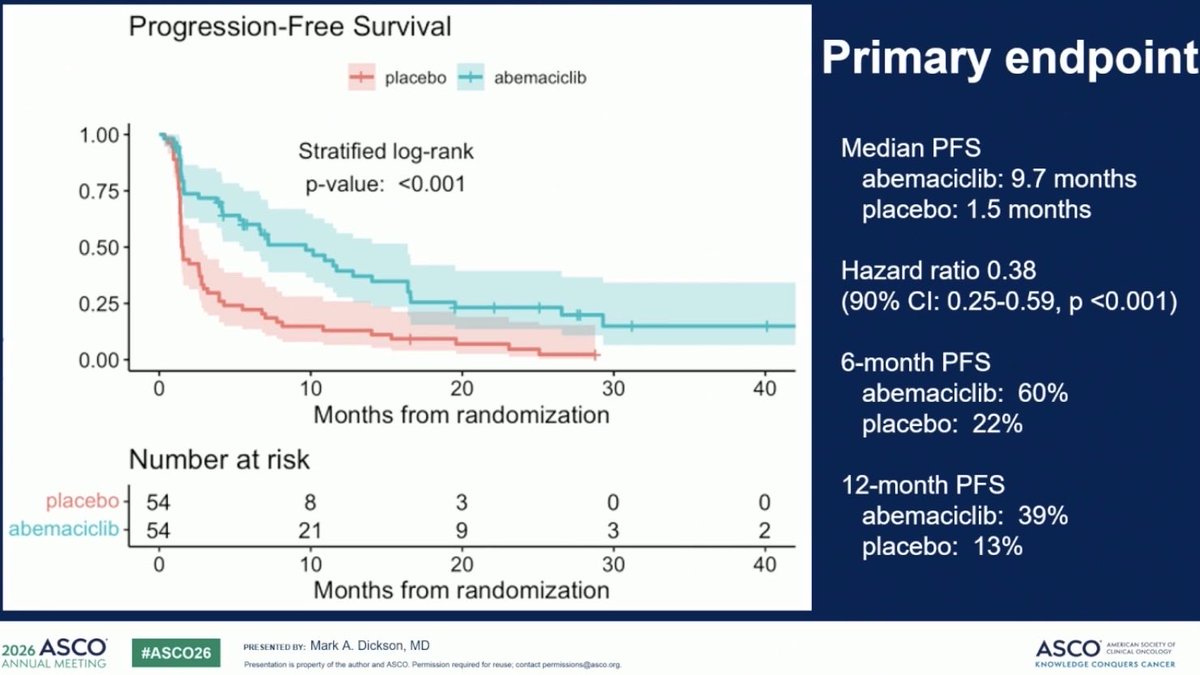
📊 Results:
• mPFS: 9.7 vs 1.5 mo
• HR 0.38, p<0.001
• ORR: 9% vs 0%
• OS trend favored abemaciclib
(HR 0.55)
🧪 Biggest benefit seen in treatment-naïve patients:
mPFS 16.4 months.
⚠️ Main AEs:
Diarrhea, neutropenia, anemia
Dose reductions: 39%
DDLPS has had very few targeted successes.
CDK4/6 inhibition may finally have a real role here.
🔖 One of the most important sarcoma reads from #ASCO26.
@OncoAlert @ASCO @myesmo @esmo_open @larvol
#OncoTwitter #Sarcoma #Liposarcoma #CDK46 #Abemaciclib #ASCO26


12
36
4,417
Thomas Zilli retweeted

May 31

Another provocative Q from @declangmurphy: does RP explain the diff across these parallel trials? #PROTEUS #ASCO26
3
9
38
7,576
Thomas Zilli retweeted

May 31
#ASCO26
The PROTEUS trial results are now online...buckle up as we wait to see the full presentation. This is going to be a trial that is likely highly controversial until the full results are published.
Some may call this a homerun, others may call this the largest negative trial @ASCO 2026. Up to you to interpret!
@urotoday @EricTopol @DrChoueiri @neerajaiims @ASCO @US_FDA @NCCN @myESMO @ASTRO_org @PCF_Science @declangmurphy @mcuban
7
61
153
71,446
Thomas Zilli retweeted
May 31
6/n #ASCO26
This is the crux of the problem, MFS by PET closely mirrors EFS, and will certainly have a STE below 0.5.
Conventional imaging:
~50% of BCR events with conventional imaging result in positive scans.
- RTOG 9202 with 15 yr fu: RT LT-ADT: 45% had BCR at 15yr, but only 17% had DM.
PET imaging:
>95% of BCR events with PET result in positive scans.
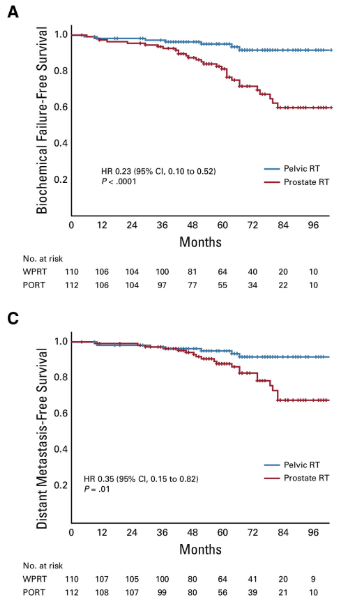
-POP-RT w/ 5yr fu: WPRT LT-ADT: Every BCR correlated to a PET finding with 6 of the 7 BCR events having corresponding DM events. You can see the KM curves are nearly identical for BCR-free survival and MFS.
@VedangMurthy @DrHowardSandler @DrMHofman @jmmrad
2
7
19
4,398
Thomas Zilli retweeted

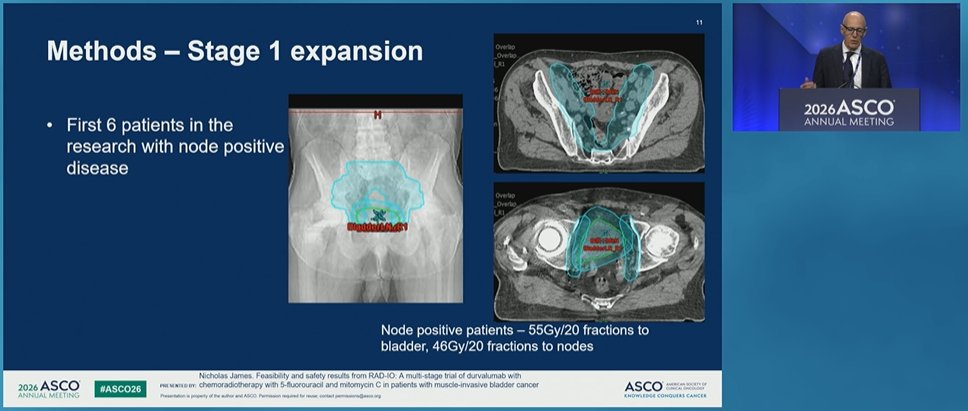
#ASCO26 🔬 Abstract 4504 | RAD-IO
Durvalumab chemoradiotherapy in muscle-invasive bladder cancer
Presented by Nicholas D. James, PhD, MBBS, FRCP
@OncoAlert
@ASCO
Bladder preservation in MIBC remains one of the most important curative-intent questions in GU oncology.
The key question here:
➡️ Can immune checkpoint inhibition be safely integrated with standard chemoradiotherapy?
RAD-IO evaluated durvalumab with bladder-directed chemoradiotherapy using 5-FU mitomycin C in patients with muscle-invasive bladder cancer.
🧪 Study design
Stage 2 efficacy cohort:
• T2 N0–2 M0 MIBC
• CRT durvalumab
• Single-arm phase II design
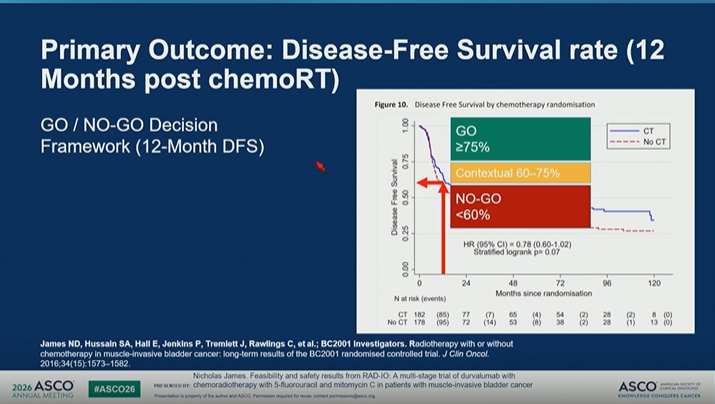
• Primary endpoint: 12-month disease-free survival
• 12-month DFS used as a surrogate for longer-term outcome
The trial used a clear GO / NO-GO framework:
🟢 GO: DFS ≥75%
🟡 Contextual: 60–75%
🔴 NO-GO: <60%
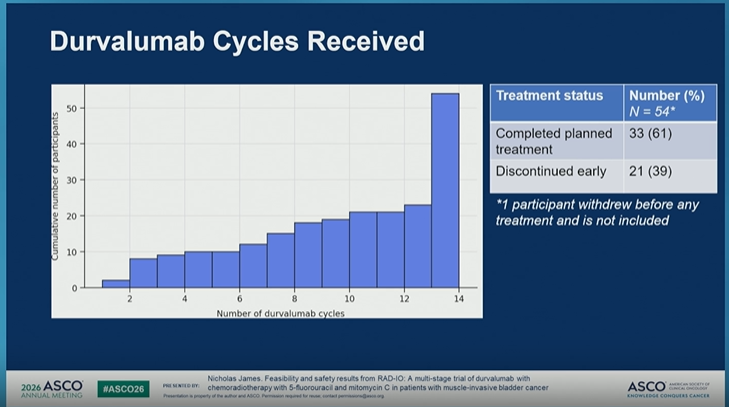
📌 Feasibility
Among 54 participants who started treatment:
• 100% received full radiotherapy: 55 Gy in 20 fractions
• 0 stopped radiotherapy early
• 87% had no RT extension or delay
• 100% received mitomycin C
• 100% received week 1 5-FU
• 78% received week 4 5-FU
• 61% completed planned durvalumab
• 39% discontinued durvalumab early
So, delivery of CRT was highly feasible, while immunotherapy completion was more challenging.
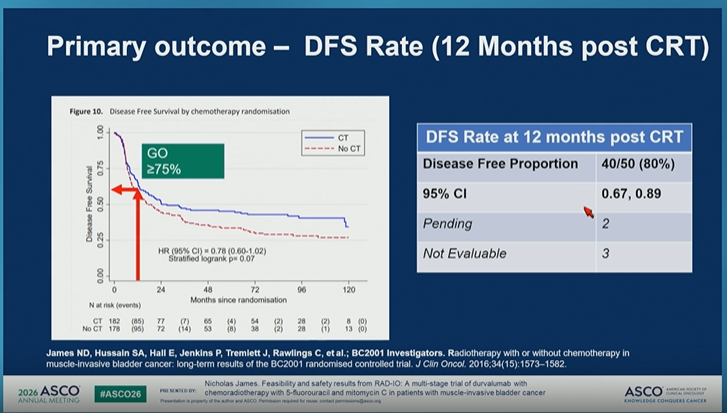
📊 Primary outcome
At 12 months post-CRT:
• DFS rate: 80%
• 40/50 disease-free
• 95% CI: 0.67–0.89
This crossed the prespecified GO threshold.
Secondary outcome PFS was consistent:
• No event: 83.6%
• Distant metastasis: 9.1%
• Local disease: 7.3%
💬 My take
RAD-IO provides an encouraging signal that durvalumab can be integrated with bladder-preserving chemoradiotherapy in MIBC.
But this is not yet practice-changing.
Important caveats:
🔹 single-arm phase II design
🔹 12-month endpoint
🔹 no randomized comparator
🔹 durability and late toxicity remain critical
🔹 completion of durvalumab was imperfect
Still, this is a very relevant direction.
In an era where systemic therapy is becoming increasingly active in urothelial cancer, bladder preservation strategies need to evolve too.
The next question is not simply whether CRT works.
It is:
➡️ Which patients are best suited for bladder preservation?
➡️ Can immunotherapy improve cure without compromising safety?
➡️ How should we integrate systemic therapy, radiation, surgery, and patient preference?
For MIBC, the future may be a more personalized curative-intent pathway — not one-size-fits-all cystectomy versus CRT.
#ASCO26 #GUOnc #BladderCancer #UrothelialCancer #MIBC #Immunotherapy #RadiationOncology #BladderPreservation
2
21
34
5,620
Thomas Zilli retweeted
#ASCO26 GU Oncology Spotlight 🚨
🔬 ENZAMET Decipher Prostate Classifier
Genomics to refine docetaxel intensification in mHSPC
As always, an outstanding and very clear presentation by @ChrisSweeney1.
Thank you, Dr. Sweeney.
@OncoAlert
@ASCO
In metastatic hormone-sensitive prostate cancer, treatment intensification has changed outcomes.
But one of the hardest clinical questions remains:
➡️ Who truly needs more intensification?
➡️ Who benefits from adding docetaxel to ADT enzalutamide?
➡️ Can biology help us avoid both undertreatment and overtreatment?
🟦 Why ENZAMET matters here
ENZAMET was an investigator-sponsored study evaluating:
• ADT standard non-steroidal antiandrogen
vs
• ADT enzalutamide
Importantly, the study later allowed planned early docetaxel after CHAARTED, creating a unique opportunity to explore:
🧬 ADT enzalutamide ± docetaxel
This is highly relevant to modern mHSPC decision-making.
🟩 Why Decipher is important
The Decipher Prostate Genomic Classifier uses a 22-gene mRNA signature.
It is designed to capture biologic features linked to:
🔹 metastatic potential
🔹 prognosis
🔹 disease aggressiveness
🔹 pathways such as DNA replication/repair, cell motility, and growth biology
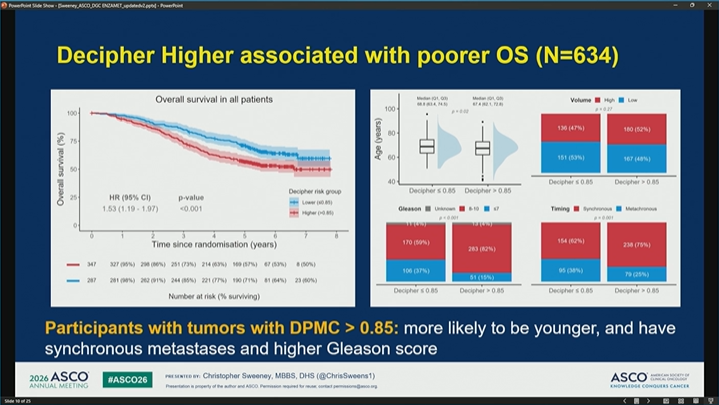
In this analysis, higher Decipher scores were associated with poorer overall survival.
🟨 The key hypothesis
Patients with tumors showing Decipher >0.85 may represent a biologically higher-risk group.
The study asked:
➡️ Could this group derive greater survival benefit from adding docetaxel to ADT enzalutamide?
And conversely:
➡️ Could patients with Decipher ≤0.85 avoid docetaxel without losing meaningful benefit?
🟧 Why this question matters clinically
Docetaxel can be effective.
But it also adds:
• toxicity
• clinic visits
• supportive care needs
• neuropathy risk
• infection risk
• quality-of-life impact
• access and feasibility issues
So the goal is not simply to add docetaxel to everyone.
The goal is to use clinical genomic risk to better personalize treatment.
🟥 Take-home from Part 1
This is exactly where prostate cancer care is heading:
Not only asking:
“Can we intensify?”
But asking:
“Who needs intensification most — and who can safely avoid it?”
Part 2: results clinical interpretation 👇
@DrChoueiri 🇺🇸@hoperugo 🇺🇸 @matteolambe 🇮🇹 @TiansterZhang 🇺🇸 @CathyEngMD 🇺🇸 @stolaney1 🇺🇸 @montypal 🇺🇸 @tompowles1 🇬🇧 @brian_rini 🇺🇸 @cdanicas 🇪🇸 @NiuSanford 🇺🇸 @amerseburger 🇩🇪 @GlopesMd 🇺🇸 @Icro_Meattini 🇮🇹 @PGrivasMDPhD 🇺🇸 @DrYukselUrun 🇹🇷
#ASCO26 #GUOnc #ProstateCancer #mHSPC #PrecisionOncology #Genomics #Decipher #Docetaxel #Enzalutamide

20
21
1,654
Thomas Zilli retweeted
#ASCO26 GU Oncology Spotlight 🚨
🔬 ENZAMET Decipher | Part 2
Can genomics guide docetaxel intensification in mHSPC?
Outstanding presentation by @ChrisSweeney1.
@OncoAlert
@ASCO
After Part 1, the key question was:
➡️ Can a genomic classifier identify which patients with mHSPC benefit most from adding docetaxel to ADT enzalutamide?
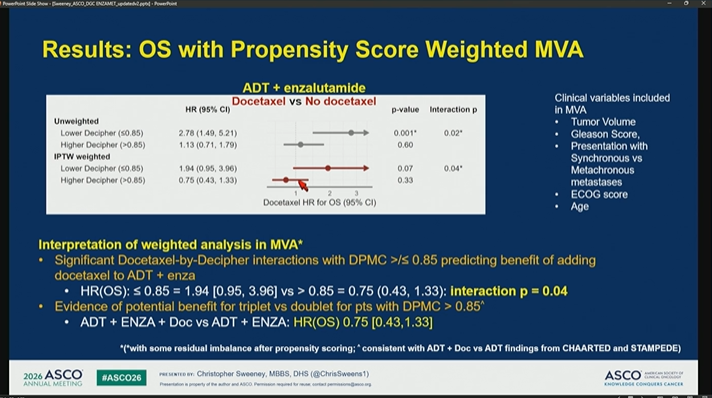
🟦 Key result
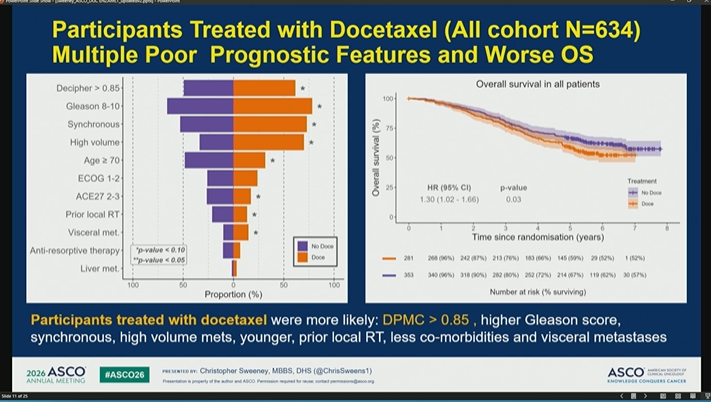
Patients with Decipher / genomic classifier >0.85 had worse outcomes with ADT enzalutamide alone.
This suggests that high genomic risk captures a biologically aggressive subgroup not fully explained by clinical variables alone.
🟩 Docetaxel signal
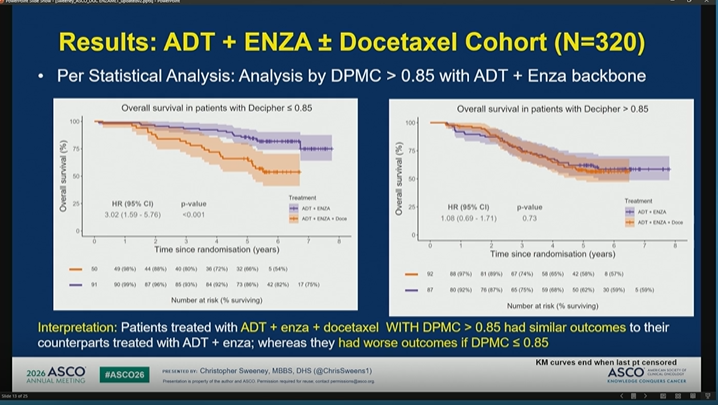
In propensity score–weighted analyses:
🔹 Decipher ≤0.85
Less evidence of benefit from adding docetaxel to ADT enzalutamide
🔹 Decipher >0.85
Evidence of benefit from adding docetaxel to ADT enzalutamide
Reported interaction signal supported a docetaxel-by-Decipher effect, suggesting Decipher may help identify who is more likely to benefit.
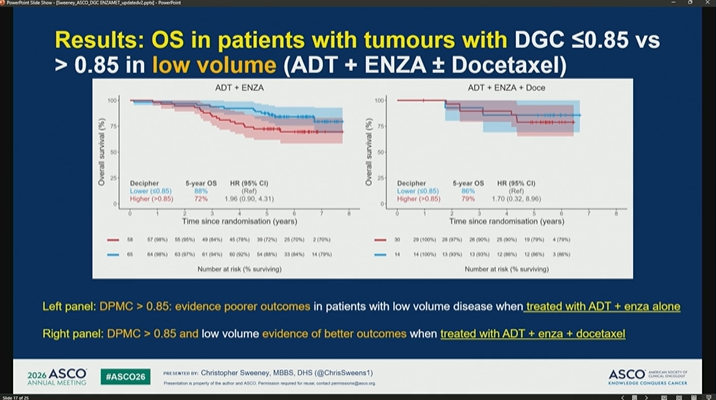
🟨 Low-volume disease matters
This is especially relevant because treatment intensification in low-volume mHSPC is often nuanced.
In the low-volume subgroup:
• Decipher >0.85 identified patients with poorer outcomes on ADT enzalutamide alone
• outcomes appeared better when docetaxel was added
This could help refine a space where clinical decision-making is often individualized.
🟧 Secondary endpoints
The signal appeared consistent across several endpoints, including:
✓ progression-free survival
✓ PSA progression-free survival
✓ prostate cancer–specific survival
This strengthens the biological plausibility of the finding.
🟥 Important limitations
This is not a simple “test says yes/no” rule.
Caveats include:
• no randomization to docetaxel
• subgroup sample sizes are limited
• propensity weighting helps but cannot remove all bias
• global access to genomic testing remains an issue
• treatment decisions still require clinical context
💬 Clinical interpretation
Decipher >0.85 may identify patients with mHSPC who have:
➡️ poorer prognosis with ADT enzalutamide alone
➡️ greater likelihood of benefit from adding docetaxel
Decipher ≤0.85 may identify patients with less evidence of docetaxel benefit — where avoiding chemotherapy could be reasonable in selected cases.
My take:
This is exactly the direction prostate cancer care needs to move:
Not just intensification for all.
But biology-informed intensification.
The future of mHSPC algorithms will likely combine:
✓ disease volume
✓ timing of metastases
✓ clinical risk
✓ genomic risk
✓ patient fitness
✓ toxicity tolerance
✓ access and preferences
The goal is to avoid both undertreatment and overtreatment.
#ASCO26 #GUOnc #ProstateCancer #mHSPC #PrecisionOncology #Genomics #Decipher #Docetaxel #Enzalutamide

22
33
3,542
Thomas Zilli retweeted

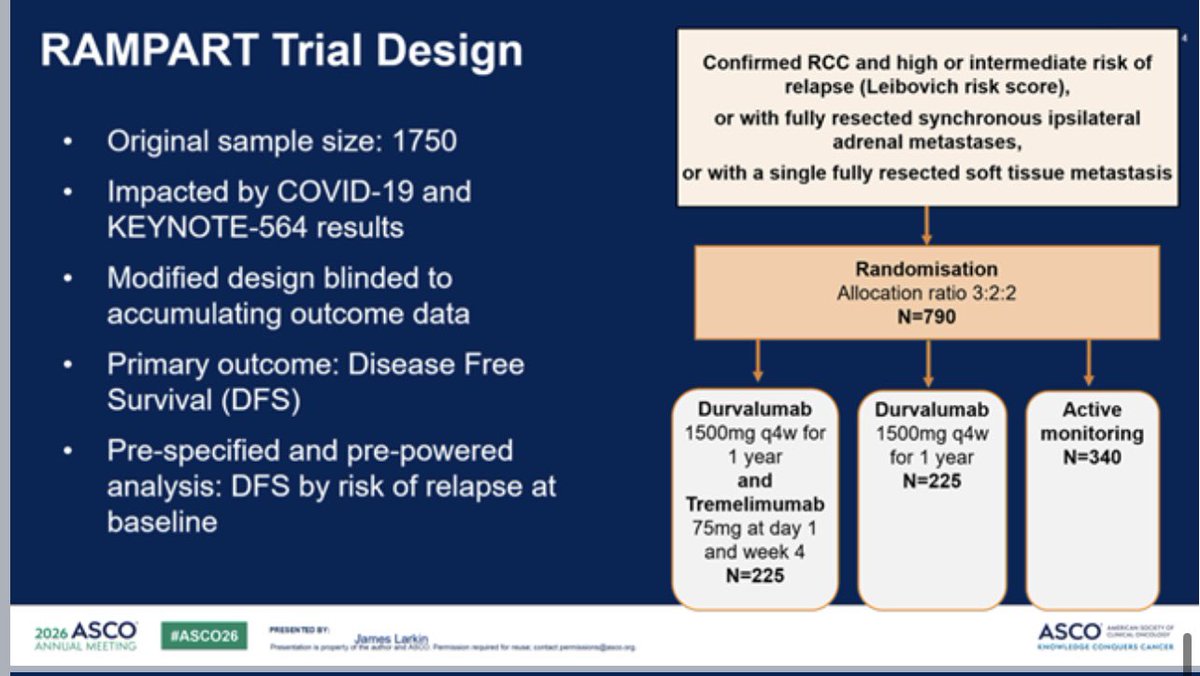
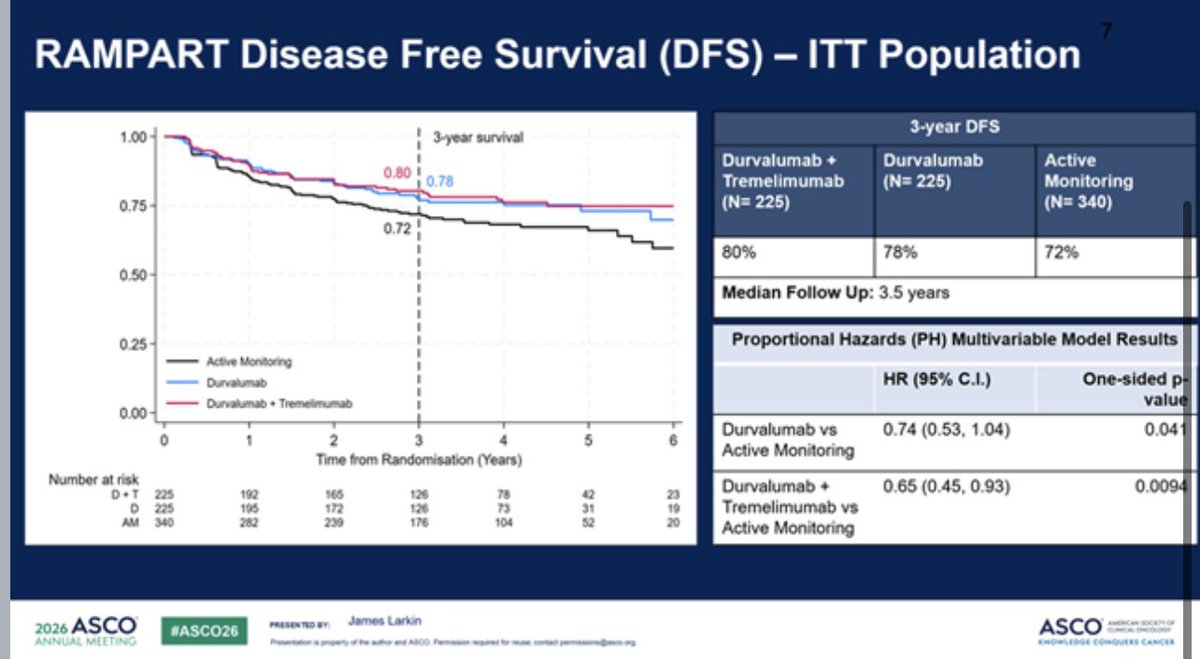
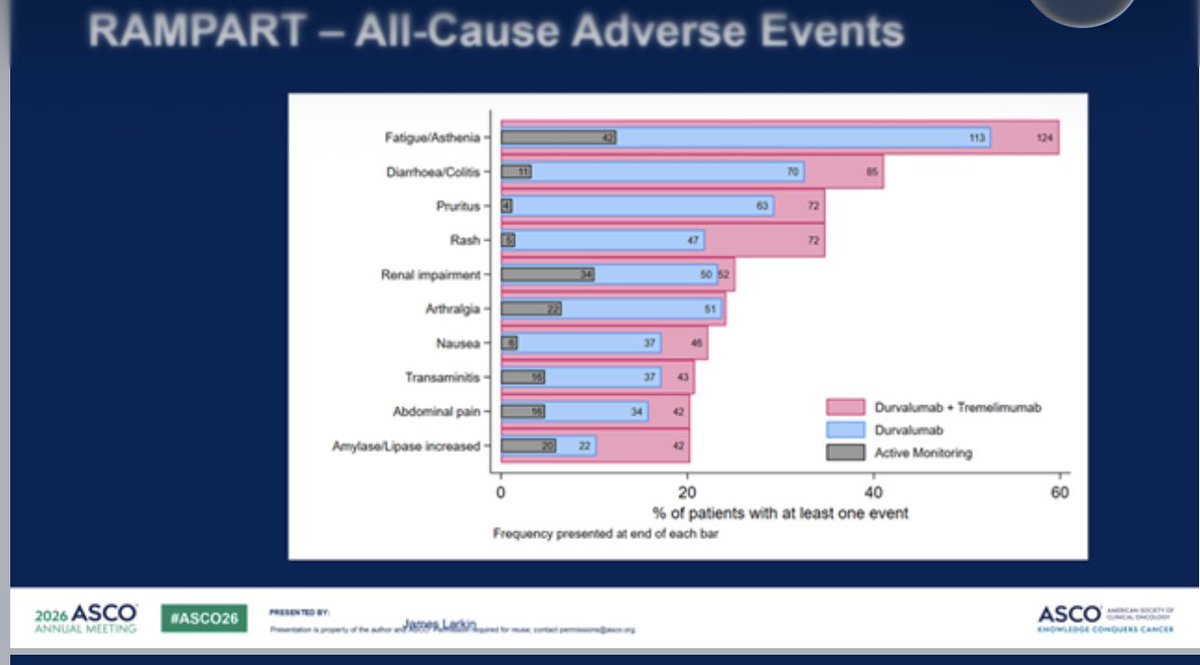
May 30
RAMPART is the 1st trial to compare PD-L1 vs PD-L1/CTLA4 vs surveillance in adjuvant renal cancer. Only the combination (durva/tremi) is statistically positive for DFS but the numbers are similar for durvalumab alone (especially in clear cell subset). Benefit may have been enriched in the high risk group. The combination has predictable toxicity. This support the premise of the benefit of ICI therapy in UC. It has not clearly resolved the issue of the additional benefits of CTLA4 #ASCO26 @OncoAlert

1
36
70
4,649


