
Founder - MaxWell Clinic. The Curious Physician. International Speaker. Best selling author.
Joined December 2014
- Tweets 427
- Following 381
- Followers 588
- Likes 326
129 Photos and videos








im skipping the line for Polymarket. if you care about being early, use my link: polymarket.com/app/jkefo
13
David H. Haase, MD retweeted

Apr 10
44
392
1,466
1,382,695
David H. Haase, MD retweeted

A Prayer In Spring
by Robert Frost
Oh, give us pleasure in the flowers today;
And give us not to think so far away
As the uncertain harvest; keep us here
All simply in the springing of the year.
Oh, give us pleasure in the orchard white,
Like nothing else by day, like ghosts by night;
And make us happy in the happy bees,
The swarm dilating round the perfect trees.
And make us happy in the darting bird
That suddenly above the bees is heard,
The meteor that thrusts in with needle bill,
And off a blossom in mid air stands still.
For this is love and nothing else is love,
To which it is reserved for God above
To sanctify to what far ends he will,
But which it only needs that we fulfill.

5
28
148
9,763
David H. Haase, MD retweeted

Feb 27
youtube.com/watch?v=laN9LS7g…
The Groundbreaking Alzheimer's Therapy Improving Cognition | Dr. David Haase
Today, I am very honored to introduce Dr. David Haase. David Haase, MD, holds dual board certifications in Family Medicine and Integrative Holistic Medicine, along with certification in Apheresis (QIA). A graduate of Vanderbilt University School of Medicine, he completed his residency at the Mayo Clinic. Dr. Haase educates physicians globally on managing Alzheimer's, dementia, and chronic illnesses.
In 2003, Dr. Haase founded the MaxWell Clinic in Brentwood, TN, a 12,000-square-foot facility dedicated to advanced diagnostics, nutrition, and brain optimization. He is the innovator behind the H.O.P.E.: Habitat Optimizing Plasma Exchange program, a groundbreaking treatment designed to enhance cognitive function and slow cognitive decline in conditions such as Alzheimer's and dementia. This program uses advanced plasma exchange techniques to improve brain health and overall well-being.
Dr. Haase is also committed to building ever-better clinical data platforms that empower relationship-based clinicians to integrate systems medicine more seamlessly into patient care. In addition to his clinical work, he actively consults for and serves on the boards of several biotech and medical science companies, contributing to cutting-edge research in Alzheimer's disease, longevity, and cognitive performance. Dr. Haase was also one of the six lead investigators on the Evanthea Dementia Reversal Randomized Controlled Trial that just concluded. His commitment to advancing medical science and improving patient outcomes has established him as a leader in functional and integrative medicine and I am very honored to have him with us today.
Hope this is helpful for you and your family!
@DavidHaaseMD @MaxWellClinic
#alzheimers #alzheimersprevention #alzheimersreversal #evantheadementiareversal #plasmaexchange #therapeuticplasmaexchange #maxwellclinic
2
5
392
David H. Haase, MD retweeted
Most people don't understand how incredibly complex 340B is. I barely get it myself.
340B creates a pricing spread. Hospitals buy drugs at a steep federally mandated discount and get reimbursed at a much higher rate. That difference is a huge revenue stream for hospitals.
Manufacturers have tried to limit some contract pharmacy arrangements, which squeezed certain middlemen.
So what happens next?
Instead of losing access to that spread, insurers and PBMs move deeper into the hospital itself.
Insurer owns the PBM. PBM buys a specialty pharmacy platform. That specialty pharmacy operates inside a 340B hospital. Now the same corporate family can still capture the margin. Different structure. Same spread.
This is what a federally created arbitrage program does. It does not lower costs. It does not simplify care. It encourages vertical integration so the largest players can internalize the subsidy.
When government creates a guaranteed pricing distortion, capital reorganizes around harvesting it.
Feb 27

𝐂𝐢𝐠𝐧𝐚 𝐕𝐞𝐫𝐭𝐢𝐜𝐚𝐥 𝐈𝐧𝐭𝐞𝐠𝐫𝐚𝐭𝐢𝐨𝐧 𝐔𝐩𝐝𝐚𝐭𝐞 (𝐖𝐢𝐭𝐡 𝐚 340𝐁 𝐓𝐰𝐢𝐬𝐭)
Bob Herman @bobjherman at @statnews uncovered that Cigna Group’s Evernorth Health Services now owns 100% of CarepathRx, a company that helps hospitals and health systems build and operate in-house specialty pharmacies.
Recall that in 2025, Evernorth also invested $3.5 billion for an undisclosed stake in Shields Health Solutions, the former WBA subsidiary with a similar hospital-focused specialty pharmacy model.
Why it matters:
✅ Manufacturers’ limits on #340B contract pharmacies have pressured Express Scripts’ 340B profits.
✅Expanding deeper into hospital-owned specialty pharmacies is a clever vertical integration play that helps preserve access to 340B-driven profits through a different channel.
P.S. Yes, both deals will appear on DCI’s soon-to-be-updated (in)famous vertical integration slide. 😉
Story: drugch.nl/4rFqMhF
8
19
70
6,827
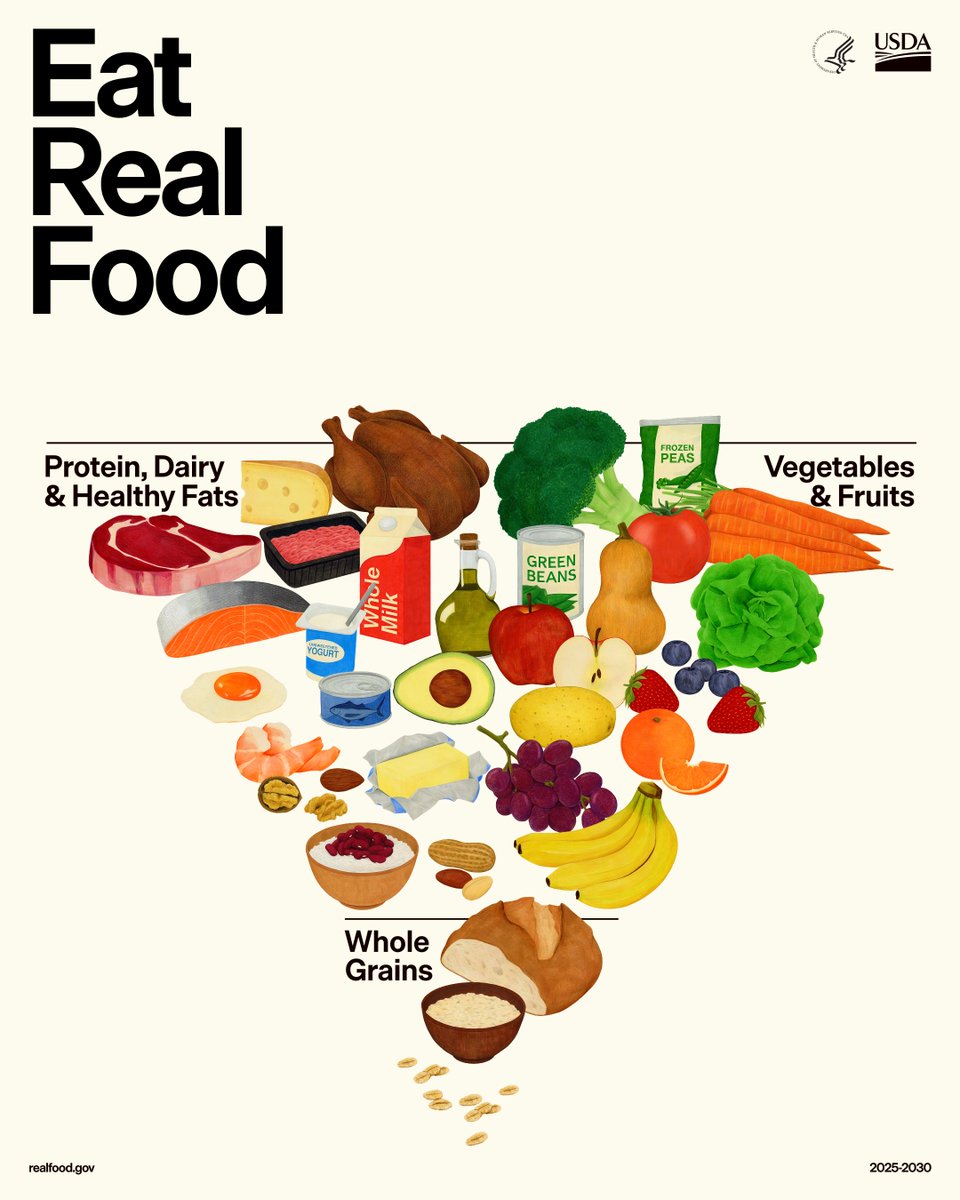
This is awesome! Very simple.
A good rule is you should only eat what you could grow, kill, or gather from nature yourself with only the processing you could do in the kitchen yourself.
It is profound what a huge effect this has on the human experience long-term.
Start a garden, even if it’s just a single pot, as soon as your growing season allows!
Doc

Under President Trump’s leadership, common sense, scientific integrity, and accountability have been restored to federal food and health policy.
For decades, the Dietary Guidelines favored corporate interests over common-sense, science-driven advice to improve the health of Americans.
That ends today.
The new Dietary Guidelines call for prioritizing high-quality protein, healthy fats, fruits, vegetables, and whole grains—and avoiding highly processed foods and refined carbohydrates.
1
7
142
Thanks, David! It is unconscionable that we still use this herbicide in the US.

The herbicide paraquat is so strongly linked to Parkinson’s that researchers use it to induce the disease in lab animals.
Yet its use continues to rise in the U.S. as Parkinson’s rates climb worldwide.
This deserves more attention.
You can learn more here: drperlmutter.com/paraquat-pa…
6
60
David H. Haase, MD retweeted

Jan 1
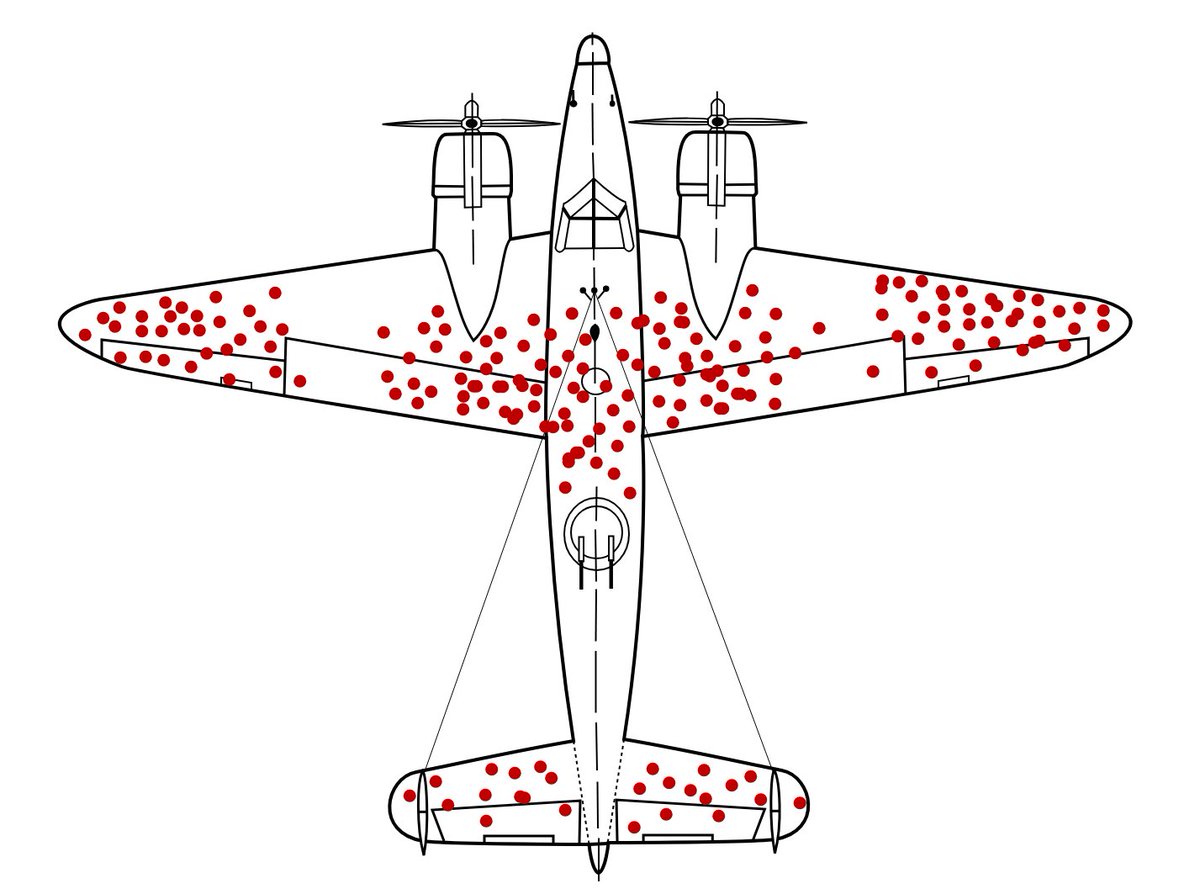
I'm obsessed with cognitive biases.
A "cognitive bias" is a systematic error in thinking that destroys decision-making.
11 most powerful (and dangerous) cognitive biases I've found: 🧵
1. Survivorship Bias:
41
548
2,272
933,718
David H. Haase, MD retweeted

12 Dec 2025
Chronic pain is a complex condition that affects many people worldwide and has been increasingly recognized as a biopsychosocial condition. What are the foundational components of the functional medicine model that support personalized treatment strategies for chronic pain?
In the following video, IFM educator @DavidHaaseMD discusses the functional medicine approach to chronic pain and explores those perspectives that may help empower patients in their healing journey. Read more: go.ifm.org/3KY1ueE
1
1
7
480

3 Dec 2025
The US healthcare system is approximately 19% of our GDP. It is a massive economic status quo where inefficiency creates cost without commensurate value .. this benefits the current stakeholders that are benefiting rather than the patients who need the care.
Read Dutch’s post and follow him. He makes a ton of sense.
3 Dec 2025

Five ideas that would lower U.S. healthcare costs immediately:
1.Repeal Certificate of Need laws.
They restrict supply, block competition, and protect incumbents.
2.Lift the ban on physician ownership in hospitals.
When physicians compete, costs fall and quality rises.
3.Expand ASC capacity everywhere.
Most states still restrict the lowest-cost, highest-value surgical setting.
4.Eliminate nonprofit tax loopholes.
If you behave like a corporation, you should be taxed like one.
5.Eliminate site-of-service payment differentials.
The same service at two different prices is not a market, it’s a subsidy.
1
5
163
13 Nov 2025
There’s so much that could be done right now with the swipe of a pen to decrease cost and increase access! Great job listing some of these John!!
13 Nov 2025

For all of the we’re trying crew….
Here’s What CMS and the Executive Branch Could Do Tomorrow Without Congress
a concrete list of actions CMS and HHS can take under existing authority. No bills. No committees. No “we tried.” These are decisions — and they’re all sitting on some bought off administrators desk.
1. Expand site-neutral payments.
Stop paying hospital-owned clinics more for the same service. It’s the single biggest driver of consolidation, and CMS can fix it with a pen.
2. Restrict anti-competitive physician non-competes.
CMS can condition Medicare/MA participation on fair employment terms instead of letting systems trap physicians and patients inside corporate fences.
3. Rein in prior authorization abuse.
Gold-carding, real timelines, specialty-matched reviewers, penalties for bad-faith denials — all possible now, without Congress.
4. Force Medicare Advantage transparency.
Publish denial rates, appeals, overturns, steering patterns, and utilization rules. MA has gotten away with too much because no one forces sunlight.
5. Fix Stark enforcement so it stops crushing small practices.
Clarify exceptions, stop weaponizing technical violations, and rewrite guidance that only massive systems can navigate.
6. Update practice-expense RVUs to reflect reality.
CMS controls RVU inputs. Adjusting them to match real private-practice overhead would stabilize half the physician economy.
7. Expand ASC and office-based procedure lists.
More spine, ortho, neuro, pain. Safer, cheaper, faster access. No legislative barrier.
8. Reform the audit and recoupment circus.
End extrapolated audits below defined thresholds. Require specialist reviewers. Fix recoupment timelines so small practices aren’t bankrupted by process.
9. Reduce the MIPS/MACRA administrative tax.
Simplify measures. Cut redundant documentation. Expand exemptions. CMS can do all of this with rulemaking.
10. Strengthen MA network adequacy.
Stop allowing MA plans to wall off independent physicians. Enforce real access standards and real specialist availability.
11. Expand telehealth flexibilities.
Fix originating-site rules, clean up supervision requirements, modernize modalities — low-hanging fruit.
12. Clean up enrollment and revalidation.
PECOS, site visits, and redundant documentation are pure administrative friction. CMS created these headaches; CMS can remove them.
13. Create physician-led models through CMMI (I hate CMMI, but if we’re going to spend money on it, this is the one good use of it.)
Independent specialist bundles, physician-led ACOs, and competition-friendly payment models are all within CMMI’s administrative authority.
14. Tackle corporate vertical integration that hides behind federal rules.
CMS can audit “steering,” offloading, and self-preferencing inside vertically integrated systems. They simply choose not to.
15. Enforce competitive fairness as a condition of Medicare participation.
CMS could take a harder stance on anti-competitive contracting, referral capture, and network manipulation — today.
2
746
David H. Haase, MD retweeted

8 Nov 2025
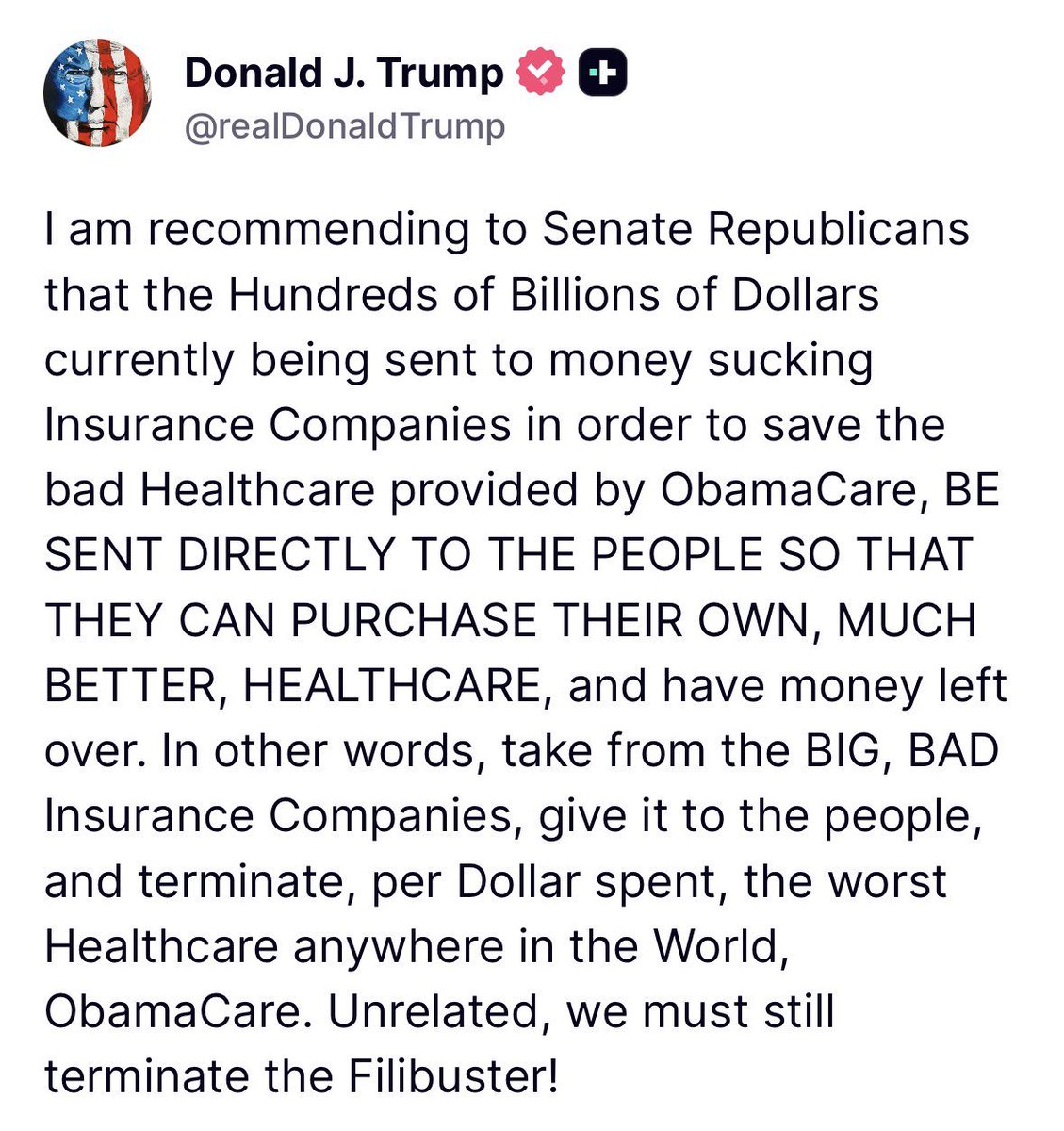
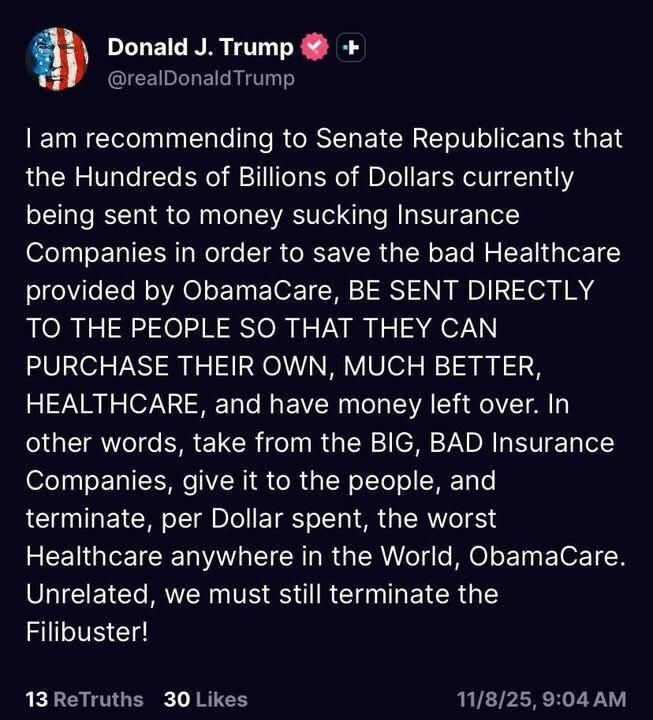
I think it’s worth drilling down on what this would actually look like in practice.
We spend hundreds of billions subsidizing healthcare, but most of that money flows to large corporations, hospitals and insurance companies, rather than to patients. If those funds were directed to patients instead, they’d finally have the power to choose the care they want.
Insurance would still play a role, but people would have far more freedom in how they use it. Generous subsidies could go into HSAs, which patients could then use to buy insurance and pay cash for routine services that don’t need it. Basic labs and office visits don’t need to go through an insurance bureaucracy.
That’s how other kinds of insurance work: car insurance doesn’t cover oil changes. Health insurance should protect against major, unexpected expenses like cancer or trauma, not everyday care.
Let people shop for routine services, keep coverage for the big stuff, and give subsidies directly to patients. It just makes more sense than the current system.

233
496
2,206
172,194
David H. Haase, MD retweeted

8 Nov 2025
I don’t know, Professor. Because in Michigan, it’s, illegal to find out.
Your employer, @UMich lobbies the state to keep it that way.
Michigan has “Certificate of Need” laws. Sounds bureaucratic. It’s not.
It’s a permission slip system where health systems get to decide if their competitors can exist.
Want to open a clinic?
Nursing home?
surgery center?
Imaging center?
You need permission from a state commission, staffed by representatives from existing health systems and the carriers.
Want to add an Operating Room to compete?
Same commission.
Same conflicts.
Want to offer a new service?
You’re asking your competitors for permission.
The university, your employer, aquired hundreds of independent physician practices across Michigan
It has used CON laws to block new competing facilities from opening
It converted the practices, so now they bill at Health Systems rates and easily raised prices 5x overnight.
Just acquired Sparrow Health System in 2023, making U of M a $7 billion organization.
Same doctor.
Same procedure.
Same building sometimes.
Different owner.
Different price.
Not because the quality changed. Because the competition was made illegal.
University of Michigan Health now generates $7 billion in annual revenue across 200 care sites statewide.
They pay zero property taxes on 3.5 million square feet of real estate.
They’ve issued $3.2 billion in tax-exempt bonds meaning Michigan taxpayers subsidize their construction costs.
They receive hundreds of millions in Medicaid supplemental payments (DSH, GME, UPL) every year.
And here’s the kicker:
According to the Lown Institute, U of M Health has a $284 million fair share deficit.
That means the tax breaks they receive exceed the charity care they provide by $284 million.
University of Michigan is a $7 billion tax-exempt empire that uses government power to eliminate competition, then calls it healthcare.
One more thing:
U of M Health operates 340 contracts with 340B pharmacies.
The 340B program was created by Congress to help safety-net hospitals serve poor patients.
The University buy drugs at a discount, then are supposed to pass those savings to patients.
U of M turned it into a profit center with 340 locations.
The discounts don’t go to patients.
They go into the $7 billion revenue pile.
So back to your question, Professor:
“Will giving people money instead of insurance subsidies lead to better functioning markets?”
I don’t know. Because in Michigan, it’s illegal to find out.
Your employer, now a $7 billion organization lobbies to maintain Certificate of Need laws that make it a crime for physicians to compete on price, quality, or service.
I’ve built health plans with no copays, no deductibles, no prior authorizations.
Direct contracts between employers and physicians.
Transparent pricing.
Bundled payments.
They work. Prices drop 30-40%. Quality goes up. Premiums go down. Patients love them.
So before you lecture Americans about “adverse selection” and “market failure,” maybe explain why the University of Michigan gets to use state violence to prevent markets from existing in the first place.
You’re not teaching economics, Professor.
You’re teaching people how to defend a monopoly while collecting a paycheck from it.
8 Nov 2025

Econ 101 midterm question: Based on what you know about risk pools and adverse selection in healthcare markets, will giving people money instead of giving them money to buy health insurance lead these markets to function more effectively, or will it just lead more people to be uninsured?
101
401
1,471
110,886
David H. Haase, MD retweeted
2 Nov 2025
“Medicare for All” sounds great.
Free healthcare for everyone, what’s not to like?
But here’s what the cheerleaders don’t tell you:
Medicare only pays about 80% of your bill.
There is no cap on what you could owe.
So, if you get cancer and treatment costs a million dollars, you’ll owe $200,000.
That’s not “universal coverage.”
That’s a government plan that leaves you broke.
And while politicians promise to expand it, they quietly outlawed the one kind of plan that actually limits your costs.
Let’s talk about what “Medicare for All” really means.
47
78
313
16,456
2 Nov 2025
life is not fair, but it's beautiful #life #positivity #positivevibes #s... youtube.com/shorts/nqF3D4Juq… via @YouTube
48


David H. Haase, MD retweeted
19 Oct 2025
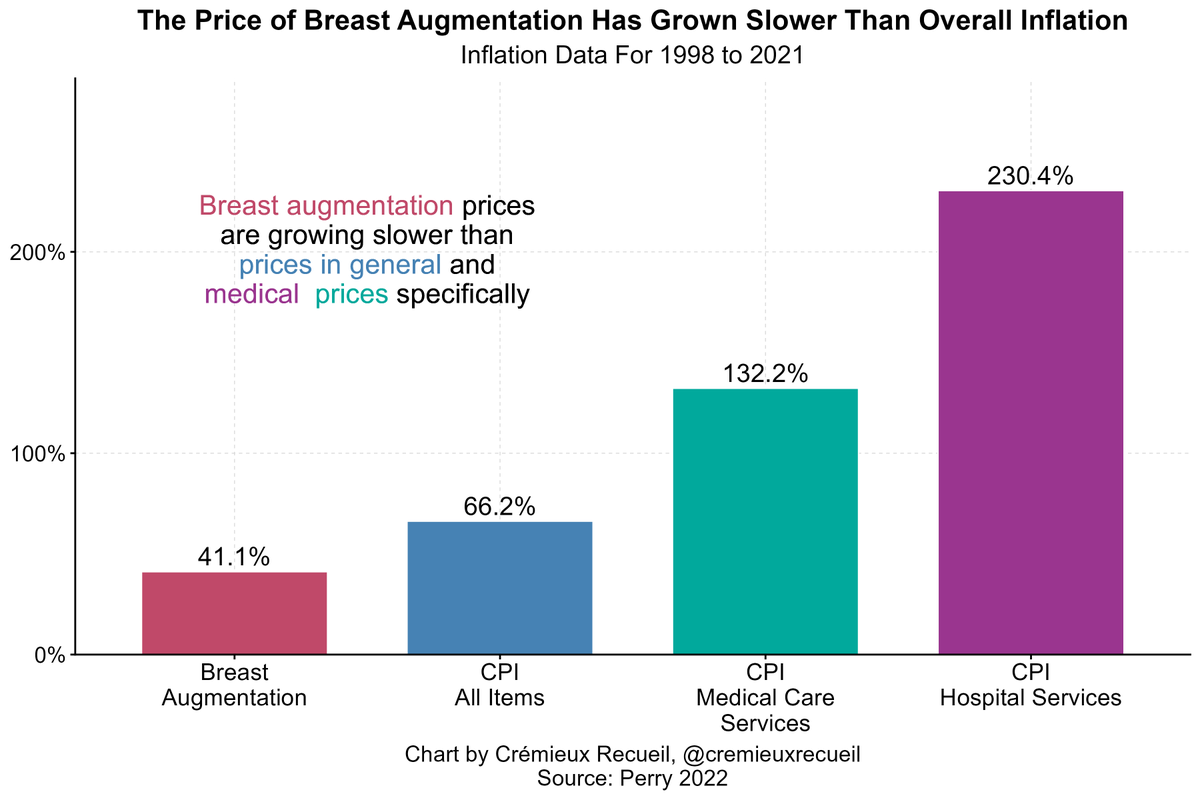
Quality and cost improve where there’s a free market.
LASIK and cosmetic surgery prove the point.
Want people to experience similar improvements in chronic disease management? Unleash the market.
19 Oct 2025

Boobtech is amazing.
It's an area that the rest of medicine could look to as an example.
The professionals making bigger, more realistic breast implants are simultaneously improving affordability, safety, and quality at a rapid rate🧵
9
33
166
14,362
David H. Haase, MD retweeted

21 Aug 2025
Incredible insights from @DavidHaaseMD, CEO and Founder of @MaxWellClinic, yesterday.
"Our body has way more capacity for healing than the current system has capacity for."
This perspective really resonates with what we are doing at @seed_healthcare.
We must continue to push healthcare beyond its limits- beyond symptom management, beyond narrow interventions, and toward embracing the deeper potential of human health and well-being.
#healthcare #innovation #wellbeing #healthcareventure
1
4
85