
PhD. Clinician-Scientist. Gamer. Chicken-herder. CCI ADHD EDS TBI TN 🏳️🌈
Joined April 2021
- Tweets 17,432
- Following 905
- Followers 11,158
- Likes 34,411
210 Photos and videos







Pinned Tweet

3 Apr 2022
What would happen if we stopped praising people for pushing through and started praising people for taking care of themselves and being mindful of the limits?
81
1,694
7,448
Wait… people know “brain retraining” programs don’t have ANY sound scientific support, right? All of the studies I’ve seen were so poorly designed I wouldn’t count them as evidence and they were conducted by people making tons of money off of marketing these “treatments” to vulnerable communities (i.e., heavy bias). Is that really what the guy is referencing in that long covid article?? I haven’t had the energy or time to read it
6
28
149
3,097
I used to have social anxiety that was so severe I avoided talking for full days when I was in middle school.
Sometime in high school I stopped giving a fuck and the social anxiety for the most part vanished.
Now, as I deal with brain fog and cognitive deficits that are so severe I have significant problems with word finding and comprehension at times, I’m noticing bits of the social anxiety coming up again.
Of all of the aspects of disability that I’ve had to accept, accepting the cognitive deficits has been the hardest one. You would think that my brain injury and ADHD would’ve made it easier, but no. And especially not when your job relies on verbal communication such as in a healthcare setting.
1
26
742
Providers being afraid of writing accommodation letters or filling out FMLA paperwork for a new patient is hilarious to me. Like what do you think is going to happen? They might get accommodated and not lose their job and the company will sue you because how could you possible assess the state of a patient in a single appointment (where you are expected to do exactly that) 🫠
2
1
39
1,384
Scent is a disability rights issue.
This includes perfume, air fresheners, scented hair products, scented deodorant, scented lotion, and yes, even essential oils.
Not only are they harmful and even potentially dangerous for some disabled people, mounting evidence suggests scents are likely harmful for people in general. So, please, be mindful of your scent in public spaces
12
39
273
9,224
This person is sharing information on Lyme treatments that appears to be false and even dangerous, suggesting that using generally supported and accepted methods such as a single dose of an antibiotic to try to prevent Lyme after a tick bite is worthless simply because two physicians wrote a letter to the editor suggesting more evidence was needed to support the practice.
I tried to politely engage, pointing out that saying there’s insufficient evidence for a preventative treatment that is hard to study in any controlled fashion does not equate it being worthless nor substantiate such a claim and I was blocked. Yikes 😬
ALT Disabled Doctor @DisabledDoctor • 22h So the study suggests an approximate 25% failure rate. No one is saying it doesn't fail. Your argument seems to be it is worthless and, as far as I can tell, you have no evidence to support that claim Dana Parish • @danaparish "As far as I can tell" comprehend? X.com ) Can you read QT underneath: Dana Parish @danaparish• 1d No. It's not good evidence. "Protected" = NO culturable Lyme in ear/bladder/heart tissues at ~4 weeks. V short timeframe in the world of BB. Misses low-level/persistent infection, dormant persisters & dissemination that standard culture can'…
2
8
256
For the 50th time, Covid conscious community, PLEASE stop with the Covid to HIV/AIDS comparisons. HIV is not as comparable to COVID as it is to other diseases and your desire to leverage the stigma of HIV to get people to take covid seriously is not only completely misguided, it’s ableist and bigoted. Cut that shit out
May 27

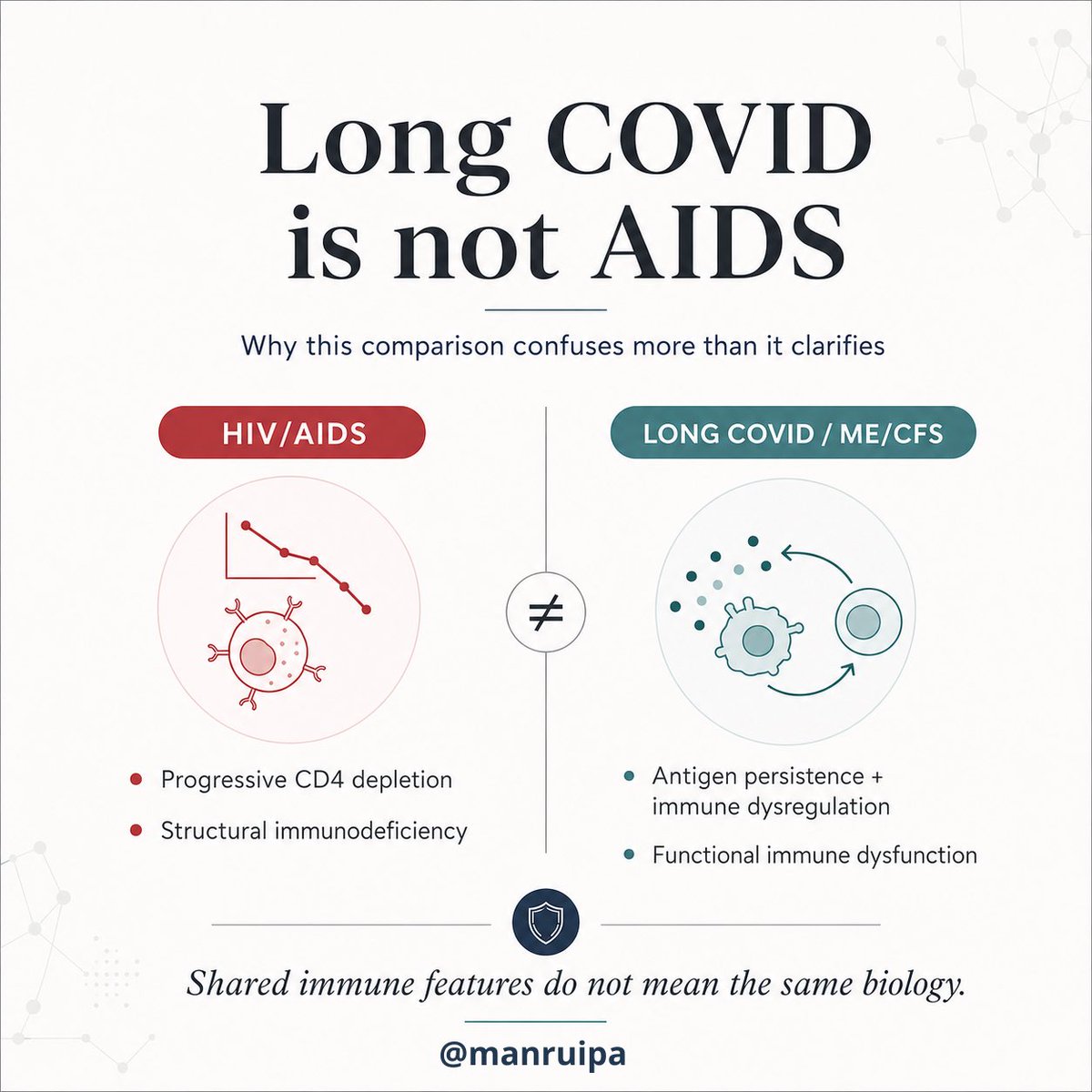
⚠️🚩Long COVID is not AIDS: why this comparison confuses more than it clarifies
Following the huge debate that has emerged around this topic, I’m going to explain in more detail why Long COVID, ME/CFS, and AIDS are not the same thing, even if they may share some superficial immunological features.
Mega thread 🧵
I’ve been seeing comparisons between Long COVID, ME/CFS, and HIV/AIDS for quite some time. I understand where they come from: chronicity, immune dysfunction, T-cell exhaustion, viral reactivations, persistent inflammation. All of that exists. But the problem is that sharing downstream immunological features does not mean we are dealing with the same biology, the same clinical trajectory, or the same type of immunodeficiency. That is where the comparison breaks down.
And yes, to be rigorous, it should be stated properly: HIV is the virus and AIDS is the acquired immunodeficiency syndrome to which untreated HIV infection progresses. But precisely because so many people on social media use “HIV” when what they really mean is the immunodeficiency state caused by CD4 depletion, it is worth clarifying why Long COVID and ME/CFS do not behave like AIDS, even if they may share some features of chronic immune dysfunction.
The main difference is this: in untreated HIV infection, the dominant axis of the disease is the progressive destruction and numerical depletion of CD4 lymphocytes, eventually leading to AIDS, which is defined, among other things, by a CD4 count below 200 cells/µL or by stage 3-defining illnesses. That progression leads to a classical, structural acquired immunodeficiency, with real loss of the CD4 compartment.
By contrast, in Long COVID and in many cases of post-infectious ME/CFS, the dominant pattern appears to be different: antigen persistence or sustained antigenic stimulation, chronic immune activation, altered inflammatory pathways, exhaustion signatures, immune dysfunction, and, in an important subgroup, autoimmunity. In other words, immunodeficiency may be present, but it is often a functional immunodeficiency due to exhaustion and dysregulation, not an immunodeficiency whose central axis is the massive destruction of the CD4 compartment. This is not a simple copy of HIV; it is a different type of immunopathological chronicity.
The first major difference is temporal and clinical. In HIV infection, there is often an initial phase that is relatively nonspecific or even asymptomatic, and the major consequences appear later, as CD4 depletion progresses. In Long COVID and ME/CFS, symptoms usually appear immediately or shortly after the triggering infection. That difference alone should already make us cautious about the comparison. From that perspective, Long COVID and ME/CFS resemble a kind of chronic infectious mononucleosis-like state much more than AIDS.
And that matters a lot immunologically. Infectious mononucleosis caused by EBV is characterized by a marked expansion of mononuclear cells, especially CD8 T lymphocytes, and by an intense inflammatory response. In that context, IFN-γ rises, the antigen-presentation machinery is amplified, and an environment is created in which CD4 cells are not disappearing, but rather actively participating in the response. Precisely for that reason, EBV infectious mononucleosis has been linked to a higher later risk of autoimmune diseases and to the pathogenesis of multiple sclerosis.
Continued in the next post ⬇️
1/
3
7
25
2,262
The fact that I now need to drive 3 hours round trip to get to the dentist for a filling because they are the only dentist in the area that I know of that actually implements any disease prevention protocols (masking etc.) is a great little example of disability tax and how everyday casual ableism makes disabled people’s lives harder.
People could do better. Easily. They just choose not to
6
39
230
3,155
Because physicians are often terrible at delivering bad news to patients and even worse at recognizing their own biases that cause them to downplay things or not evaluate the situation (or the research) properly — inadequate scientific training and having a trade degree that no one tells you isn’t a scientific degree will do that to you.
Telling patients the reality of their health situation and what their physicians neglected to tell them (but put in their chart) was half of my job when I worked at the VA.
May 15

A cruise (several days or weeks eating and socializing in confined spaces) is arguably much worse than a birthday party. So why would you expect only transmission via close contact and tell fellow cruise passengers that they are at low risk?
x.com/Ayjchan/status/2054902…
5
2
20
981
Disabled Doctor retweeted

May 13
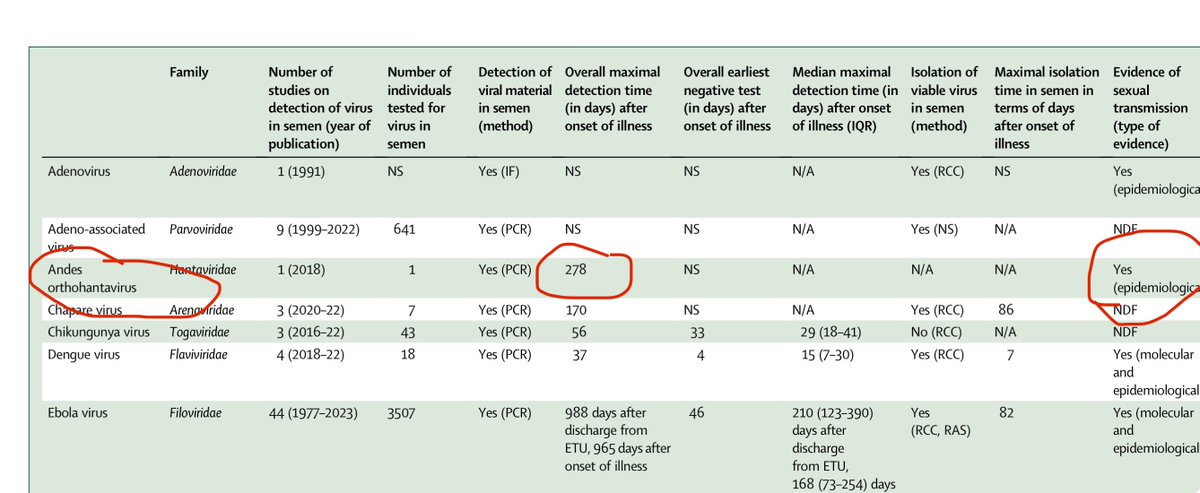
If it were true, all the Joe Rogan manosphere men would immediately want a lockdown and wear N95 masks. 💡But wanna know what is true… hantavirus RNA can persistent in human semen for 9 months after infection…
A 2024 systematic review in The Lancet Microbe analyzed viral persistence in semen across many viruses. Andes virus is a notable exception with documented long-term RNA presence of 278 days—plus the Andes hantavirus is documented to be sexually transmissible.
27
170
522
42,259
You know what’s worse than social judgement or embarrassment??
Dying or giving someone else a life threatening disease.
Put on a fucking mask, you absolute babies
25
145
691
5,155
Disabled Doctor retweeted

Have seen more than one post calling people brain damaged, crazy, stupid, etc.
No thanks.
Alternatives you can use for these phrases include:
ignorant, unprepared, missing context, sharing misinformation, not based on facts, unreasonable, ridiculous.

CC community: please keep your ableism and sanism in check while discussing the hantavirus situation. If you could even just pretend to be in community with disabled people for a little while that would be great. Thanks!
1
4
15
379
I’ve been in an off and on severe flare since we moved in late February and I was set to try to take on a few new patients soon but I’m accepting that I need to delay them more as I’m barely getting by with my caseload as is.
It sucks though. It’s so hard to balance caring for and accommodating myself while also trying to do my best to support patients and take on new ones who I know have few to no other options for care.
I beat myself up a bit even though I know better than most how unhelpful that is. I often wonder if I’d have such a hard time setting these limits for myself if I did anything else for work. But, here we are, and I’m just doing my best. We desperately need more disabled healthcare providers
4
2
33
1,106
CC community: please keep your ableism and sanism in check while discussing the hantavirus situation. If you could even just pretend to be in community with disabled people for a little while that would be great. Thanks!
4
35
151
3,917
Disabled Doctor retweeted

May 11
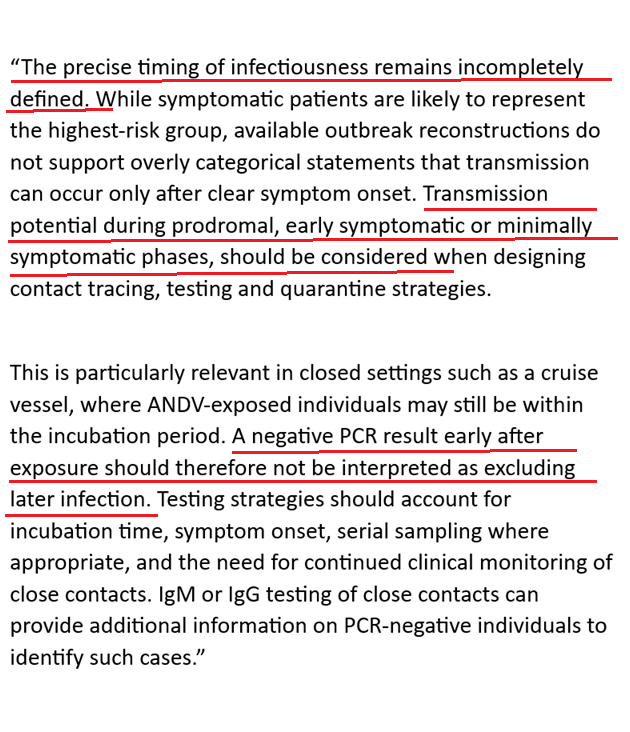
There is growing evidence from the ship that you probably don't need "prolonged close" contact to spread the virus.
And the implications here are pretty clear
If we are serious about ending this outbreak, all the passengers should undergo a full quarantine away from others
141
592
3,415
299,425
Funny enough, I’m not worried about hantavirus. I wear a fit tested respirator. I’ll probably be fine.
I am concerned for all the assholes who refuse to mask and for the disabled and vulnerable people who cannot mask that they might infect.
This isn’t about anxiety, it’s about common sense and protecting those who cannot protect themselves (disabled people, infants, etc.). It’s about being part of a community and helping one another. If something as simple as masking might keep others from dying and a person isn’t willing to even consider it because they refuse to deal with their own trauma around COVID, that person is a raging piece of shit who doesn’t know how to (and honestly maybe doesn’t deserve to) live in community with others.
11
25
204
4,620

Andes virus/Statement from the International Hantavirus Society
-Current evidence does not support describing Andes virus as 'barely transmissible'
-Transmission potential of asymptomatics should be considered
-A negative PCR result doesn't exclude infection
1/2
25
439
1,405
86,958
Friendly reminder that MDs are trade degrees and they receive little to no scientific training.
The scientific training they do receive, if any, is generally from other MDs who also have little to no training.
This is why MD/PhD combo degrees exist (because an MD isn’t adequate for scientific pursuit).
When it comes to issues like what we are facing now, look to the scientists, not the know-it-all MDs who are so poorly trained that they don’t even understand what they don’t understand.
May 8

There is literally nothing to worry about, calm down. x.com/KenDBerryMD/status/205…
14
131
678
16,880