
Joined June 2016
- Tweets 2,867
- Following 1,491
- Followers 5,730
- Likes 11,011
222 Photos and videos


Dr Sarah Sammons retweeted

We are optimizing treatment for young onset CRC but 41% are walking in emotionally distressed & only 27% get the support they need.
The tumor is not the only target.
Nice report on how dedicated navigation services improve supportive care access
ascopubs.org/doi/abs/10.1200…
2
3
169
Dr Sarah Sammons retweeted

Jun 14
The Evolving Evidence on Weight Loss Interventions in Breast Cancer - Neil Iyengar (@Neil_Iyengar)
oncodaily.com/voices/neil-iy…

2
6
194
Dr Sarah Sammons retweeted

MAID program (Medical Assistance in Dying) is the topic of next week's #HealthcareUnfiltered. It's an important topic to address.
what is it? who qualifies? is it good? bad? why and why not?
As more states are legislating MAID, tune in Tue to learn more.
Pls subscribe & share.
4
15
1,127
Dr Sarah Sammons retweeted

Jun 13
Thanks so much. Was definitely a group effort. Despite the trial outcome, there is a great need to identify new approaches to optimize scalp cooling efficacy.
1
3
549

Jun 12
I really wish cool capping had worked for TDXd but we did not see benefit. Not surprising given long half life of drug.
Amazing effort @esalehiDNP and the whole @DFCI_BreastOnc team.

New study now out in @ESMO_Open looking at #ScalpCooling outcomes in patients receiving trastuzumab deruxtecan for #MetastaticBreastCancer
🔓pubmed.ncbi.nlm.nih.gov/4225…
@esalehiDNP @elmayermd @DrKateDibble @drsarahsam @NabihahTayob @stolaney1 #MBC #TDXd #BreastCancer #ColdCaps #ADCs

4
8
28
3,490
Dr Sarah Sammons retweeted

Jun 11
Whether it’s 3 pointers, Jiu Jitsu or surgery it’s all about volume volume volume .
I always tell my med students to find the neurosurgery program that will give them the highest and most diversified surgical volume , not the research powerhouse.
Jun 11

One realization I’ve made from 20 years on the job: many docs who trained at prestigious centers had to fight for procedures, and came out with a shiny resume but weak skills.
Can’t speak for surgeons, but if you want an ED doc who can intubate a mosquito, can insert a central line eyes-closed in under 30 seconds, and can calmly run multiple codes simultaneously while strolling from doorway to doorway, they typically do not come from the places a layperson would think of.
6
4
88
13,471
Dr Sarah Sammons retweeted

Jun 11
Interesting press release by Alphamab: the biparatopic HER2 mAb KN026 improved PFS vs HP when combined with a taxane in the CLEOPATRA regimen (1L HER2 MBC). alphamabonc.com/en/html/news…
1
11
39
5,478
Dr Sarah Sammons retweeted

Jun 11
This. Every word of it.
Since Amy died, I’ve found myself doing exactly what Abigail (@AMJohnston1315) describes, replaying conversations, scrolling through years of text messages & emails, wondering if she knew how much she was loved.
The tragedy is that after someone dies, there is no final survey question, no debrief, no certainty. There is only the relationship as it was lived.
A beautiful & 💔 reflection on grief, friendship, & the impossible questions we ask ourselves after losing someone we love.
And yet, somehow, we keep showing up for the people we love who are still here, in the best way we know how, hoping it’s enough. Read it 👇🏻
#bcsm
#griefandloss
#metastaticbreastcancer

New blog post all about the dark nights of the soul when a dear friend has died … nohalfmeasures.blog/2026/06/… #bcsm
2
3
19
1,874
Jun 11
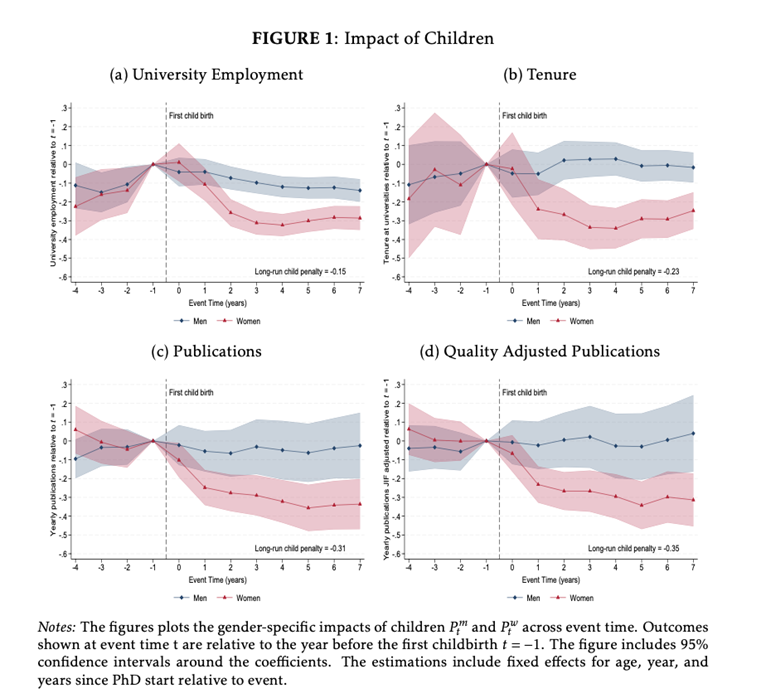
The clear problem is for women after children in academia.
Academic careers after children are possible but are best achieved with a good partner, great childcare and a strong social network. This all-star line up is hard to achieve for the best of us.
We need to start a curriculum.

Children derail academic careers even in places with good social nets, like Denmark
2
8
49
5,413
Dr Sarah Sammons retweeted

Invasive Ductal Carcinoma is a spectrum of disease—ranging from well-differentiated tumors to high-grade, aggressive variants. Check out the Substack for a deep dive! 🔽🔽🔽
open.substack.com/pub/thepat…
#PathX #DiagnosticPathology #BreastPath

5
12
1,144
Dr Sarah Sammons retweeted

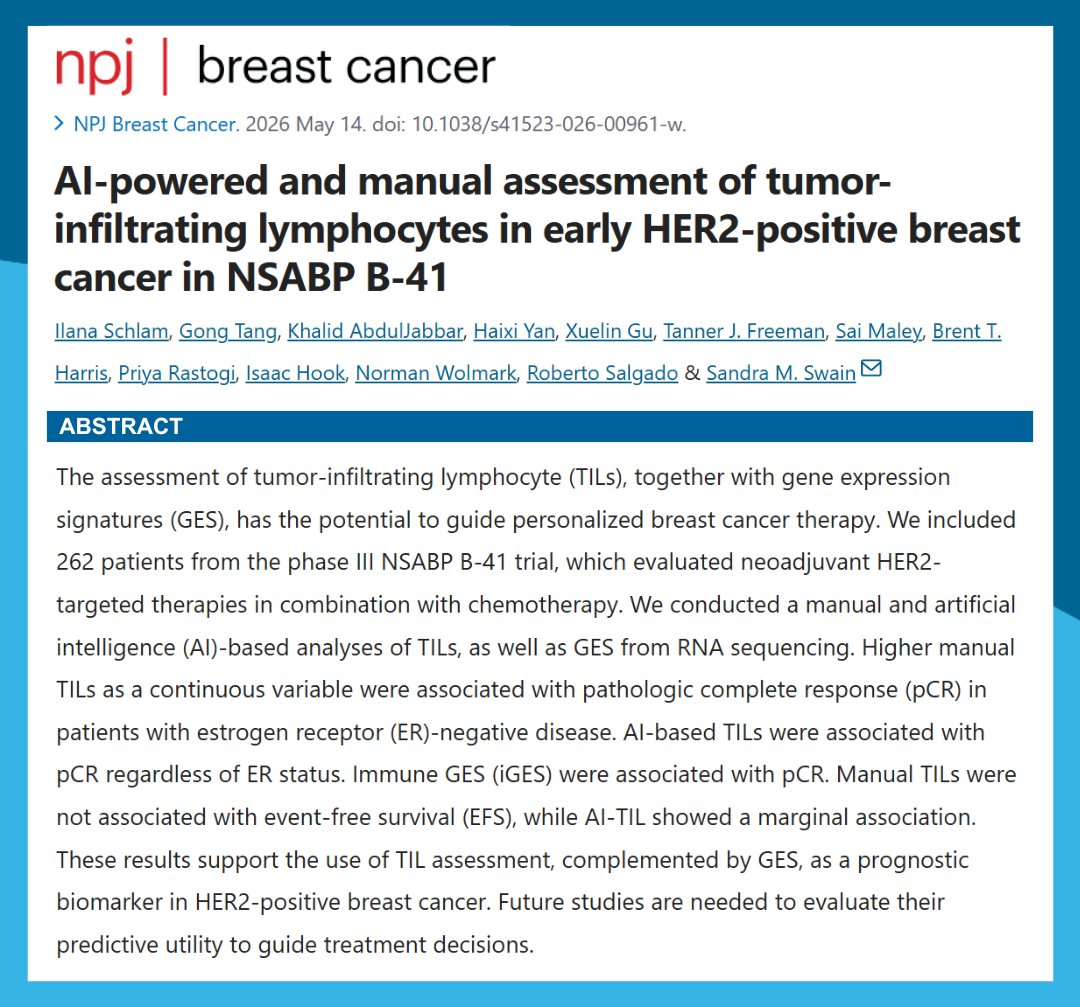
Check out this new @Nature_NPJ study looking at AI-powered and manual assessment of #TumorInfiltratingLymphocytes in early HER2-positive #BreastCancer in NSABP B-41.
🔓pubmed.ncbi.nlm.nih.gov/4213…
@IlanaSchlam @khalidated #TILs
1
6
9
2,082
Dr Sarah Sammons retweeted

Jun 9
When this article was published about a month ago, I outlined the main methodological concerns on X.
One month later, four comments have accumulated on the article’s online page. After reading them, it is hard not to ask a very simple question: how did this study pass editorial and peer review in its current form?
For those who have time, I would strongly recommend reading the comments under the article. My comment was probably the most superficial one; the more substantial and technically important critiques are in the other comments.
jamanetwork.com/journals/jam…
May 12

Survival and Recurrence With GLP-1 Receptor Agonists in Breast Cancer
A provocative signal, but not yet an anticancer effect
1. Retrospective EHR-based study; association does not prove causality.
2. High risk of residual confounding despite propensity score matching.
3. Possible healthy-user effect: GLP-1 RA users may have better follow-up, access, adherence, and metabolic care.
4. Strong calendar-time bias: GLP-1 RA use increased in more recent years, when breast cancer care also improved.
5. Weak exposure definition: ≥2 prescriptions do not prove sustained treatment.
6. No time-varying exposure model; immortal-time bias may persist.
7. Landmark analyses reduce bias but do not replace proper time-varying modeling.
8. The signal weakens against the active comparator SGLT2 inhibitors.
9. Insulin/metformin is a problematic comparator because it may represent a sicker diabetes population.
10. Limited tumor biology: ER/HER2 status, grade, nodal burden, tumor size, Ki-67, and genomic risk are inadequately captured.
11. ER-positive rates appear unrealistically low, suggesting incomplete EHR capture.
12. Cancer treatment data appear incomplete; surgery and radiotherapy rates look clinically implausible.
13. RFS is code-based, not a true clinical recurrence endpoint.
14. No breast cancer–specific survival; all-cause mortality may reflect cardiometabolic benefit rather than anticancer effect.
15. No competing-risk analysis despite substantial non-cancer mortality risk.
16. No weight-loss data; the actual metabolic effect is unknown.
17. Effective follow-up is short despite reporting 10-year estimates.
18. Few patients remain at risk beyond 5 years, weakening 10-year KM estimates.
19. High administrative censoring limits late outcome interpretation.
20. Mechanism remains unclear: anticancer effect, weight loss, metabolic control, or patient selection?
jamanetwork.com/journals/jam…

2
14
51
11,663
Dr Sarah Sammons retweeted
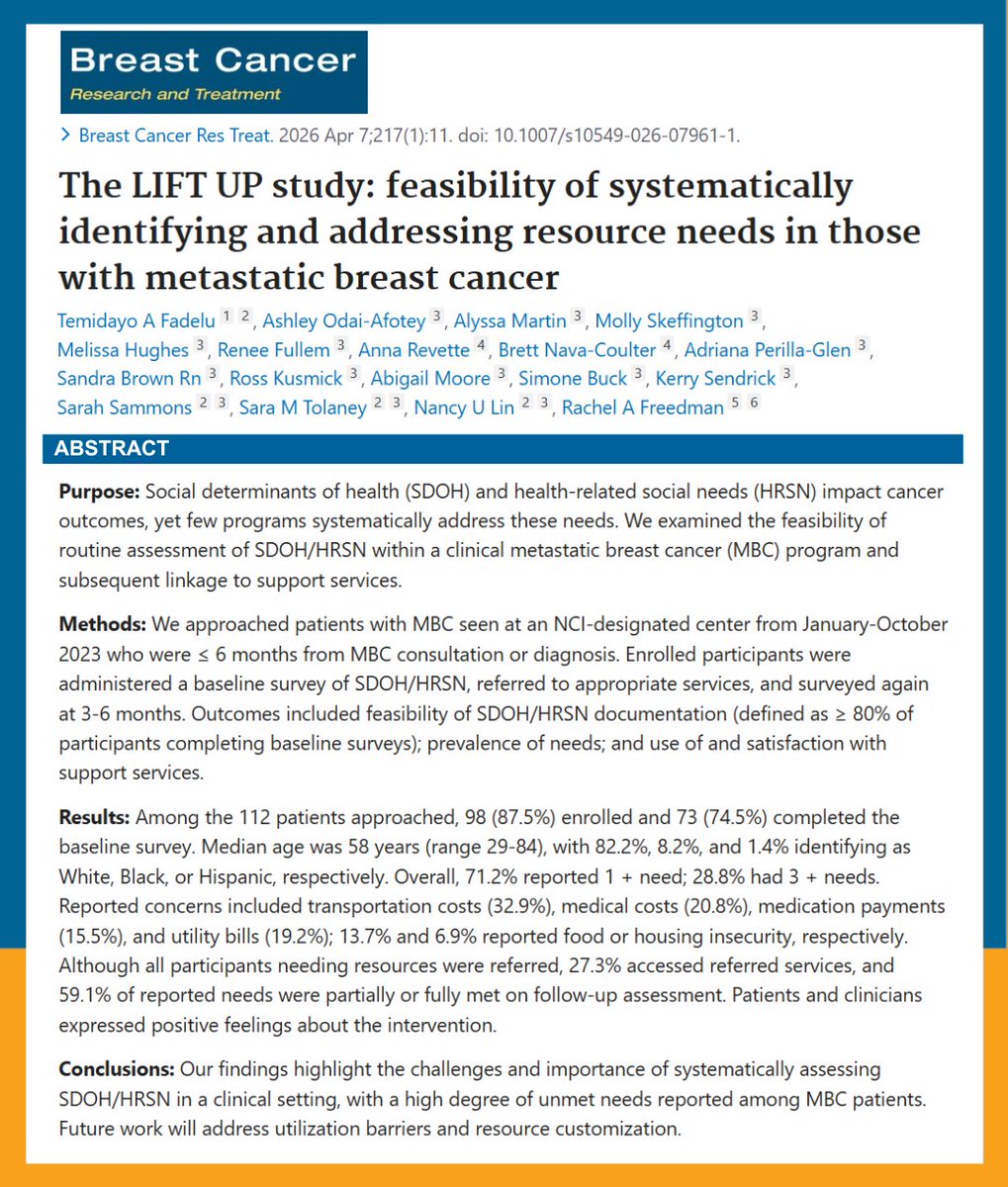
Check out the recently published LIFT UP study, which examined the feasibility of systematically identifying and addressing resource needs in those with #MetastaticBreastCancer.
👉pubmed.ncbi.nlm.nih.gov/4194…
@AshleyOdai @aperillaglen1 @drsarahsam @stolaney1 @nlinmd @DrRFreedman #BreastCancer #MBC
#SocialDeterminantsOfHealth #SDOH #HRSN
1
7
7
669
Dr Sarah Sammons retweeted
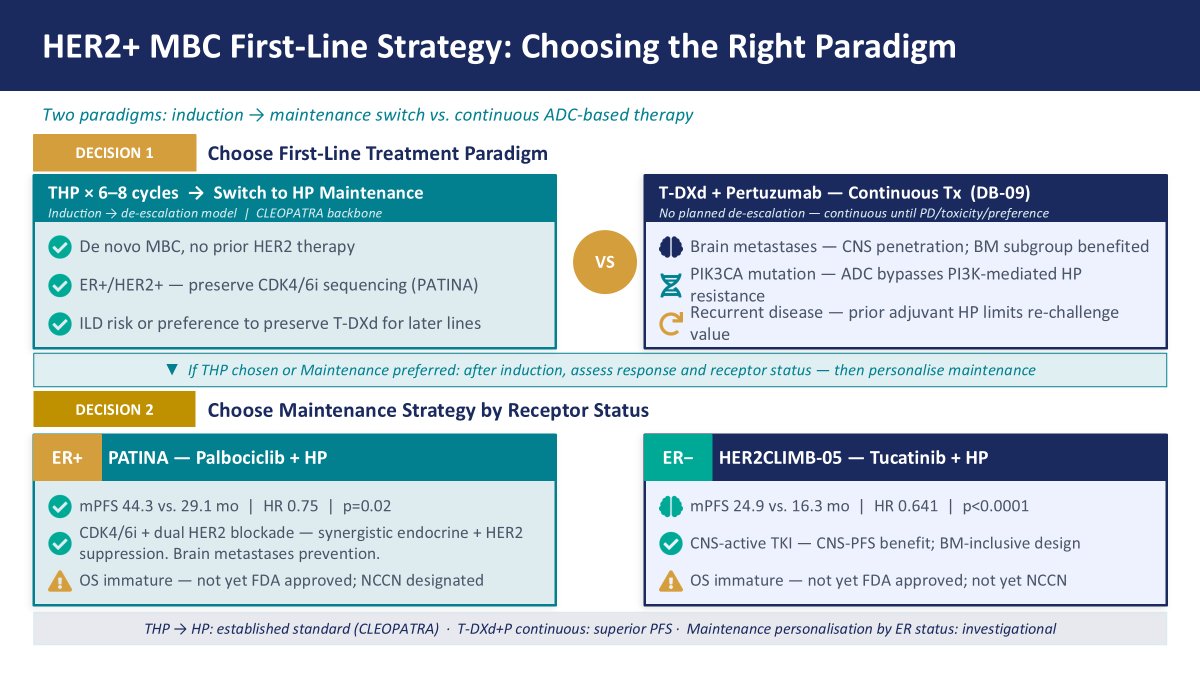
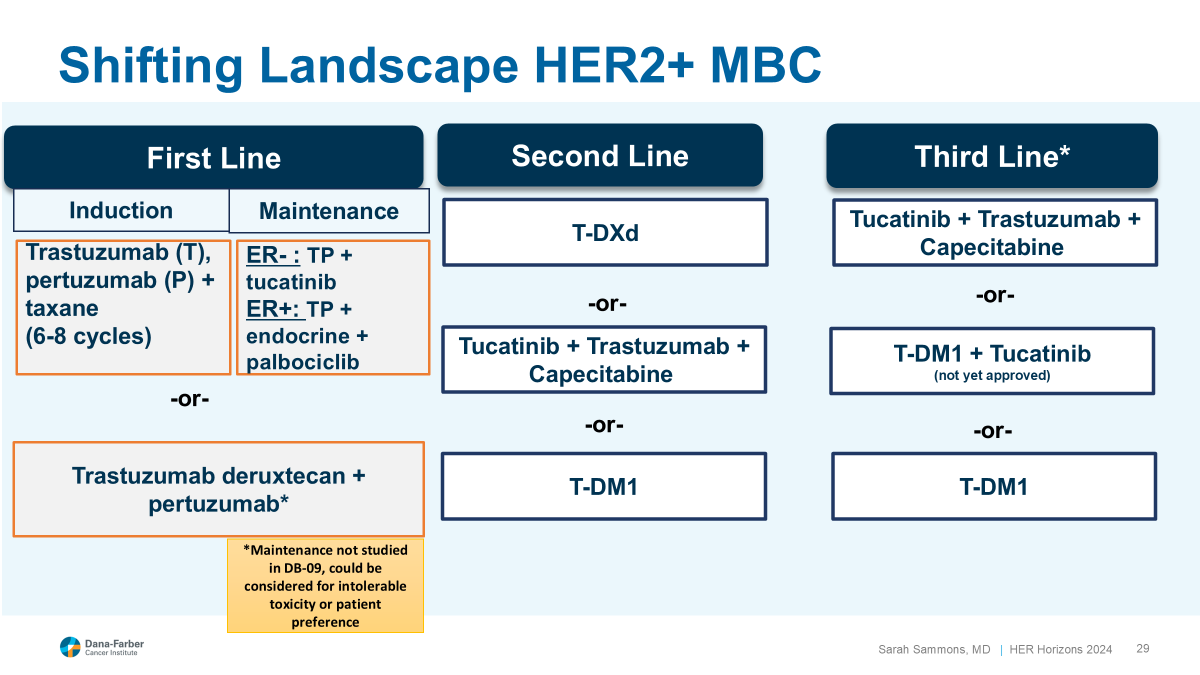
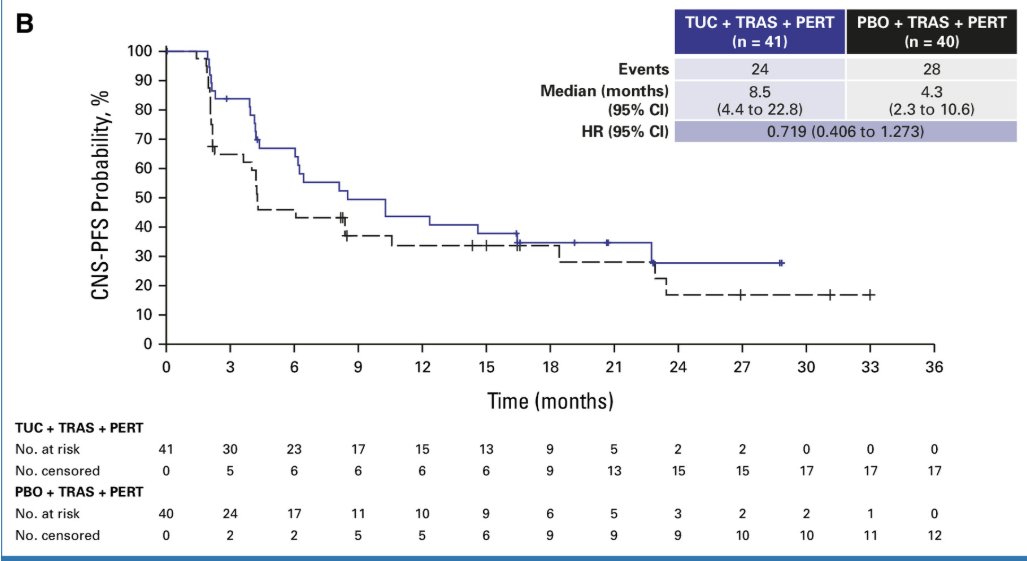
Drs. Waks (@adawaksmd) and Sammons (@drsarahsam) introduce a patient case of a 62‑year‑old woman with HER2 /HR- #breastCancer. They discuss how to select an optimal first‑line regimen for her amid an expanding range of therapeutic options. They review and compare data from the DESTINY‑Breast09 and phase 3 HER2CLIMB-05 trials, outlining evidence‑based treatment strategies for this clinical scenario. Watch here ⬇️⬇️
d.peerdirect.com/12482CC01/1…

1
5
9
984
Dr Sarah Sammons retweeted

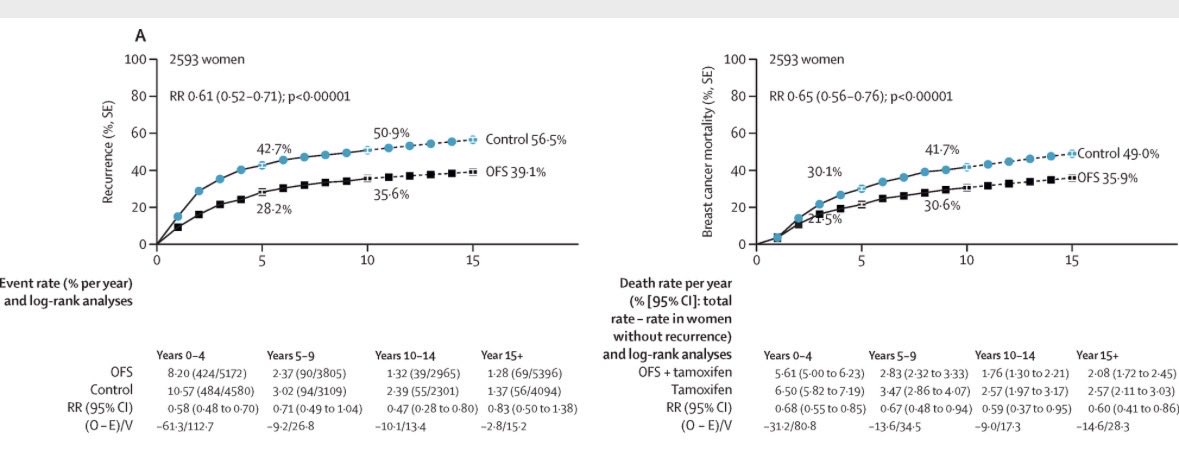
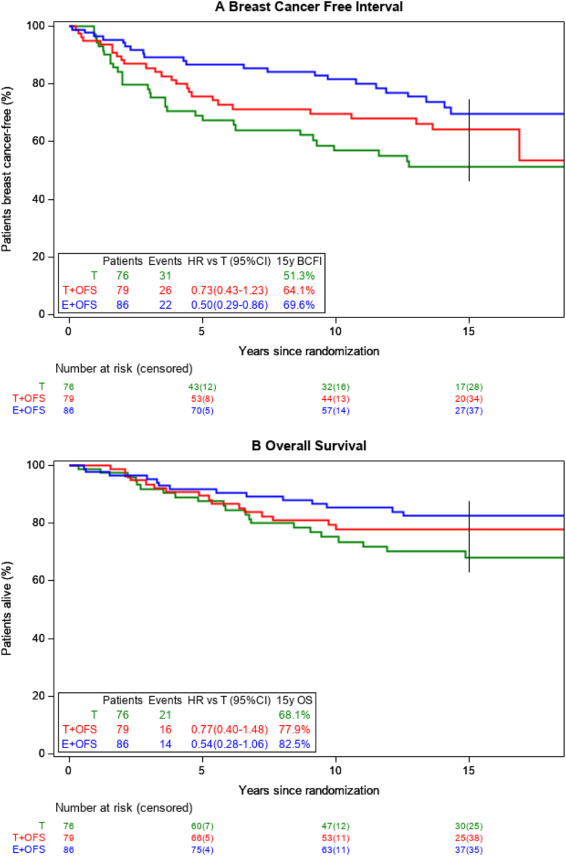
The 15-yr #SOFT/#TEXT data followed nearly 6,000 premenopausal women with HR #breastcancer for up to 17 years.
The critical question: does every premenopausal woman need the most intensive treatment?
For most, the answer is no. If your tumor was small, low-grade, and you didn't need chemotherapy, #tamoxifen alone gave you >94% chance of never seeing your cancer spread. OFS added side effects without adding survival.
But if you were young or had an aggressive tumor, the data tell a different story:
Under 35 with HR HER2- breast cancer: 82.5% alive at 15 years with exemestane OFS vs 68.1% with tamoxifen alone. That 14.4% difference is real lives.
Grade 3 HR HER2- tumor: 9.7% fewer women experienced distant spread and 5.8% more were alive at 15 years with the more intensive regimen.
Yet even here, we are asking young women to accept sudden, severe menopause - bone pain, hot flushes, sexual dysfunction. Prior adherence analyses show ~20% discontinue early. The prescription is only the beginning of the conversation.
The data are 15 years mature. Our job is to use them precisely - and to sit with our patients long enough to make the decision together. We need better risk stratification and protocols to manage the side effects.
How are you framing this risk/benefit discussion in your own practice? 👇
#bcsm #OncTwitter #BreastCancer #MedOnc
Final outcomes of the SOFT and TEXT phase III trials in premenopausal hormone receptor-positive early breast cancer - Annals of Oncology annalsofoncology.org/article…
1
15
55
4,784
Dr Sarah Sammons retweeted

Jun 5
How do you find grit in a resume?
Look for this pattern: multi-year commitments with evidence of progress.


5
66
593
57,392
Dr Sarah Sammons retweeted

Jun 5
A pleasure to participate in this patient facing podcast with my friends @AMJohnston1315 and @drsarahsam! Speaking in my personal capacity, I appreciated the opportunity to discuss how FDA Advisory Committees can support public engagement and bring patient, clinician, and stakeholder perspectives into complex drug regulatory discussions. @FDAOncology @SusanGKomen @BCRFcure @Perlmutter_CC
Have you had a chance to hear @NeilVasan on the Live from Stage 4 podcast talking about the #ODAC vote? Check it out: livefromstage4.org/episodes/… @PIK3CApathbreak #bcsm
1
4
10
1,847
Dr Sarah Sammons retweeted

Jun 4
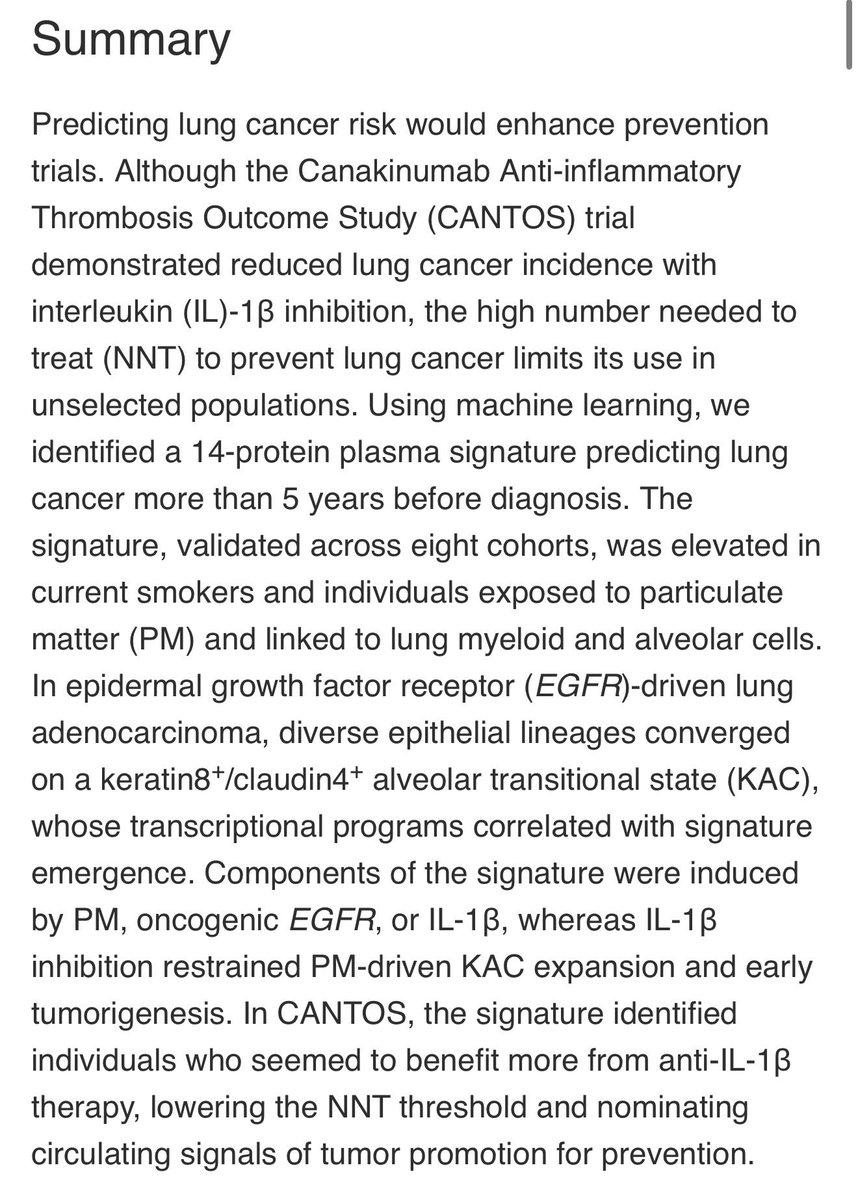
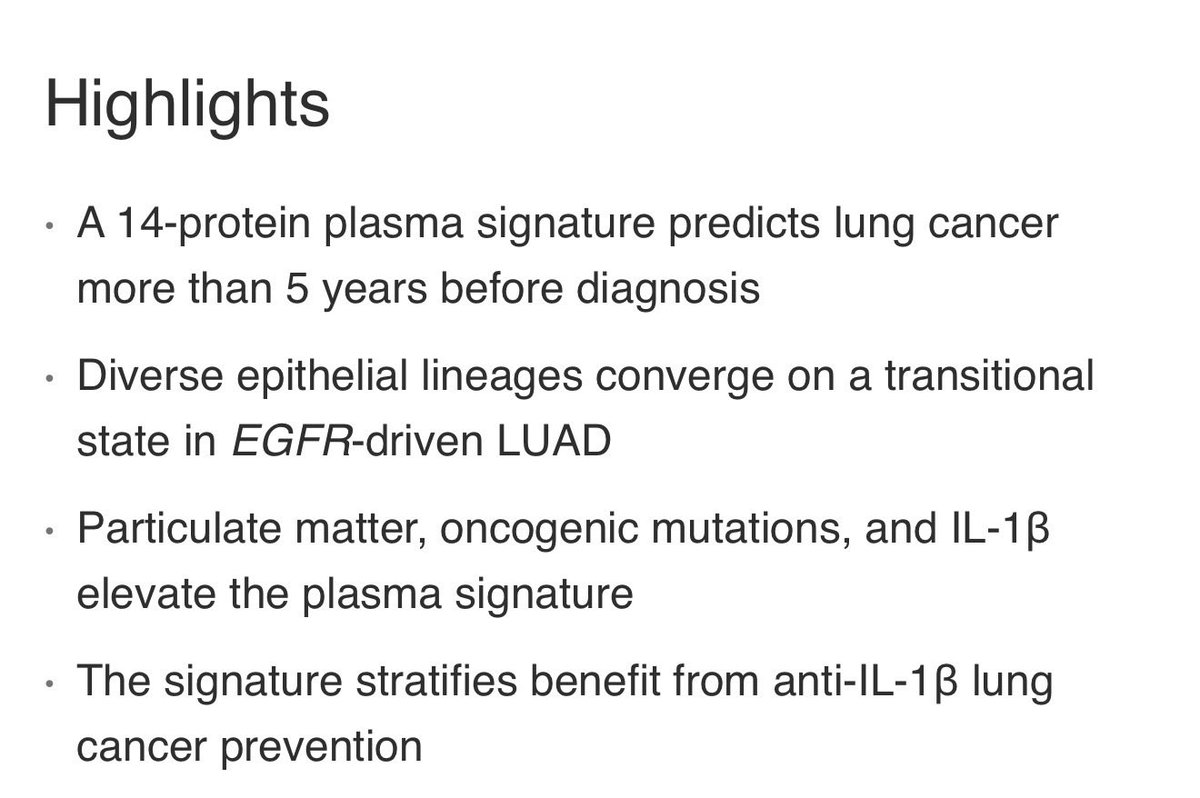
Detecting lung cancer 5 years before it happens, in @CellCellPress courtesy of the @CharlesSwanton group.
Astonishing translational work !
cell.com/action/showPdf?pii=…


4
90
334
26,635
Dr Sarah Sammons retweeted

Jun 4
Finally got our first #pancreaticcancer patient onto #daraxonrasib through @RevMedicines @FDAOncology Expanded Access Program. Turned into an unplanned bring-your-daughter-to-work day to get same-day consent to start therapy. Fingers crossed!

17
33
510
47,508
Dr Sarah Sammons retweeted

🆕 article in press: Final outcomes of the SOFT and TEXT phase III trials in premenopausal hormone receptor-positive early breast cancer @DrHBurstein @LoiSher
doi.org/10.1016/j.annonc.202…
22
48
6,974