
Joined January 2024
- Tweets 2,465
- Following 1,125
- Followers 1,721
- Likes 22,458
179 Photos and videos




FLUTTER retweeted

Jun 11
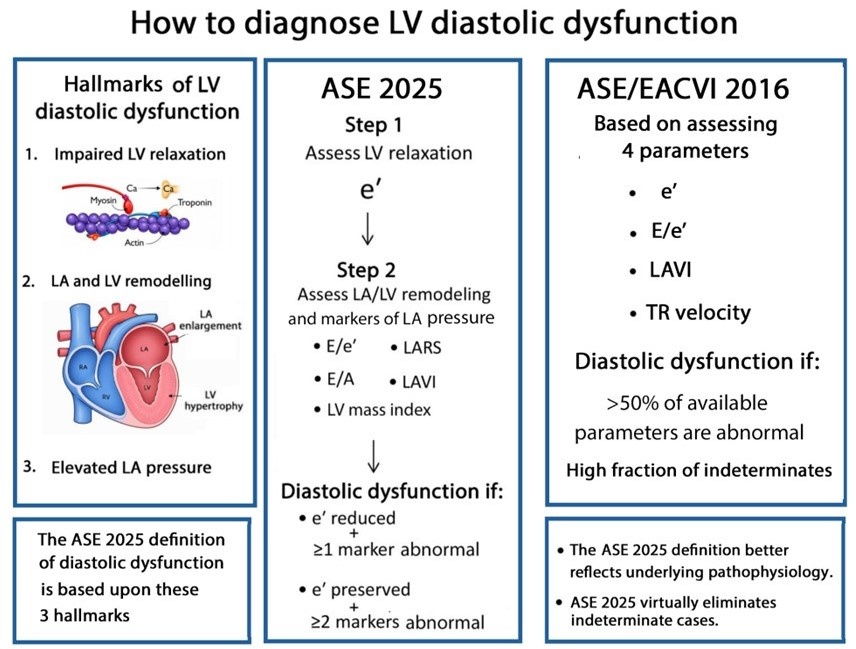
Most echocardiography laboratories have adopted the 2016 diastolic guidelines. With the release of the 2025 update, an important question arises:
What are the key conceptual differences between the 2016 and 2025 approaches to diagnosing diastolic dysfunction?
academic.oup.com/ehjcimaging…
@JGrapsa
12
82
249
16,428
FLUTTER retweeted

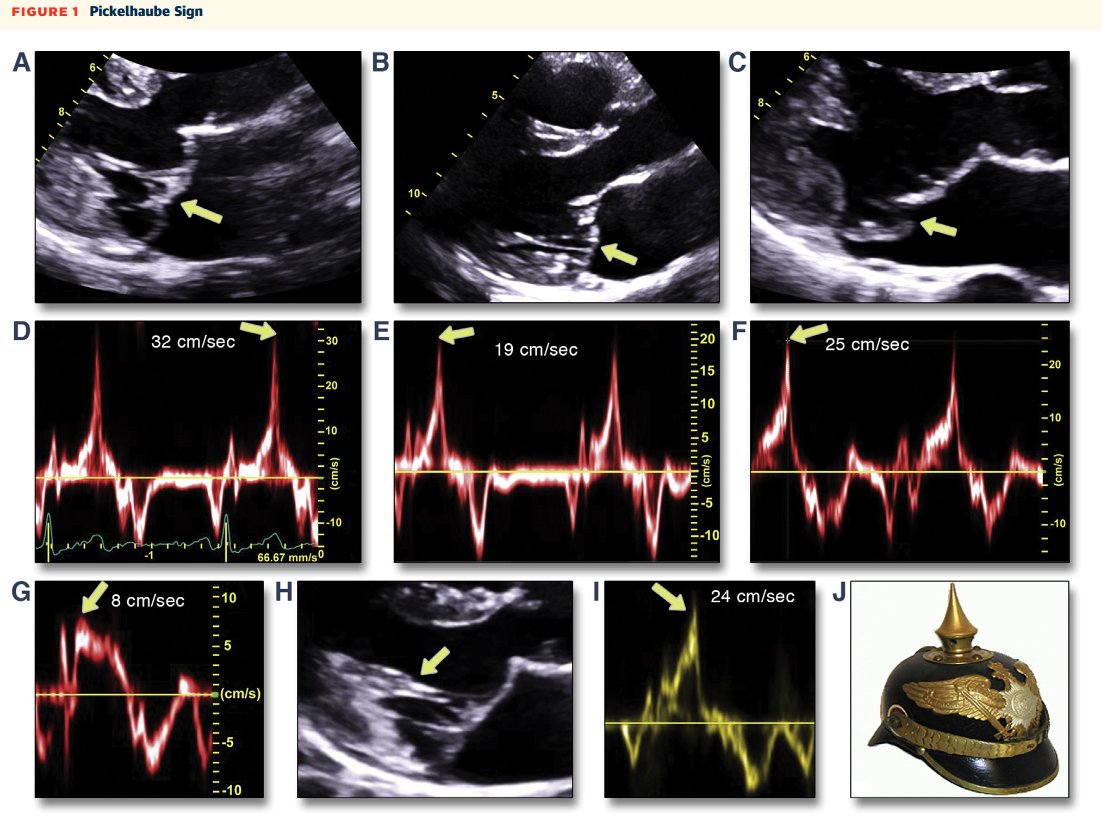
#ASEchoJC The Pickelhaube sign: Lateral annular S′ ≥16 cm/s associated with ventricular arrhythmias in MVP ⚡️
#EPeeps
👉jacc.org/doi/epdf/10.1016/j.…
28
62
2,800
FLUTTER retweeted

May 31
#POCUS #echofirst #Nephpearls
RVOT pulse-wave Doppler can provide useful clues about pulmonary vascular resistance.
In normal individuals (A), the waveform has a smooth, dome-shaped appearance, with peak velocity occurring in mid-systole, reflecting a compliant, low-resistance pulmonary circulation.
As RV afterload increases, the waveform gradually becomes more triangular. The RVOT acceleration time shortens, and the peak velocity shifts earlier into systole (B).
With further increases in pulmonary vascular impedance and reduced arterial compliance, a characteristic mid-systolic notch may appear (C), creating the classic "W sign."
In advanced pulmonary hypertension with RV failure, the Doppler envelope becomes smaller and more abbreviated, with a very short and steep AccT (D). This reflects rapid equilibration of RVOT and proximal pulmonary artery pressures due to severe afterload elevation.
Like most POCUS findings, RVOT Doppler should be interpreted in the context of the overall echocardiographic picture rather than in isolation.

May 31

#POCUS #Nephpearls #FOAMed
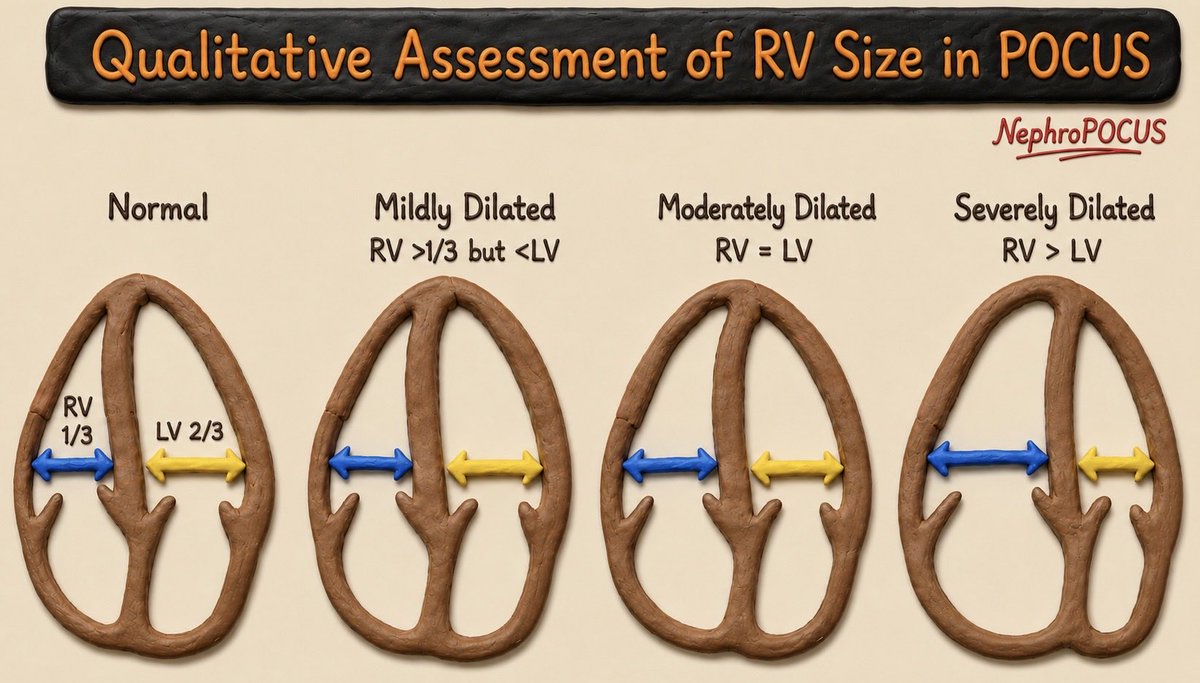
The RV should normally appear smaller than the LV in the apical 4-chamber view and should not exceed about two-thirds of the LV size. If the RV appears equal to or larger than the LV, significant RV dilation should be suspected.
Another helpful visual clue is when the RV becomes the apex-forming ventricle instead of LV. While this finding has not been formally validated with quantitative thresholds, it generally suggests at least moderate RV dilation.
If you remember just one measurement, remember this: the upper limit of normal RV basal diameter is 4.2 cm, measured at end-diastole in an RV-focused apical 4-chamber view.
Also assess RV wall thickness. An RV end-diastolic free wall thickness >5 mm (typically measured in the subcostal view) indicates RV hypertrophy, which often accompanies chronic pressure overload and RV dilation.
Finally, don’t forget to look for interventricular septal flattening on the parasternal short-axis view. Septal flattening (“D-shaped” LV) is another important clue to RV pressure and/or volume overload.
1
39
113
12,919
FLUTTER retweeted

May 20
#CardioNuggets™
The Pickelhaube sign is a sharp, spiked high-velocity systolic tissue Doppler signal of the lateral mitral annulus seen in arrhythmic mitral valve prolapse.
It’s named after the old German “Pickelhaube” helmet because the Doppler waveform resembles the helmet’s pointed spike.
Why it happens:
Prolapsing mitral leaflets cause abrupt systolic tugging of the papillary muscles/mitral annulus → creating a tall systolic velocity spike on TDI.
Why it matters:
Suggests arrhythmic MVP
Associated with ventricular arrhythmias/SCD risk
Often seen with bileaflet MVP and mitral annular disjunction (MAD)
Image from @drahmedmohsen85
#CardioNuggets #MedEd #EchoFirst


2
30
133
7,076

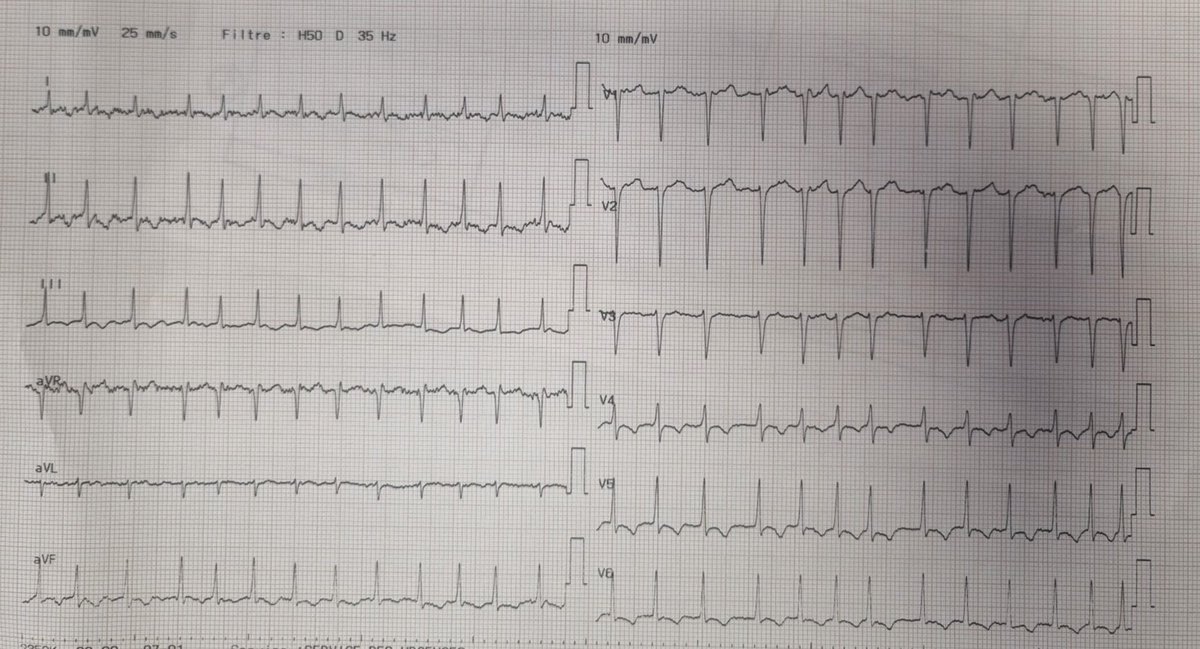
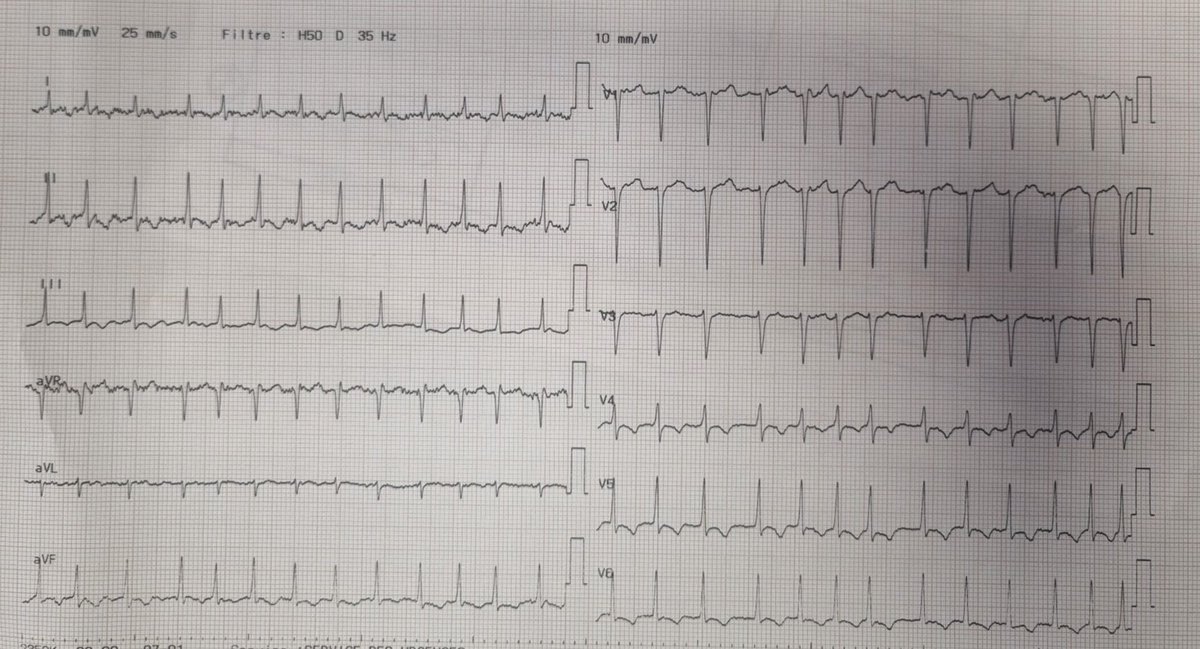
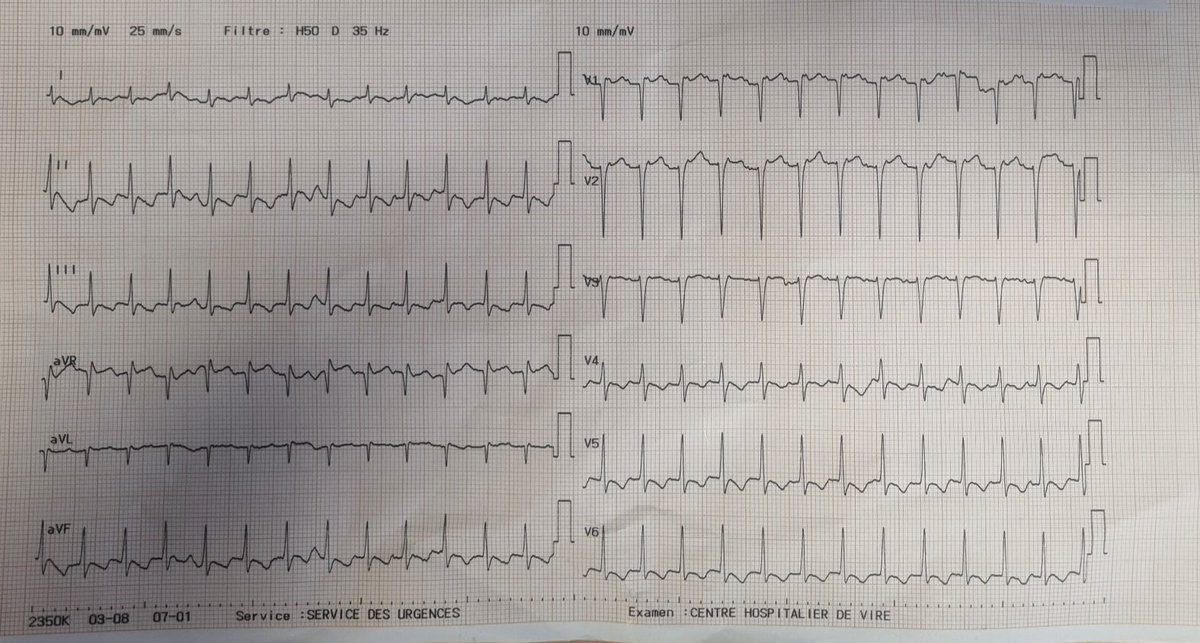
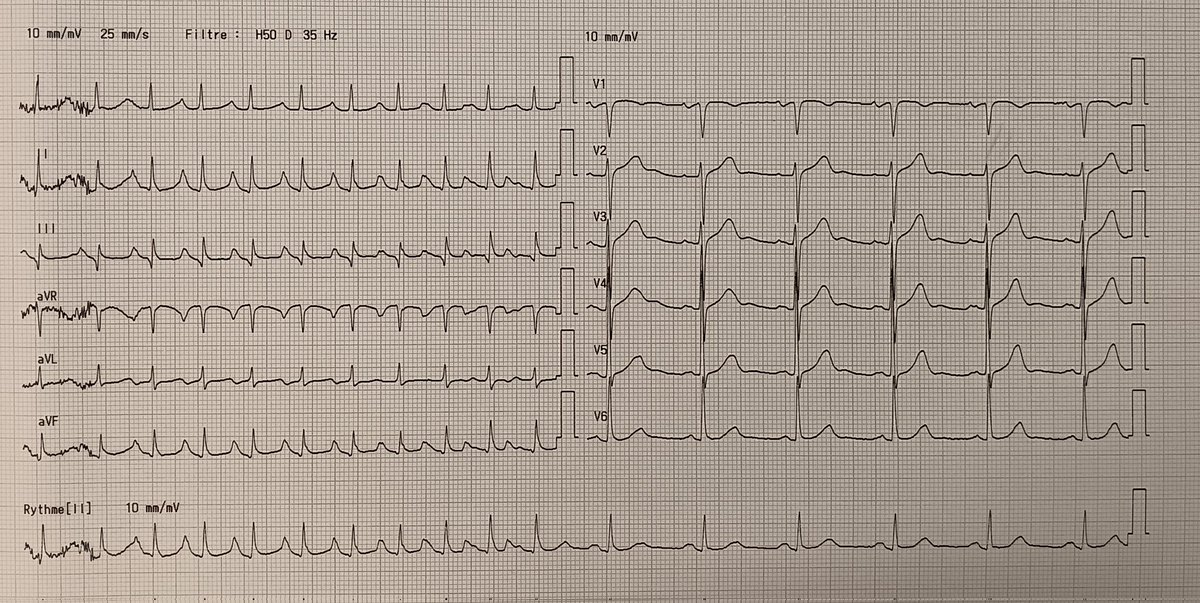
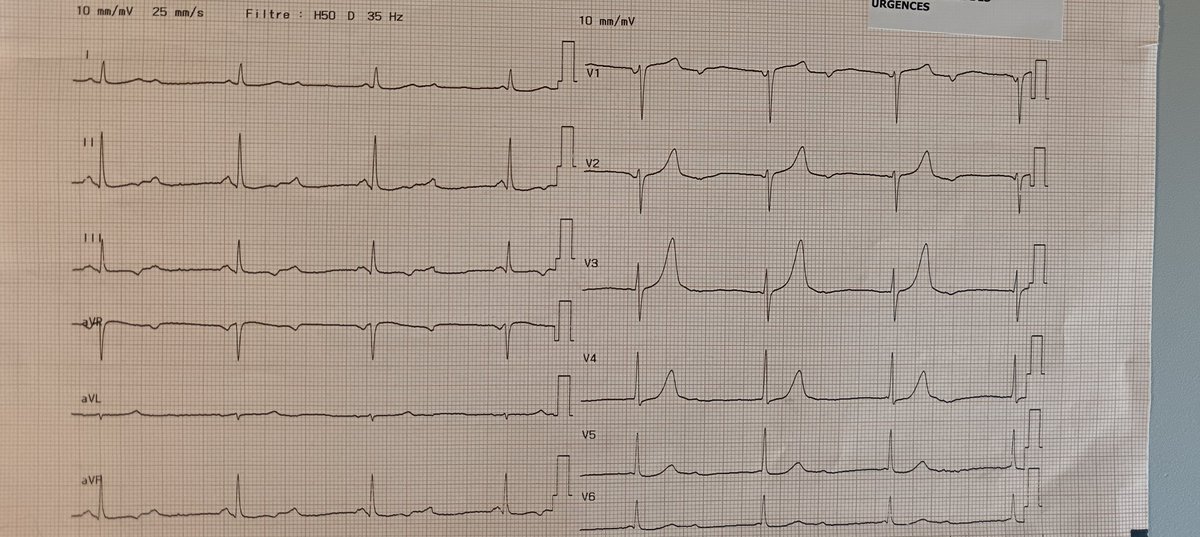
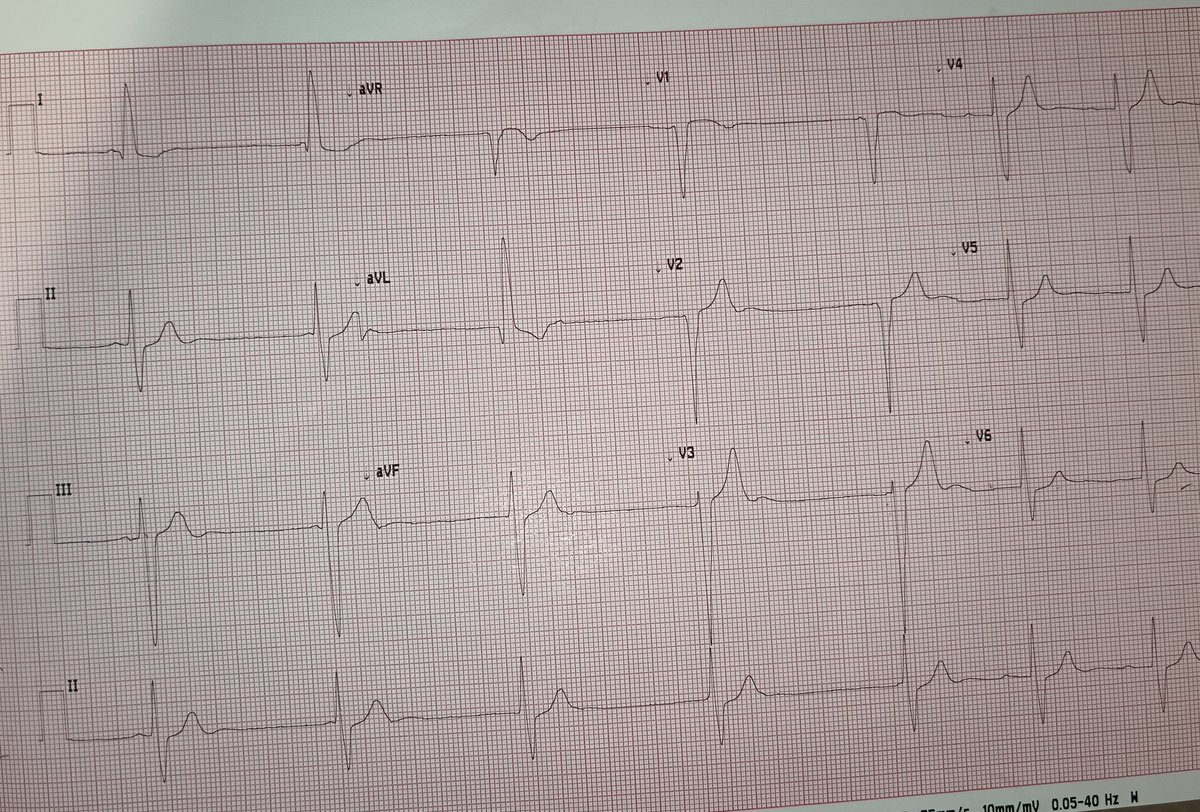
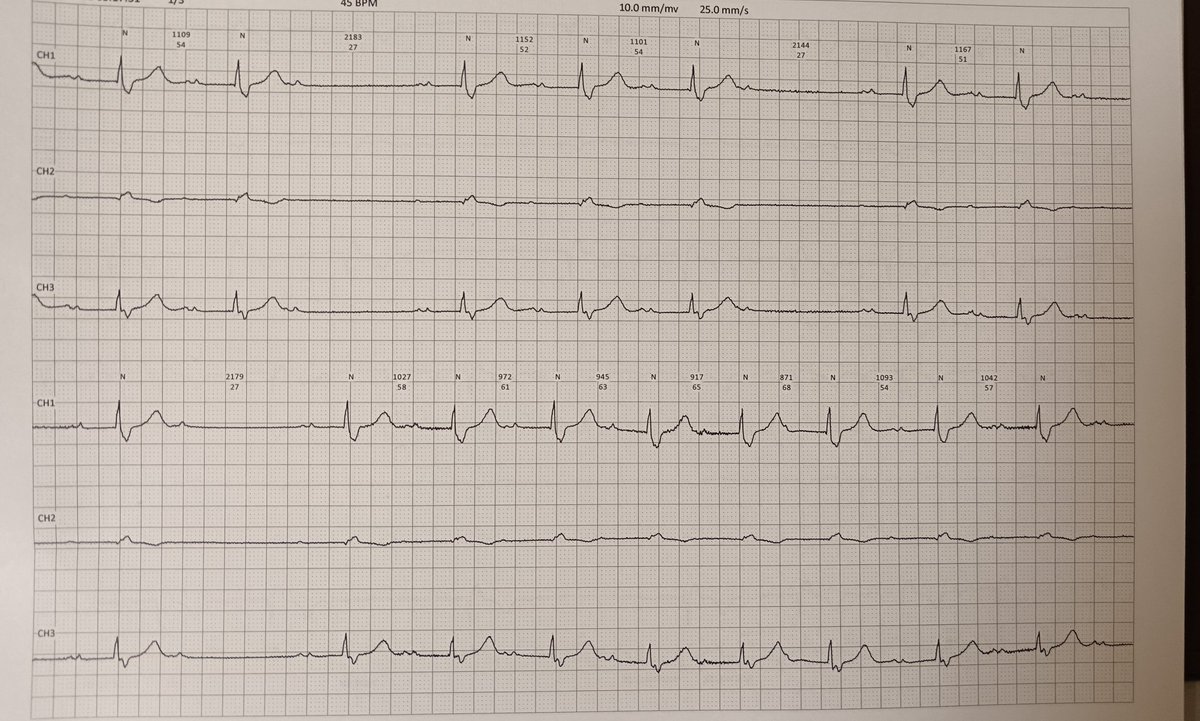
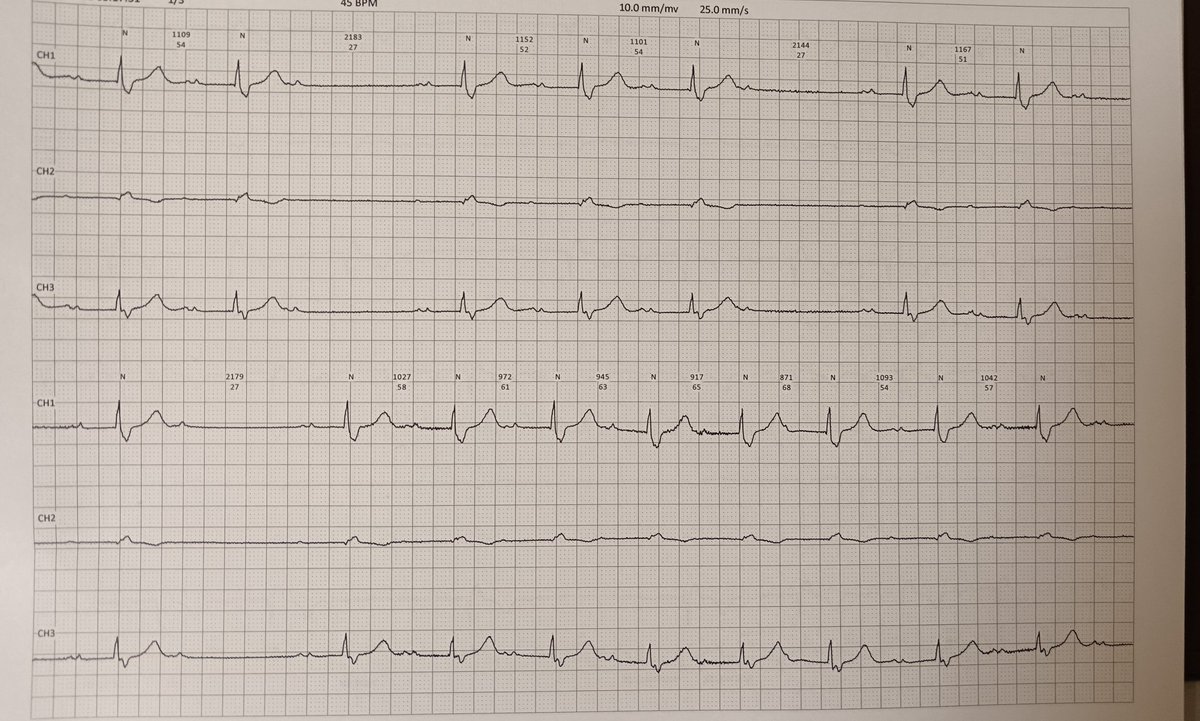
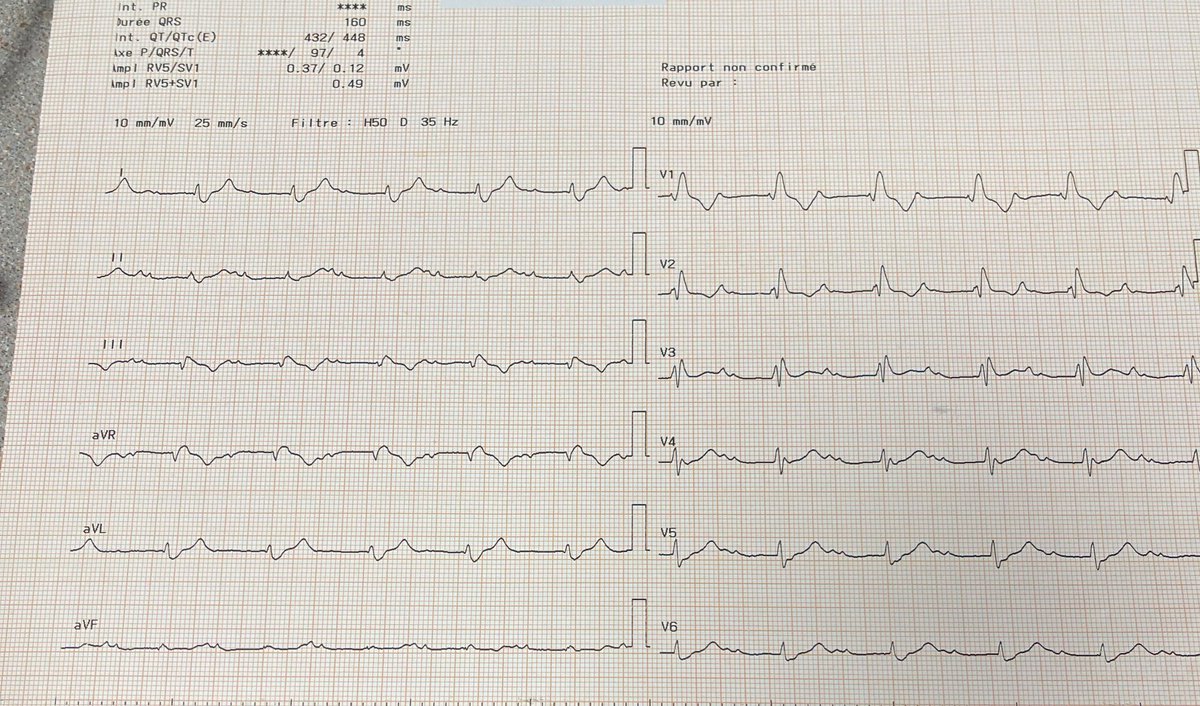
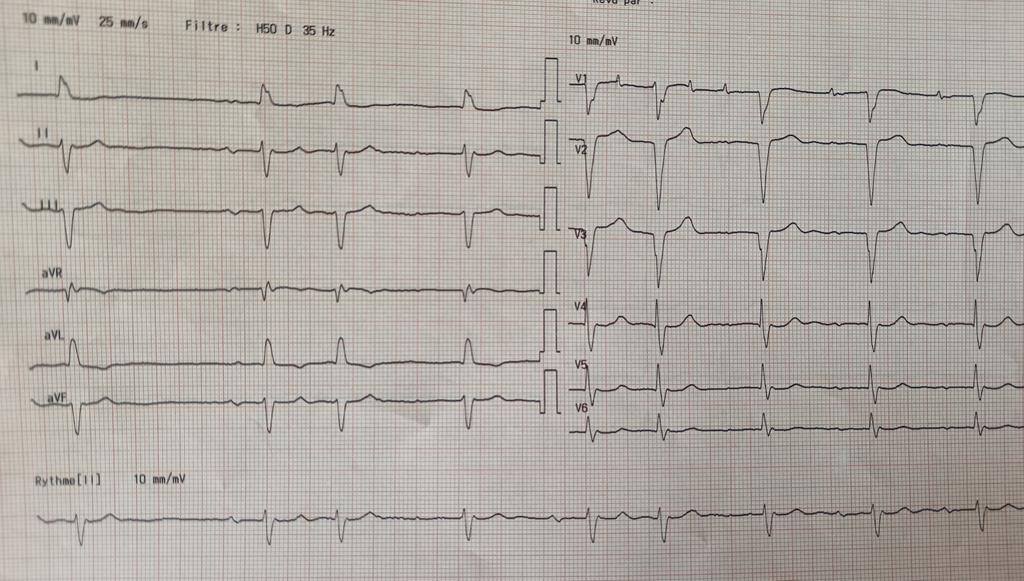
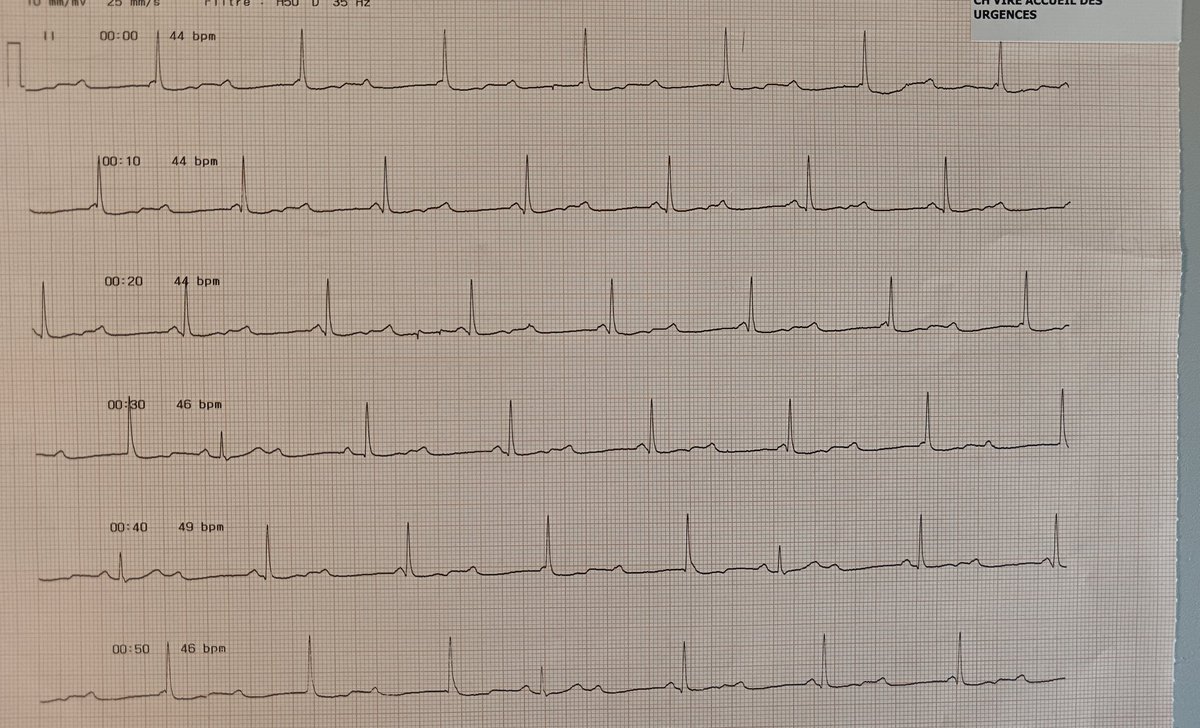
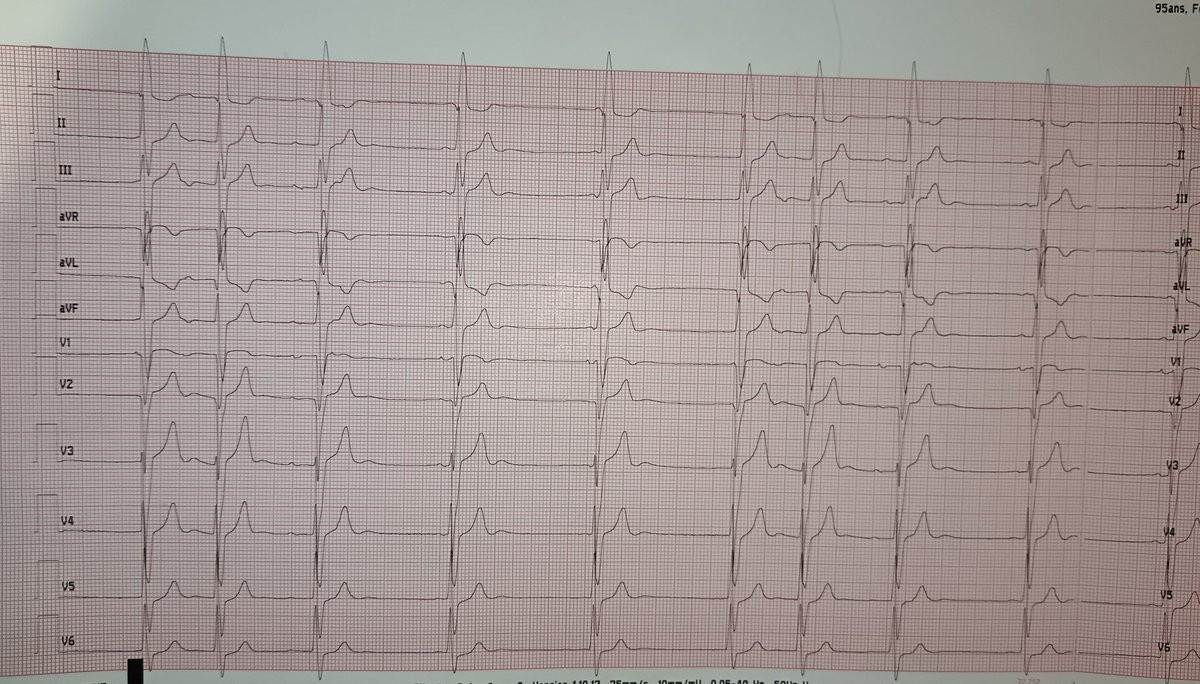
May 18
Same patient, a few minutes apart
@Ecgloverr @BerkBmf @akuseierikachan @FrdBjk112 @lila_enis @MertAvsever @marioalrb84_a @nihar_nayak2 @Nikhil_Kr16 @ThaierT13525 @MiguelP23970914 @sohrab1104 @ghwamasoob @Drakhil_cardio @Amhar_47 @AMigelheva @josecruz2102 @YilmazEile63275
1
2
310
FLUTTER retweeted

May 14
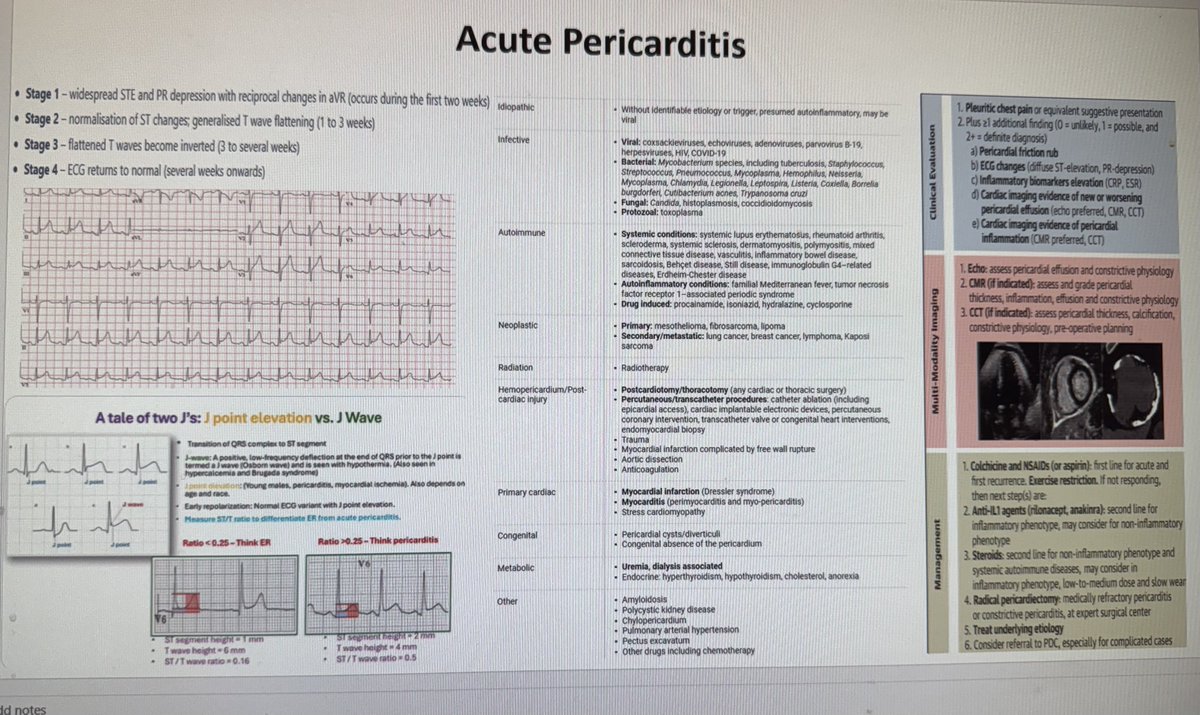
Everything you need to know about acute pericarditis
31
158
7,712
FLUTTER retweeted
🚨 HOT OFF THE PRESS! 🚨
New guidance from the American Society of Echocardiography @ASE360 for Cardiac Ultrasound Artifacts 🫀📡
➡️bit.ly/4tKDSvf
👉 A must-read for everyone in #EchoFirst!
🔍 What is an artifact?
➡️ An imaging feature that does NOT reflect true anatomy/pathology
➡️ Common, expected, and rooted in ultrasound physics ⚙️
💡 Why this matters
⚠️ Artifacts can mimic disease → misdiagnosis → inappropriate management
⚠️ Present across ALL modalities:
• 2D 🖥️
• Spectral Doppler 📈
• Color Doppler
• 3D echo 🧊
📘 What this guideline delivers
✅ Standardized, structured approach to artifacts
✅ Clear explanation of:
• Appearance 👁️
• Mechanism ⚙️
• Clinical impact 🏥
• Real-world cases 🧾
• Mitigation strategies 🛠️
🧠 Also covers
🔹 “Artifact-like” phenomena
🔹 Interference from external devices & equipment 📡
🎯 Key takeaway
👉 Artifacts are inevitable—but misinterpretation is not
👉 Mastering them = safer, smarter echo practice
👩⚕️👨⚕️ Who should read this?
➡️ Sonographers
➡️ Cardiologists
➡️ Trainees
➡️ Anyone interpreting cardiac ultrasound
📢 Elevate your imaging game. Recognize. Understand. Mitigate.
#CardioX #Cardiotwitter @JournalASEcho #ACCFIT
48
135
10,117
FLUTTER retweeted
Apr 21
Dagger-shaped LVOT Doppler - classic in HOCM, but increasingly relevant in #CriticalCare #Nephrology #POCUS
• What you see
Late-peaking, “dagger” CW Doppler profile
Slow rise → abrupt mid–late systolic peak
• Why it matters
Distinguishes dynamic LVOT obstruction from fixed AS (which peaks early)
• Mechanism
Systolic anterior motion (SAM) of mitral valve
→ leaflet pulled into LVOT during ejection
→ obstruction worsens as systole progresses
• Hemodynamics
Gradient = 4 × V²
≥30 mmHg → significant obstruction
Not just HCM — big ICU problem
Dynamic LVOTO can occur without structural HCM
Seen in septic shock, stress cardiomyopathy, hypovolemia
🚨 Can present as refractory hypotension
…and paradoxically worsens with inotropic vasoactive agents.
Triggers
• Hypovolemia
• Inotropes (dobutamine 👎)
• Low afterload (sepsis)
• Tachycardia, hypercontractility
• High sympathetic tone
Substrate
• LVH (common in #ESRD)
• Small LV cavity
• Sigmoid septum
• Elderly, often female
#POCUS clues (don’t miss this)
• Hyperdynamic, small LV
• SAM of mitral valve (use M-mode in PLAX)
• LVOT flow acceleration
• Dagger-shaped CW Doppler (key finding)
Management flips the script (“LVOTO bundle”)
❌ Stop harm
• Inotropes
• Diuretics
✅ Do the opposite
• Fluids → increase preload
• Afterload → switch norepinephrine to phenylephrine/vasopressin
• Beta-blockade → reduce contractility
• ↓ PEEP if too high
Bottom line
Not all hypotension needs more inotropy.
If you see a dagger, think LVOTO and reverse your reflexes.
13
42
2,359