
@JohnsHopkinsDOM Hospitalist/Proceduralist; #IMPOCUS #EdTech #Simulation #LearningAnalytics #AI CCEeXAM testamur
Joined May 2015
- Tweets 5,298
- Following 1,642
- Followers 1,676
- Likes 9,183
365 Photos and videos





Gigi Liu retweeted

Jun 12
Review
Categories of Aortic Stenosis: What’s New and the
Clinical Implications doi.org/10.3390/medicina6205… #echofirst #cardiology

13
33
1,918
Gigi Liu retweeted
Jun 12
Review
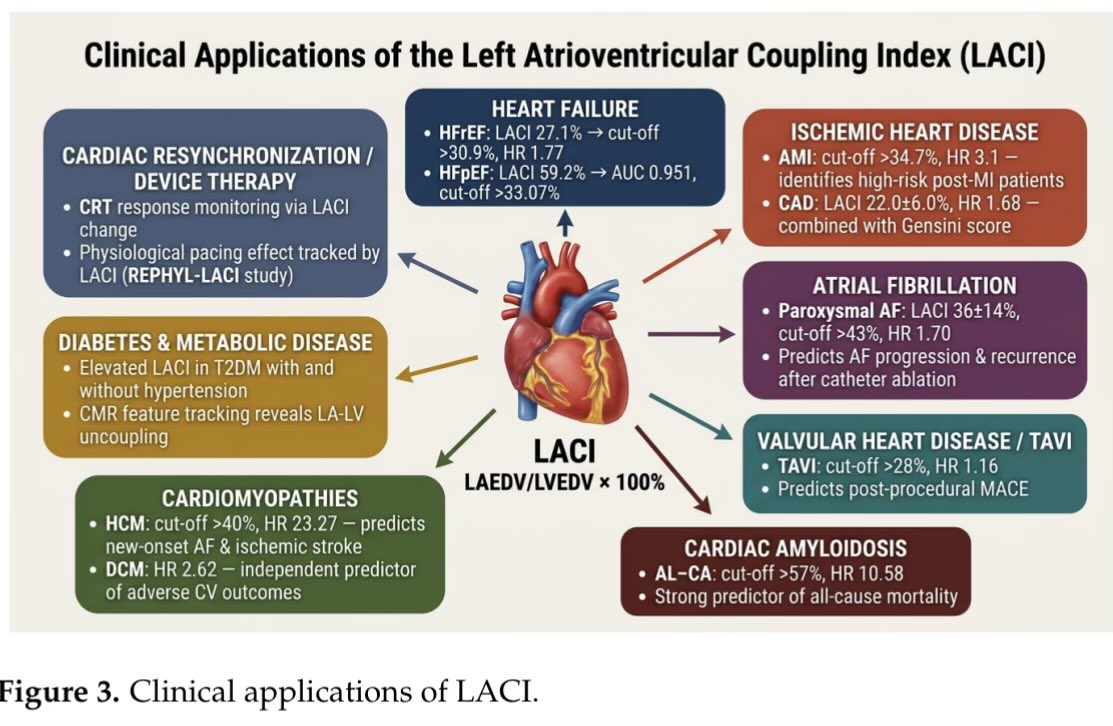
Left Atrioventricular Coupling Index: A Comprehensive Review
of the Literature doi.org/10.3390/life16050722 #echo #echofirst #cardiology
1
19
38
2,281
Gigi Liu retweeted

Jun 13
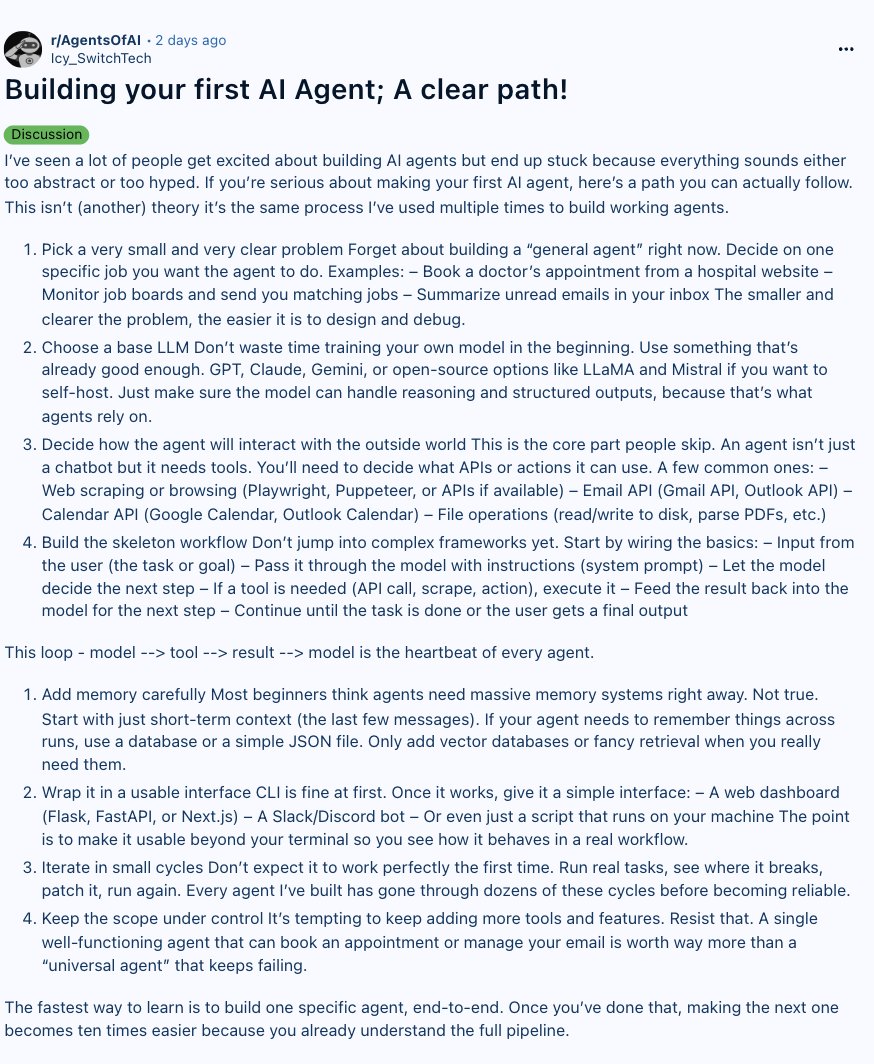
How to build your first AI agent (Full guide)

21
724
4,320
553,533
Gigi Liu retweeted

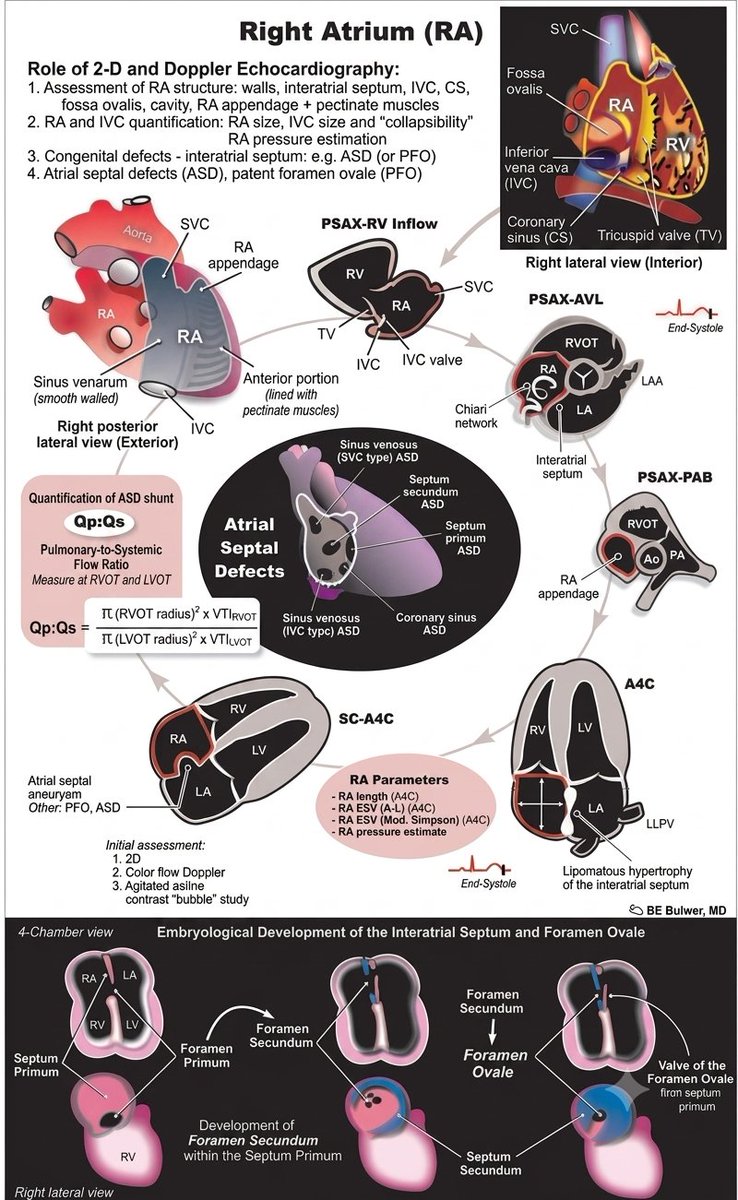
Echocardiographic assessment of the right atrium.
Image courtesy of: BE bulwer, MD
1
31
95
3,207
Gigi Liu retweeted

🫀 Septic Shock Is Not Just About Blood Pressure: It Is About Ventriculo-Arterial Coupling
For years, septic shock resuscitation has focused on restoring MAP, increasing cardiac output, and normalizing lactate.
But what if the real problem is not flow alone?
What if the heart and arterial system are no longer working together?
This is the concept of ventriculo-arterial coupling (VAC): the dynamic interaction between ventricular contractility (Ees) and arterial load (Ea). When coupling is preserved, the cardiovascular system operates efficiently, maximizing stroke work while minimizing myocardial energy expenditure.
Why VAC Matters in Septic Shock
Sepsis causes profound vasoplegia, myocardial depression, and alterations in vascular tone.
As a result, many patients develop ventriculo-arterial uncoupling, where ventricular contractility and arterial load become mismatched. This leads to:
✅ Reduced cardiovascular efficiency
✅ Increased myocardial energetic cost
✅ Impaired tissue perfusion despite apparently adequate cardiac output
✅ Variable responses to fluids, vasopressors, and inotropes
In other words:
Two patients may have the same MAP and cardiac output but completely different cardiovascular efficiency and energetic burden.
The Norepinephrine Paradox
One of the most interesting concepts highlighted by Pinsky and Guarracino is that increasing blood pressure does not always improve cardiovascular performance.
In some septic shock patients with depressed contractility:
🔹 Norepinephrine increases arterial elastance (Ea)
🔹 MAP rises
🔹 Left ventricular afterload increases
🔹 Stroke volume may fall
🔹 VAC worsens
🔹 Cardiac output may remain unchanged or even decrease
The monitor shows a better blood pressure.
The ventricle may actually be working less efficiently.
Why Some Patients Respond and Others Do Not
The review provides a physiological explanation for the heterogeneity we see every day in the ICU.
Patients with preserved contractile reserve may tolerate increased afterload and maintain efficient coupling.
Patients with septic cardiomyopathy may not.
This may explain why identical norepinephrine doses can produce dramatically different hemodynamic responses among seemingly similar septic shock patients.
Beyond Left Ventricular Function
The same principles apply to the right ventricle.
In septic patients with ARDS:
🔹 Pulmonary vascular resistance rises
🔹 RV afterload increases
🔹 RV-pulmonary artery coupling deteriorates
🔹 Venous congestion develops
🔹 Organ perfusion worsens despite acceptable systemic pressures
This reminds us that shock physiology extends far beyond MAP alone.
Clinical Takeaway
Perhaps the next evolution of septic shock management is not simply asking: "Did cardiovascular efficiency improve?"
Reference 📚
Pinsky MR, Guarracino F. Pathophysiological implications of ventriculoarterial coupling in septic shock. Intensive Care Medicine Experimental. 2023;11:87.
doi.org/10.1186/s40635-023-0…

ALT
72
193
6,650
Gigi Liu retweeted

Jun 13
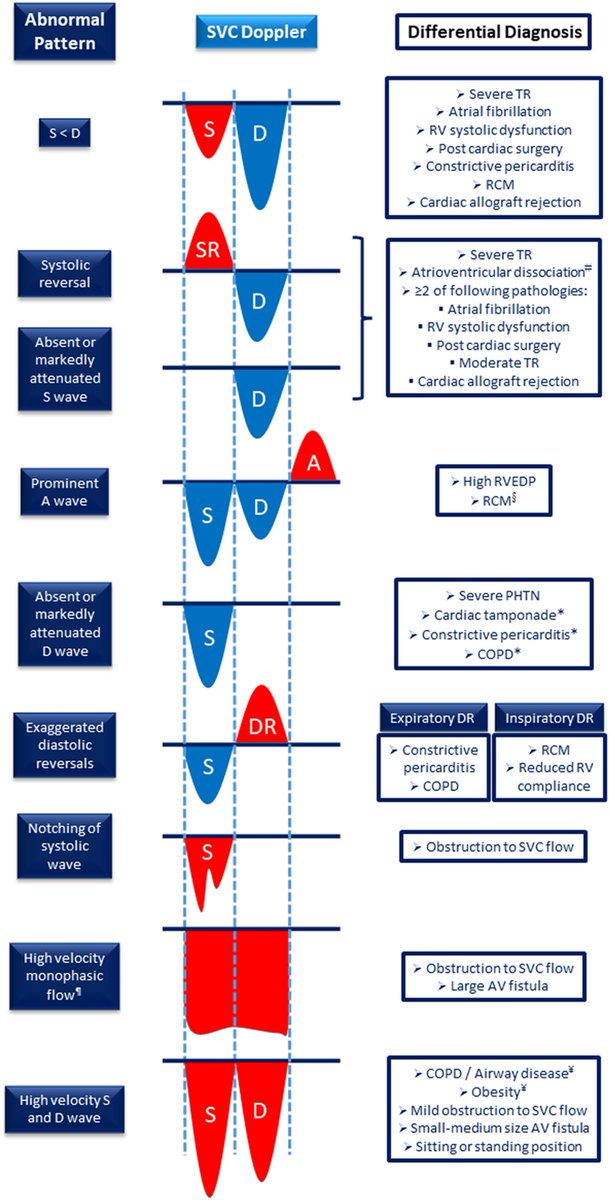
How to do SVC #POCUS 📹 an illustration of abnormal SVC Doppler patterns.
#VExUS #eVExUS #Nephpearls
From 🔗J Am Soc Echocardiogr. 2023;36(5):447-463. doi: 10.1016/j.echo.2023.01.017
3
64
182
9,067
Gigi Liu retweeted

Jun 11
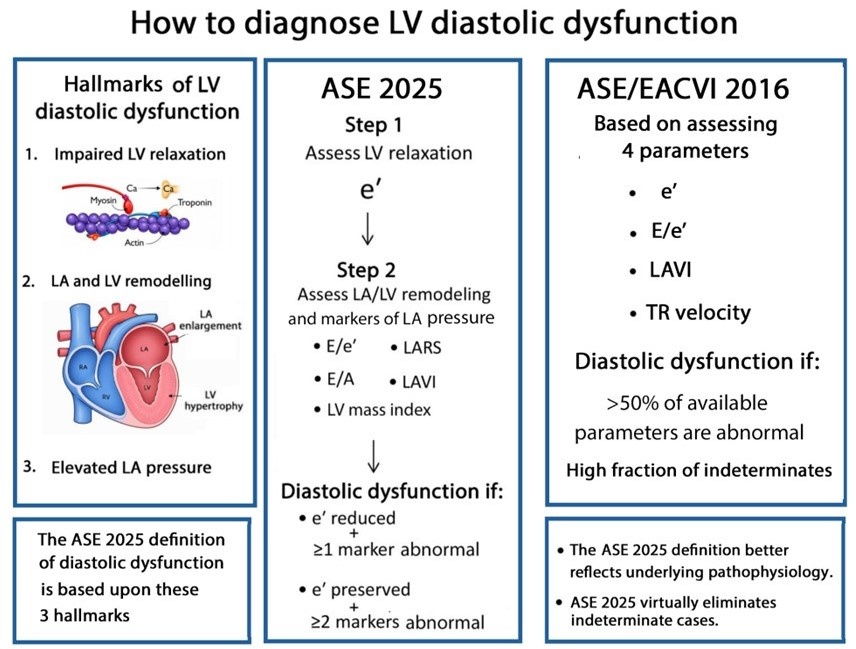
Most echocardiography laboratories have adopted the 2016 diastolic guidelines. With the release of the 2025 update, an important question arises:
What are the key conceptual differences between the 2016 and 2025 approaches to diagnosing diastolic dysfunction?
academic.oup.com/ehjcimaging…
@JGrapsa
12
82
252
16,831
Gigi Liu retweeted

Some enhancements in the SMV Simulator
Live Monitor with run and pause
Patient-Ventilator Interactions and Dyysynchronies
societymechanicalventilation…
1
3
452
Gigi Liu retweeted

Jun 10
What can you tell by looking at this inspiratory hold?

1
8
43
7,569
Gigi Liu retweeted
Jun 10
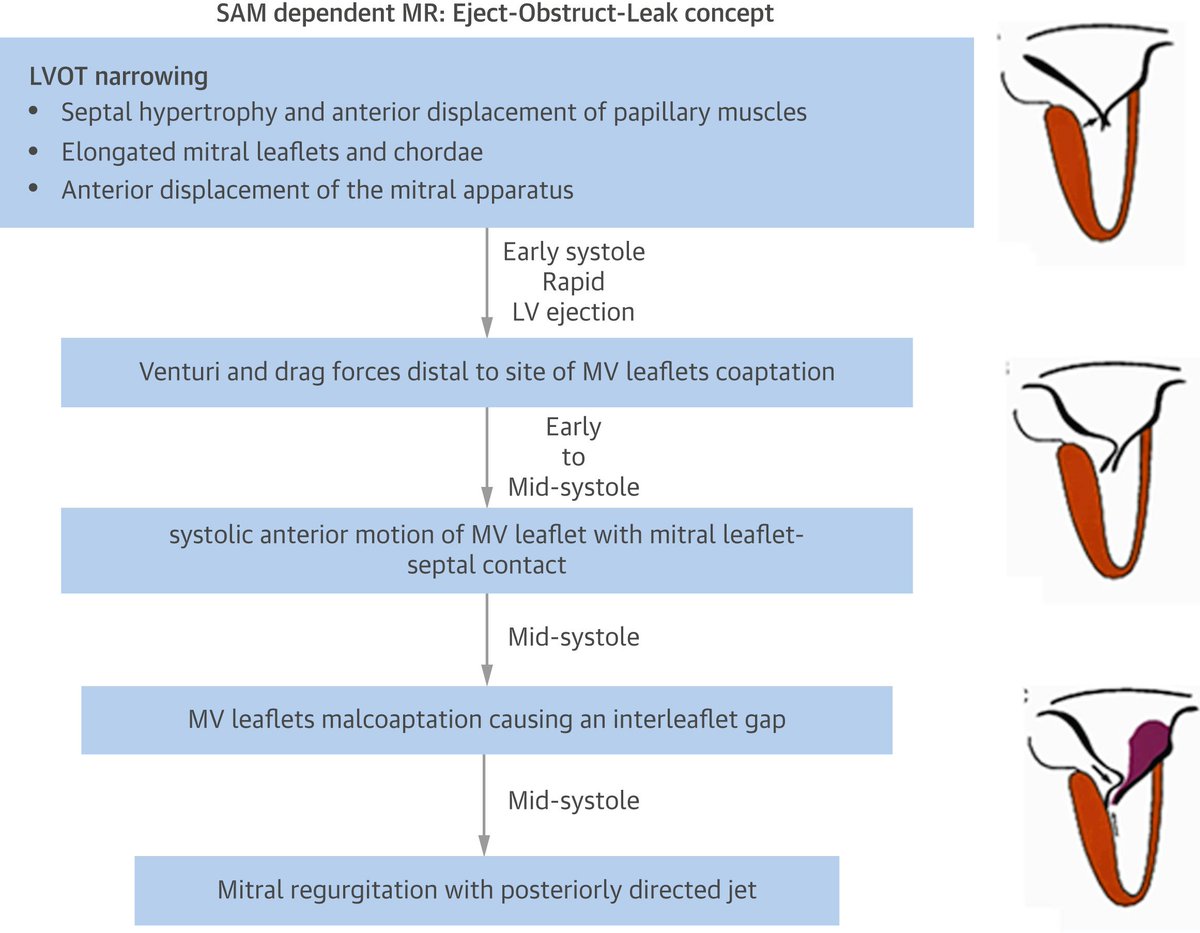
Mechanism of Dynamic LV Outflow Obstruction and Associated MR.
From - PMID: 27687191
#POCUS #FOAMed #Nephpearls
16
63
3,332
Gigi Liu retweeted
Jun 10
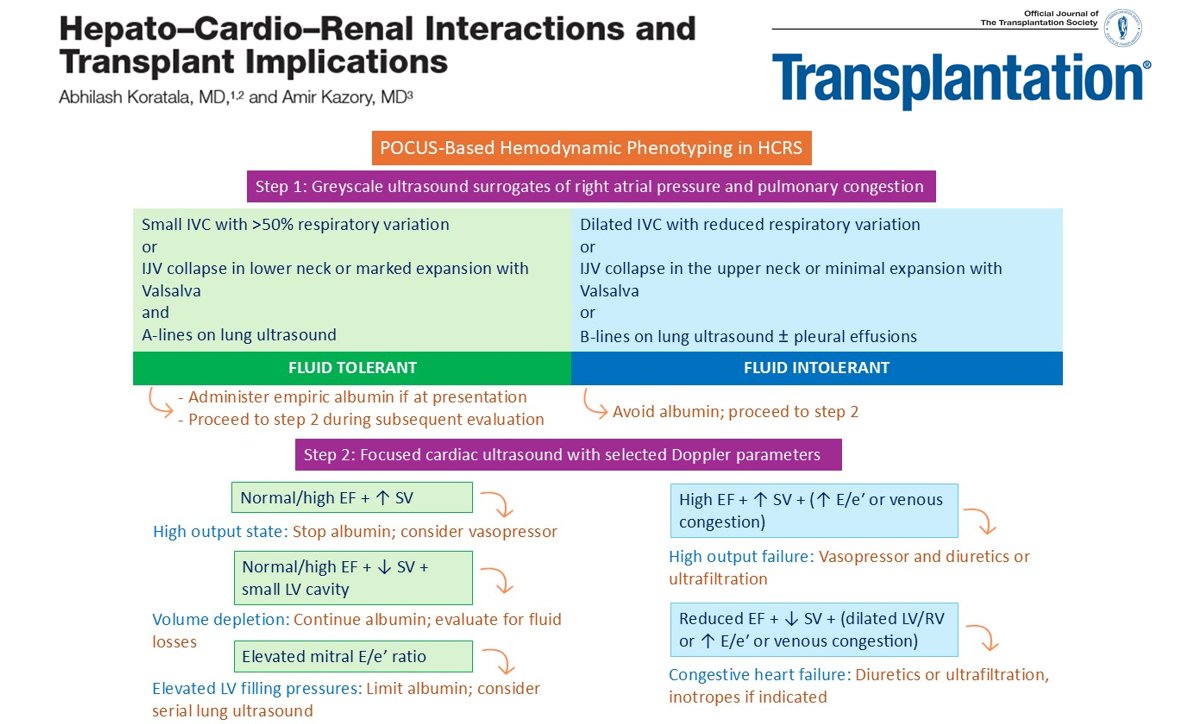
Excited to share our latest review in @TransplantJrnl on hepato-cardio-renal interactions, #POCUS and #transplant implications. Honored to collaborate with Prof. @AmirKazory, a pioneer in this field who coined the term hepato-cardio-renal syndrome.
#hepatorenal 🤝#cardiorenal
Glad to see a major transplant journal taking interest in multi-organ POCUS and bedside hemodynamic phenotyping.
Much more research is needed in this area, but meaningful progress will require equally strong efforts in education and training.
🔗journals.lww.com/transplantj…
2
17
36
2,834
Gigi Liu retweeted
A gift from us to you
Try this Ventilator Simulator, calculate total System and Trans-Pulmonary work/energy, its components
societymechanicalventilation…


8
14
1,311
Gigi Liu retweeted
Jun 9
Pleased to have had the opportunity to write this CJASN editorial @asnpublications on the USE-the-FORCE-for-Acute Kidney Injury trial by our Canadian colleagues.
🔗journals.lww.com/cjasn/citat…
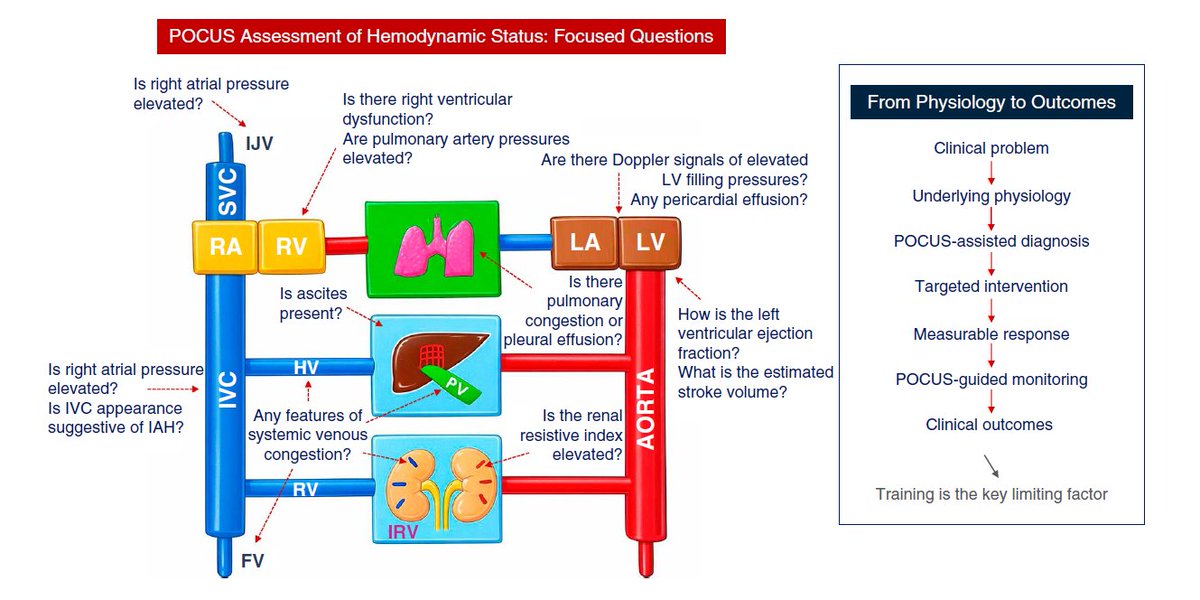
I'm especially glad to see mainstream #nephrology journals taking interest in multi-organ #POCUS. Even better, I managed to sneak my proprietary hemodynamic circuit illustration into the article!!
1
32
80
9,349
Gigi Liu retweeted

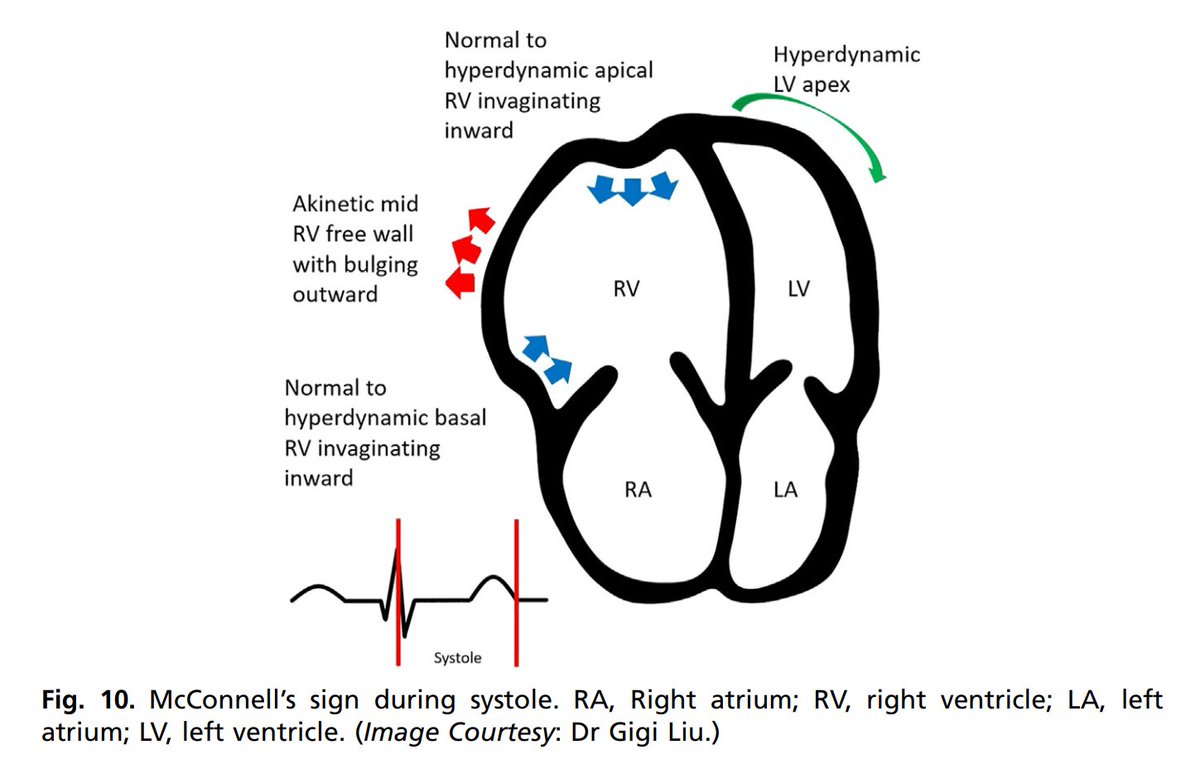
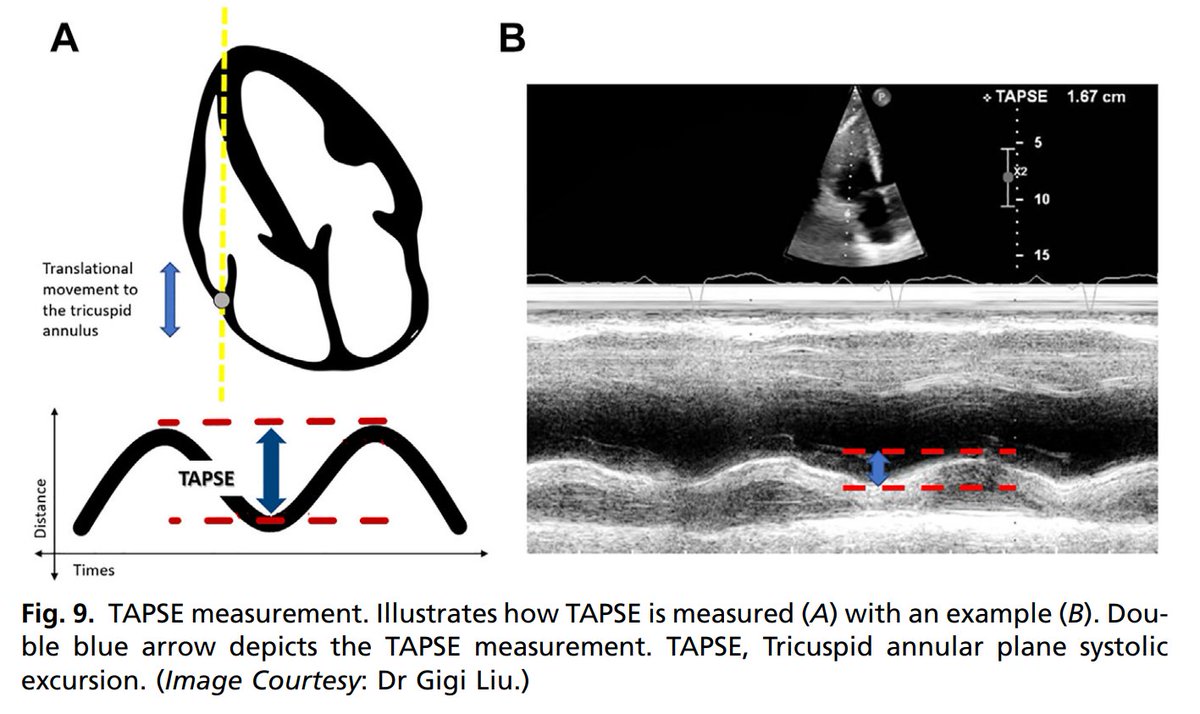
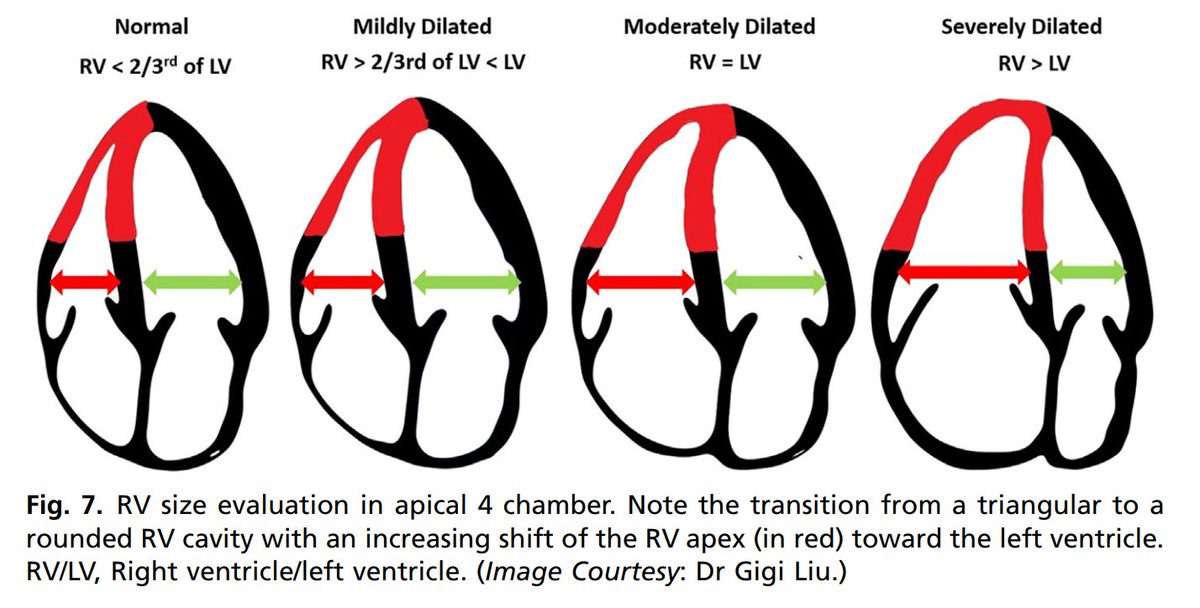
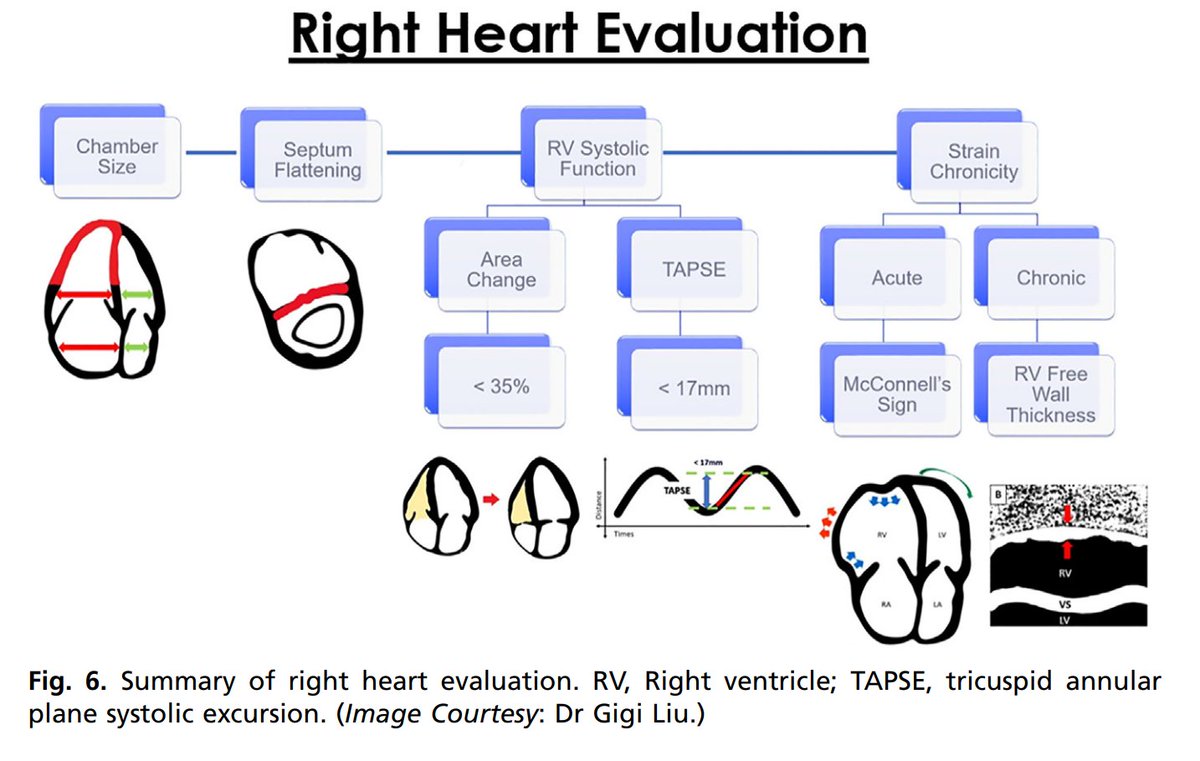
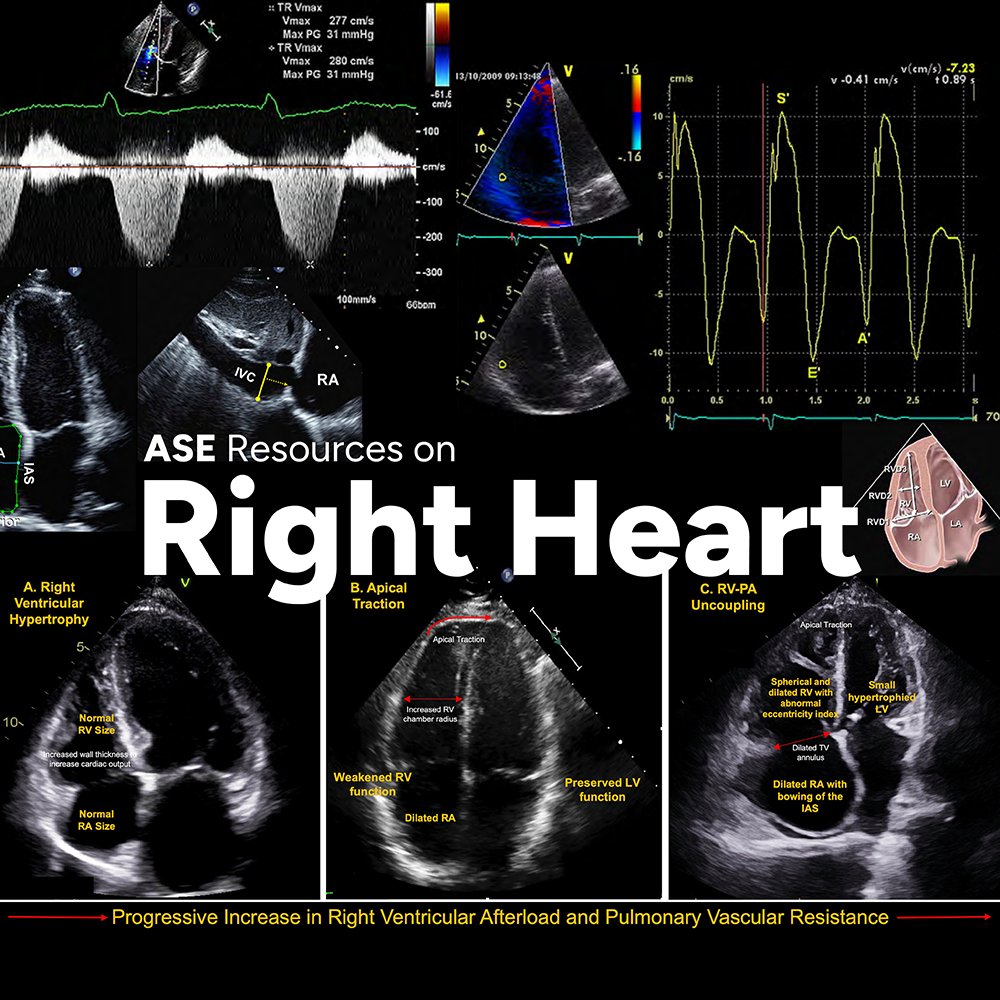
ASE and @accpchest recently partnered on a project to develop two educational webinars to improve the understanding of cardiovascular ultrasound's application in pulmonary hypertension (PH). @chest
You can find them on our Right Heart Resources web page! bit.ly/4nQ5E7p
54
149
6,231
Gigi Liu retweeted
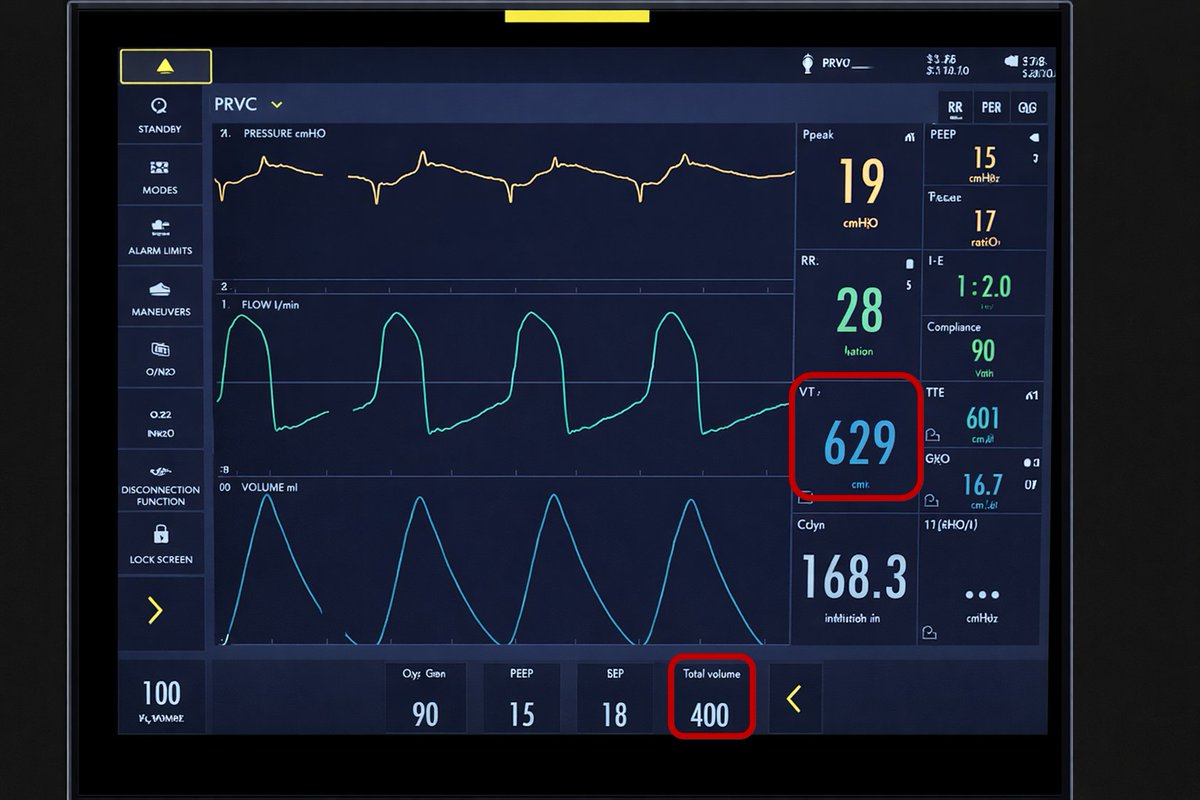
You set the ventilator to deliver a Vt of 6ml/kg of PBW on PRVC to a patient with severe ARDS.
Is the patient receiving lung protective ventilation?
8
16
57
13,052
Gigi Liu retweeted

Jun 4
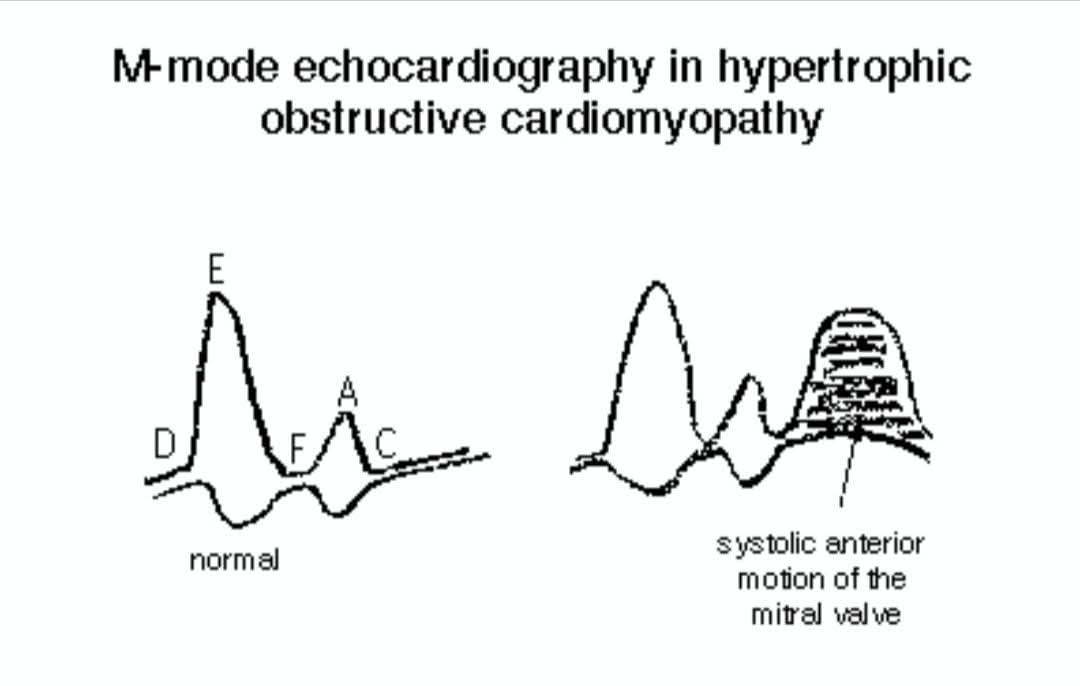
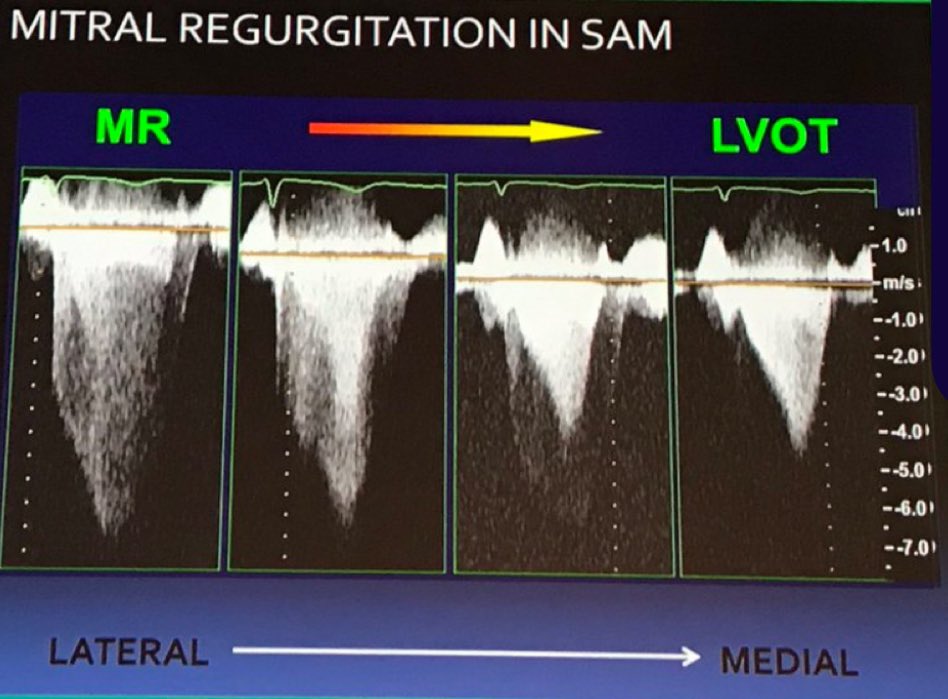
🫀 Systolic Anterior Motion (SAM) of the Anterior Mitral Leaflet(AML)
Have you ever seen a mitral valve leaflet moving toward the septum during systole? This classic echocardiographic finding is called Systolic Anterior Motion (SAM) and is a hallmark of (HOCM)
Thread 👇
1
15
61
2,724
Gigi Liu retweeted

13 Nov 2024
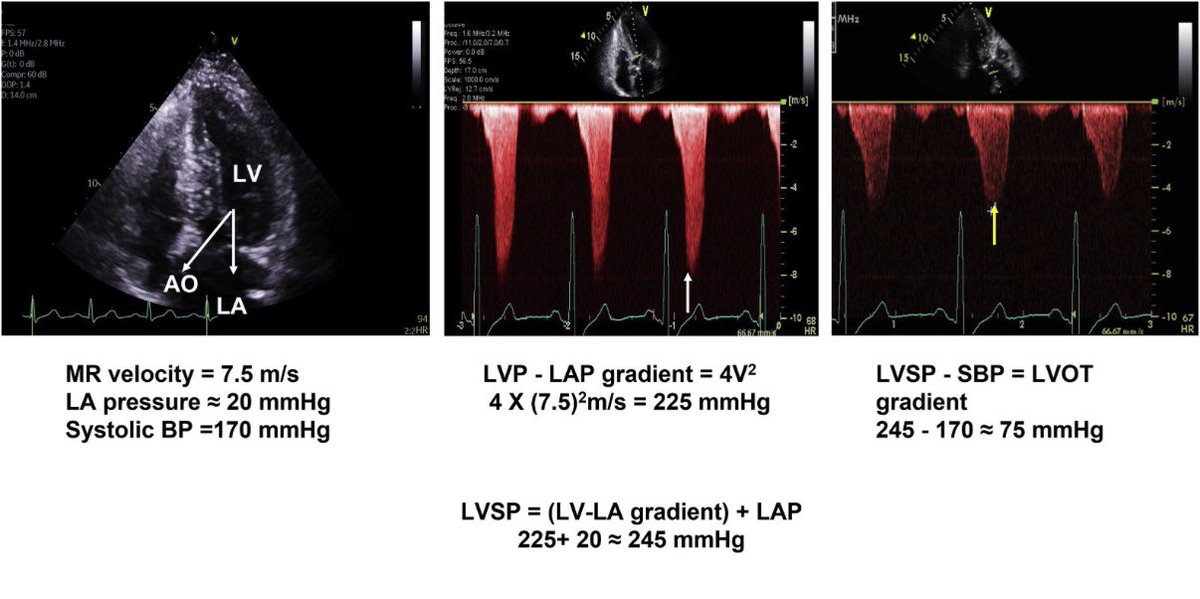
confusing LVOT Doppler signal w mitral regurgitation due to SAM in hypertrophic CM?
double check if it’s really the LVOT signal by estimating LVOT gradient with SBP/peak MR jet
& see if this matches measured LVOT (4v2) gradient
1.Peak MR signal(velocity) gives LVP-to–LAP gradient (4V2)
2.LVSP estimated by LV-LA gradient LAP (~10-20mm Hg)
3.LVOT gradient estimated by LVSP – systolic BP #echofirst @echo_batman
8
90
283
107,728
Gigi Liu retweeted
Jun 1

1
27
129
5,120
Gigi Liu retweeted

Central Venous Pressure Revisited: Physiology, Pitfalls, Misconceptions, and Modern Clinical Interpretation in Critical Care
CCR Journal Watch
criticalcarereviews.com/late…

72
213
10,298
Gigi Liu retweeted
May 29
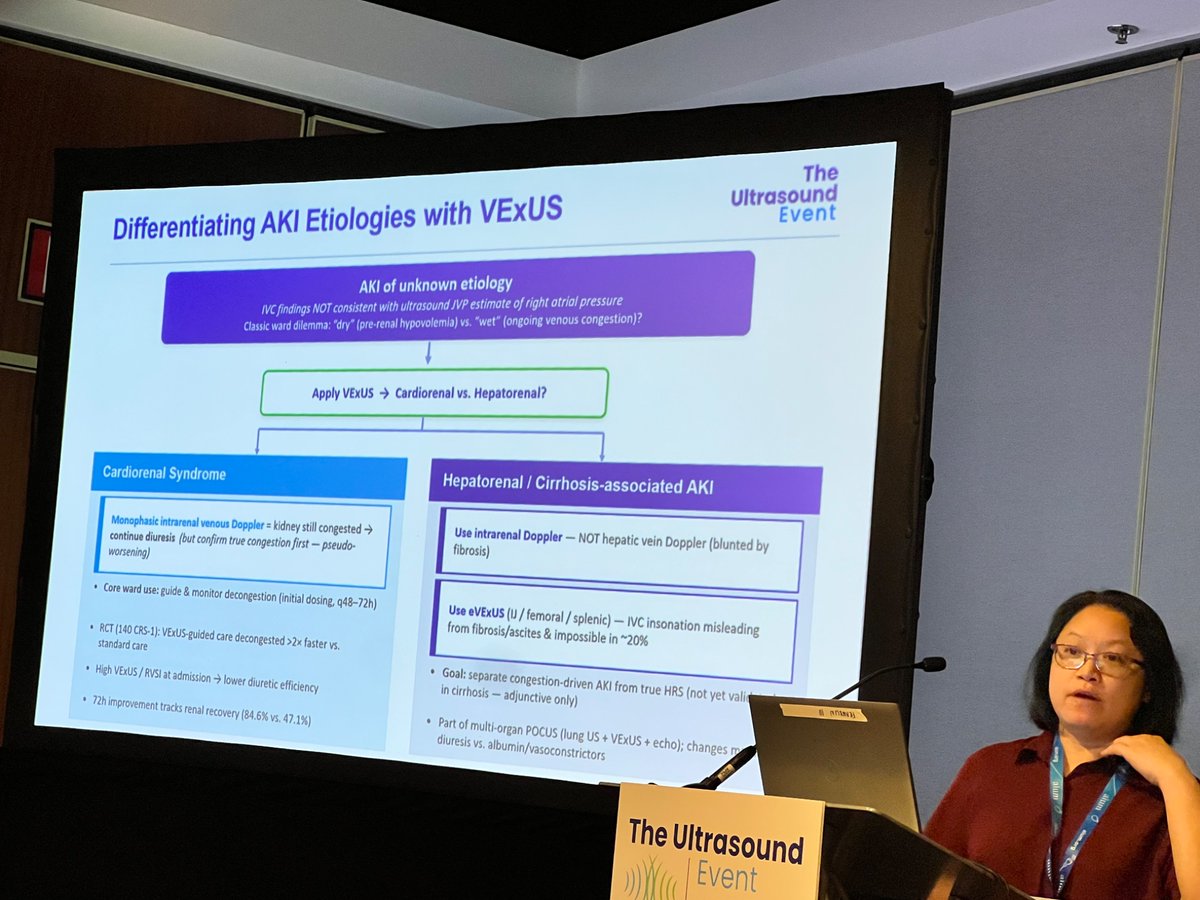
How can #VExUS help in #AKI?
Dr. @G2Disrupt offers a practical snapshot of its current clinical application at #AIUM2026 VExUS session.
16
61
4,315