
Latest #DigitalHealth, #HealthIT news. #HIMSS #HITsmIND | Newsletter hcitexpert.com/newsletter | Editor @msharmas | Support Us - bit.ly/2zXCu17
Joined July 2012
- Tweets 66,520
- Following 14,183
- Followers 15,582
- Likes 19,294
2,158 Photos and videos





Pinned Tweet

25 Aug 2021
Building A Purpose Driven #Digital #Oncology #Platform To Deliver World Class #Cancer #Care By Venkataramanan R , Founder CEO, @karkinoshealth
hcitexpert.com/2021/08/build…
#healthcare #digitalhealth #health #oncology #innovation #research #ceo #cancercare
1
7
22
The HealthCare IT Experts Blog retweeted

Jun 12
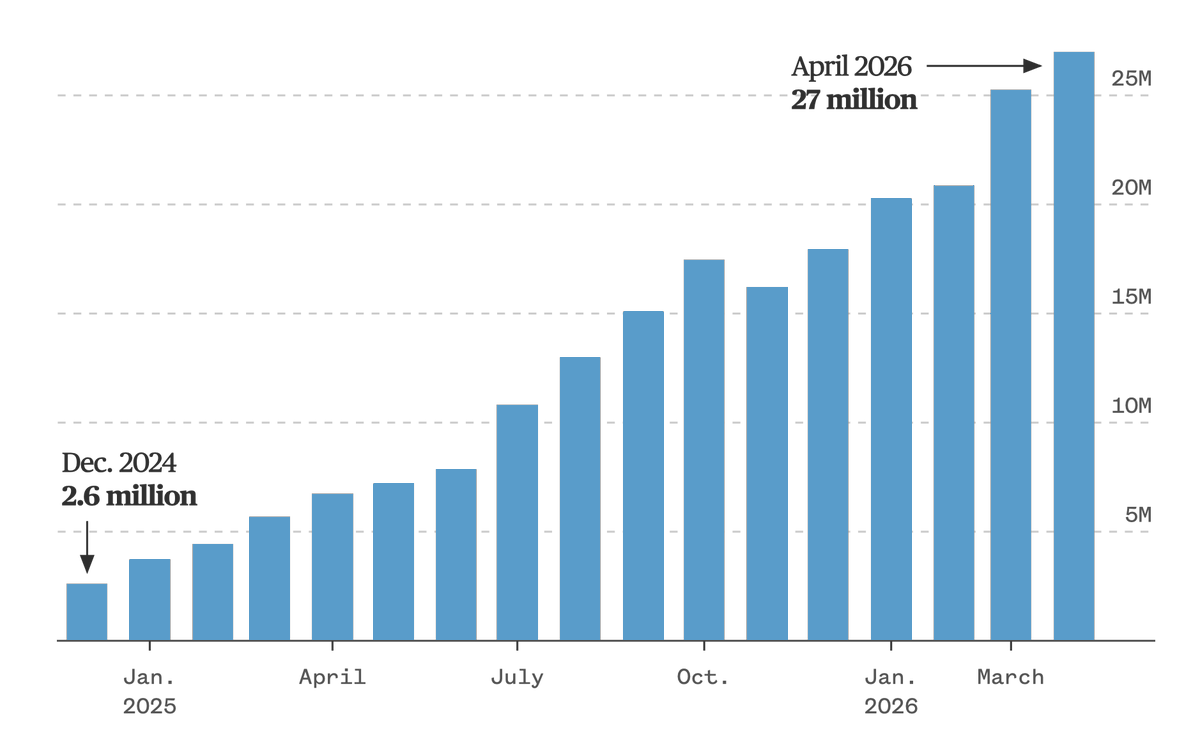
>65% of US physicians use OpenEvidence, with 27 million prompts in April
nbcnews.com/tech/tech-news/o…
5
14
127
44,459
The HealthCare IT Experts Blog retweeted
Jun 12
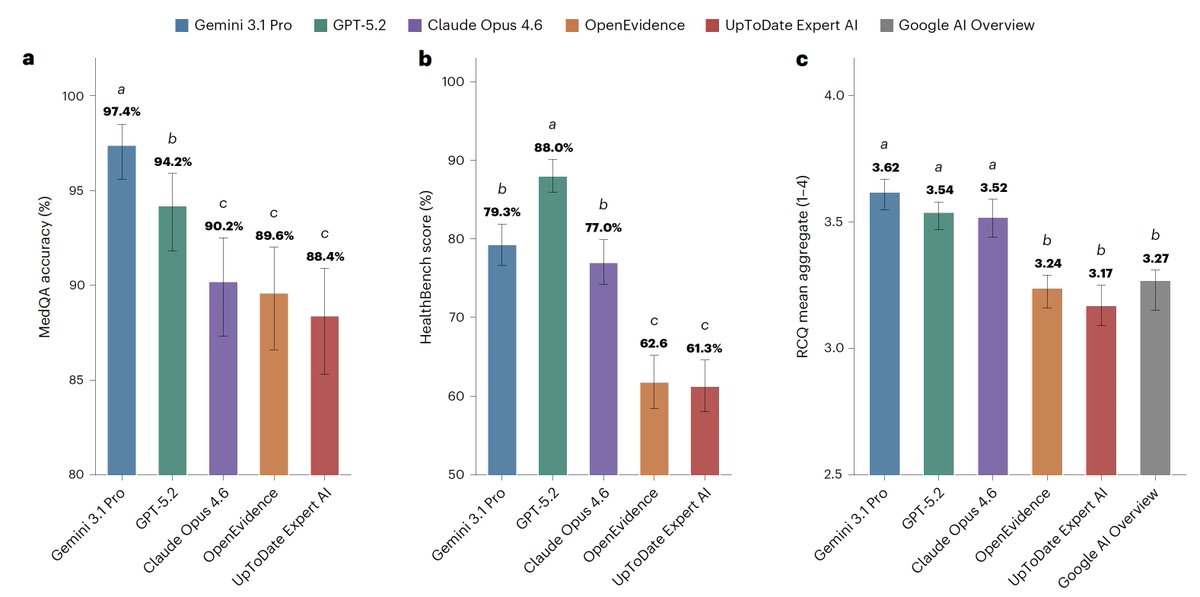
For medical information, general AI frontier models (Google, OpenAI, Anthropic) outperformed specialized @EvidenceOpen and @UpToDate as assessed by 12 US clinicians, randomized and blinded to which model and extensive testing/benchmarks. This was not anticipated. @NatureMedicine
nature.com/articles/s41591-0…
118
522
1,934
809,496
The HealthCare IT Experts Blog retweeted

Jun 12
Medicine discovers the bitter lesson: frontier LLMs (here GPT 5.2, Opus 4.6, Gemini 3.1) outperform specialized "clinical AI" (e.g. OpenEvidence) in a blind test.
Even funnier that hospital IT are more likely to approve the *specialized* versions despite them being worse.
Jun 12

For medical information, general AI frontier models (Google, OpenAI, Anthropic) outperformed specialized @EvidenceOpen and @UpToDate as assessed by 12 US clinicians, randomized and blinded to which model and extensive testing/benchmarks. This was not anticipated. @NatureMedicine
nature.com/articles/s41591-0…
30
166
1,153
184,064
The HealthCare IT Experts Blog retweeted

Jun 10
Today I'm publishing a new essay, Policy on the AI Exponential. AI is progressing extremely fast—much faster than the policy process was built to handle. The essay lays out where I think the technology is now, and the action needed to close the gap: darioamodei.com/post/policy-…
1,343
2,432
13,560
6,519,257
The HealthCare IT Experts Blog retweeted

Most people think NHCX is a database for health insurance claims.
It isn't. And that distinction matters more than you'd expect.
A quick thread on what NHCX actually does and why it's built the way it is. 🧵
#NHCX #CaladriusHealthAI
1
1
1
23
The HealthCare IT Experts Blog retweeted
Full article covers the ABDM stack, FHIR R4 standards, implications for hospitals, insurers, and TPAs, and what genuine NHCX readiness requires.
Article: linkedin.com/pulse/abdm-stac…
Video: youtu.be/sb7q1cihJ5Q?si=-dll…
#ABDM #NHCX
1
1
19
The HealthCare IT Experts Blog retweeted
The innovation pipeline is moving too.
In March 2026, the NHCX Hackathon at IIT Hyderabad drew over a hundred FHIR-aligned claims submissions.
The developer community isn't waiting for mandates. It's already building.
1
1
2
25
The HealthCare IT Experts Blog retweeted
And when something goes wrong, the system returns specific, standardized error codes rather than vague rejection notices.
That changes how billing teams respond. Less guesswork, more actionable next steps.
1
2
2
20
The HealthCare IT Experts Blog retweeted
One of the less discussed shifts: claims status visibility.
Rather than waiting for a final response with no updates in between, providers can look up transaction status at any point through a self-service function built into the protocol.
1
2
2
15
The HealthCare IT Experts Blog retweeted
Every NHCX transaction gets a unique correlation ID, similar to a package tracking number.
If a request fails to reach its recipient, the gateway retries automatically. If it still fails, the ID is deactivated, preventing duplicate or ghost transactions from circulating.
1
2
2
12
The HealthCare IT Experts Blog retweeted
Right now, eligibility checks involve reaching out to each payer through their own process.
Under NHCX, providers send a single structured digital request. The gateway routes it. The payer responds through the same channel. Every time, in the same format.
#CaladriusHealthAI
1
2
2
11
The HealthCare IT Experts Blog retweeted
Standardization rarely gets credit for the operational work it does.
But in a system where every payer communicates differently, a common protocol changes more than just the technology. It changes how work gets done every day.
Here is what NHCX introduces in practice 🧵#NHCX
1
2
2
20
The HealthCare IT Experts Blog retweeted
Full practical guide: architecture, FHIR, authentication, error handling, and pitfalls linked below.
Part 5 of the CaladriusHealth.AI NHCX Series.
linkedin.com/pulse/navigatin…
#HealthTech #ABDM
2
2
21
The HealthCare IT Experts Blog retweeted
All data exchange is FHIR Bundles: eligibility, pre-auth, claims, responses.
And the gateway is protocol-strict. Wrong status code, reused Correlation ID, expired token, any of these terminates the transaction.
1
2
2
23
The HealthCare IT Experts Blog retweeted
NHCX is asynchronous.
Request goes out → HTTP 202 confirms receipt → actual response arrives later via callback.
Dropped callbacks mean lost claims.
1
2
2
10
The HealthCare IT Experts Blog retweeted
Connecting to NHCX isn't just an API integration.
It's a shift in how systems communicate: asynchronous, FHIR-native, and protocol-strict.
A quick breakdown. 🧵#NHCX #CaladriusHealthAI
1
2
3
29
The HealthCare IT Experts Blog retweeted
83 payers. 43278 providers. 23 million claims.
NHCX is active infrastructure, and the global playbook offers a clear roadmap for what comes next.
linkedin.com/pulse/beyond-nh…
3
3
38
The HealthCare IT Experts Blog retweeted
Full written analysis 👇
linkedin.com/pulse/beyond-in…
Video breakdown 👇
youtu.be/AtiQpFr6TnU?si=OOqC…
#HealthInsurance
2
2
14
The HealthCare IT Experts Blog retweeted
This is an ecosystem maturing toward greater efficiency, transparency, and better outcomes for policyholders.
Every participant has a role in shaping what that looks like.
1
2
2
19
The HealthCare IT Experts Blog retweeted
The investor signal worth watching.
India's insurtech sector has attracted significant cumulative venture funding, concentrated largely in distribution.
As NHCX matures, attention is shifting toward claims technology, data analytics, and clinical services.
1
2
2
26