
Director @sfhealthnetwork HF Program Zuckerberg SF General Hospital @zsfgcare @ucsfcardiology. New Dad x2! Alum @WUSTLmed⬅️ @UCSFmedicine⬅️ @cornell he/his/him
Joined April 2014
- Tweets 3,180
- Following 585
- Followers 3,128
- Likes 13,995
100 Photos and videos



Pinned Tweet

14 Jun 2020
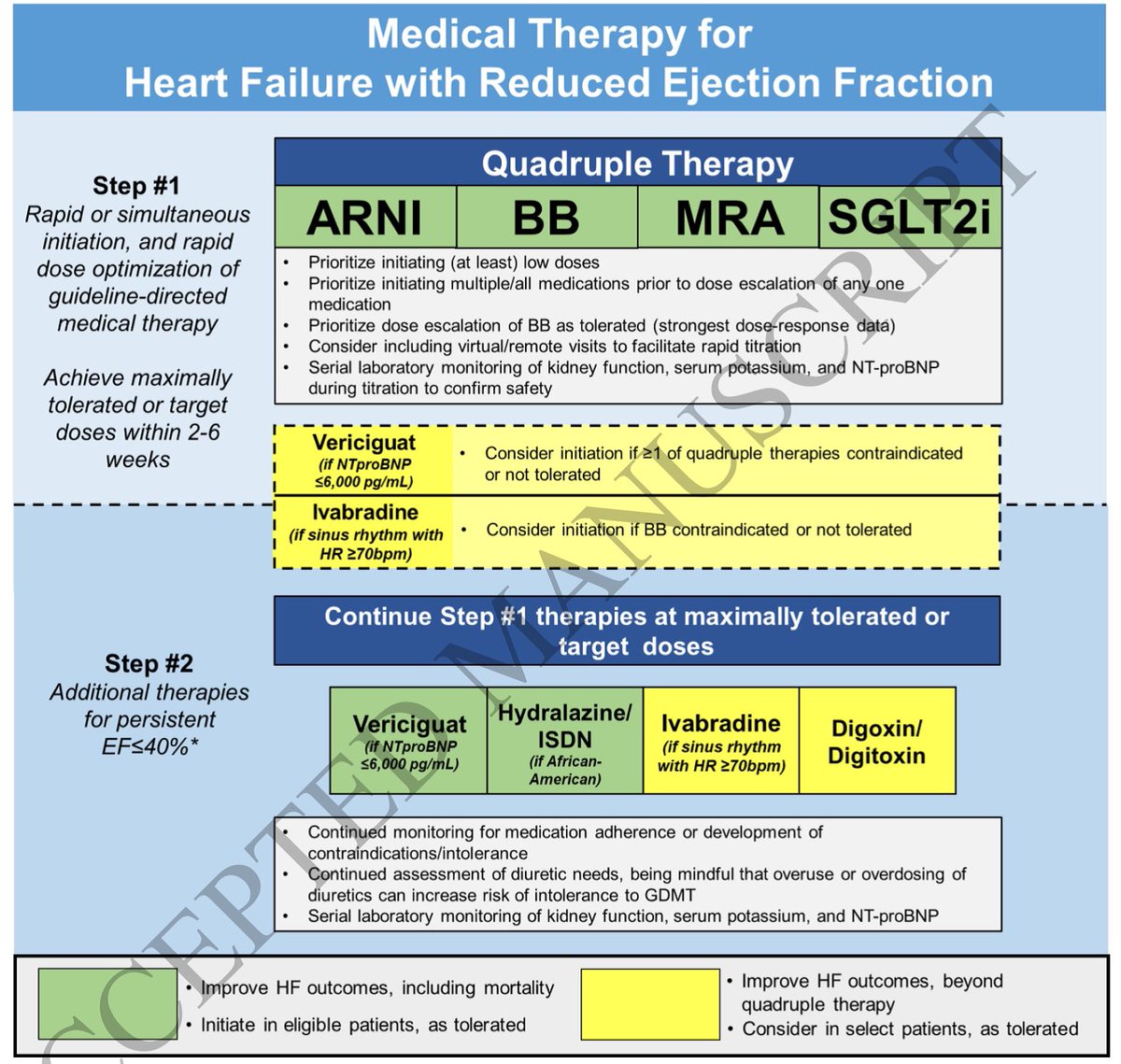
The 3 rules of #GDMTWorks for #HFrEF:
1. Start more
2.⬆️doses
3. Keep them going
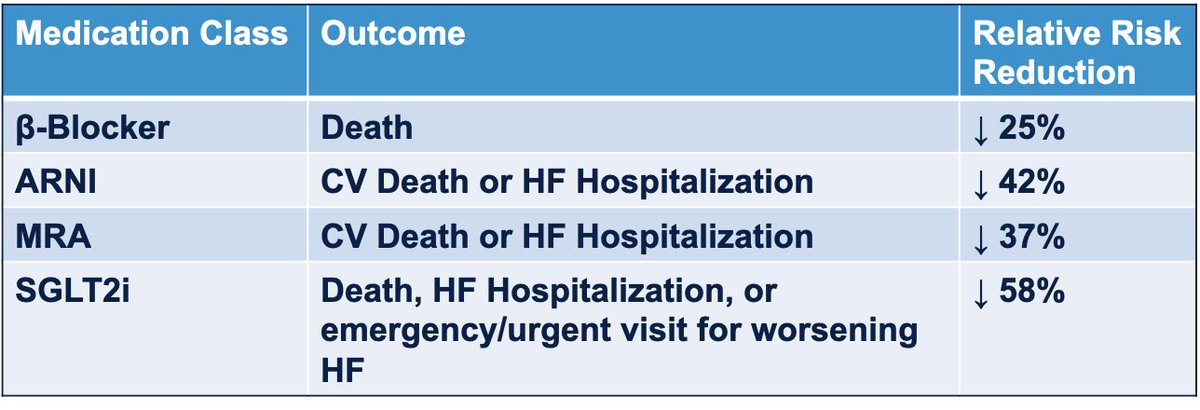
#QuadTherapy: BB ARNI MRA SGLT2-I. 75% RR reduction w NNT of <4!! @gcfmd @MKIttlesonMD @AndrewJSauer @AminYehyaMD @mpsotka @DrNasrien @shwinner @ShelleyZieroth @iamritu @DevinMehta @datsunian
11
39
201
Jonathan Davis, MD, MPHS retweeted

Jun 6
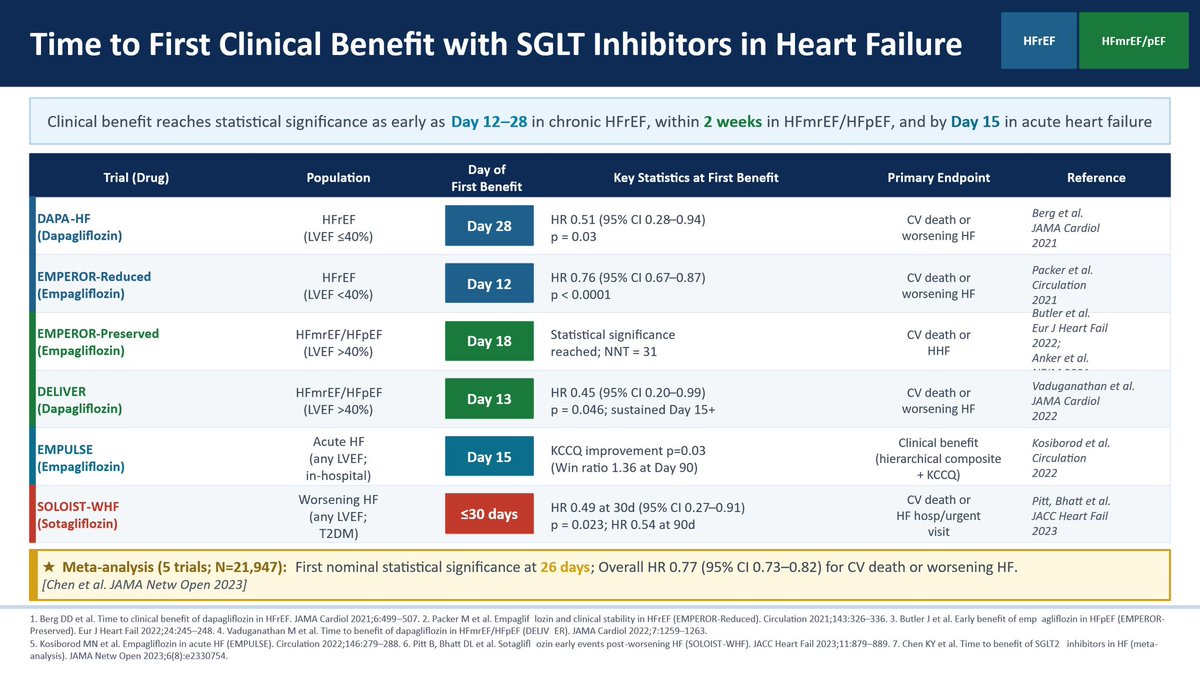
❤️🩹 Heart failure
💊 SGLT inhibitors
🚀 Ultrafast clinical benefits (across the EF spectrum)
Amazing value
🛎️ What are you waiting for?
2
39
74
4,519
Jonathan Davis, MD, MPHS retweeted
May 27
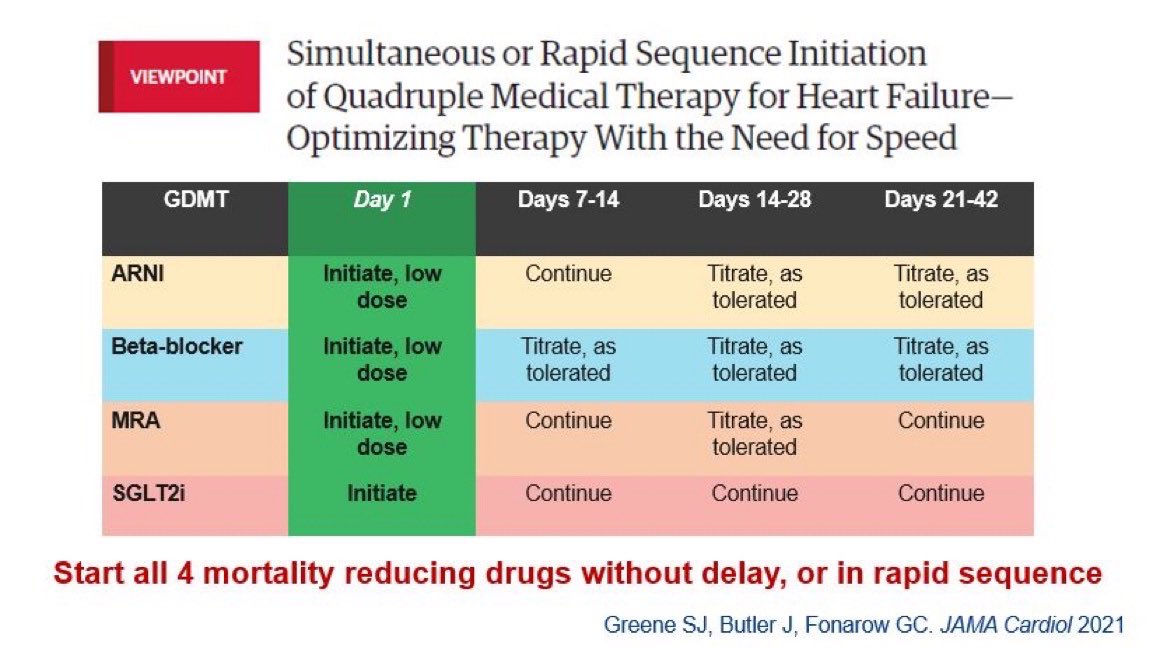
Is the simultaneous/rapid sequence initiation strategy for GDMT for HFrEF superior to usual care one by one approach?
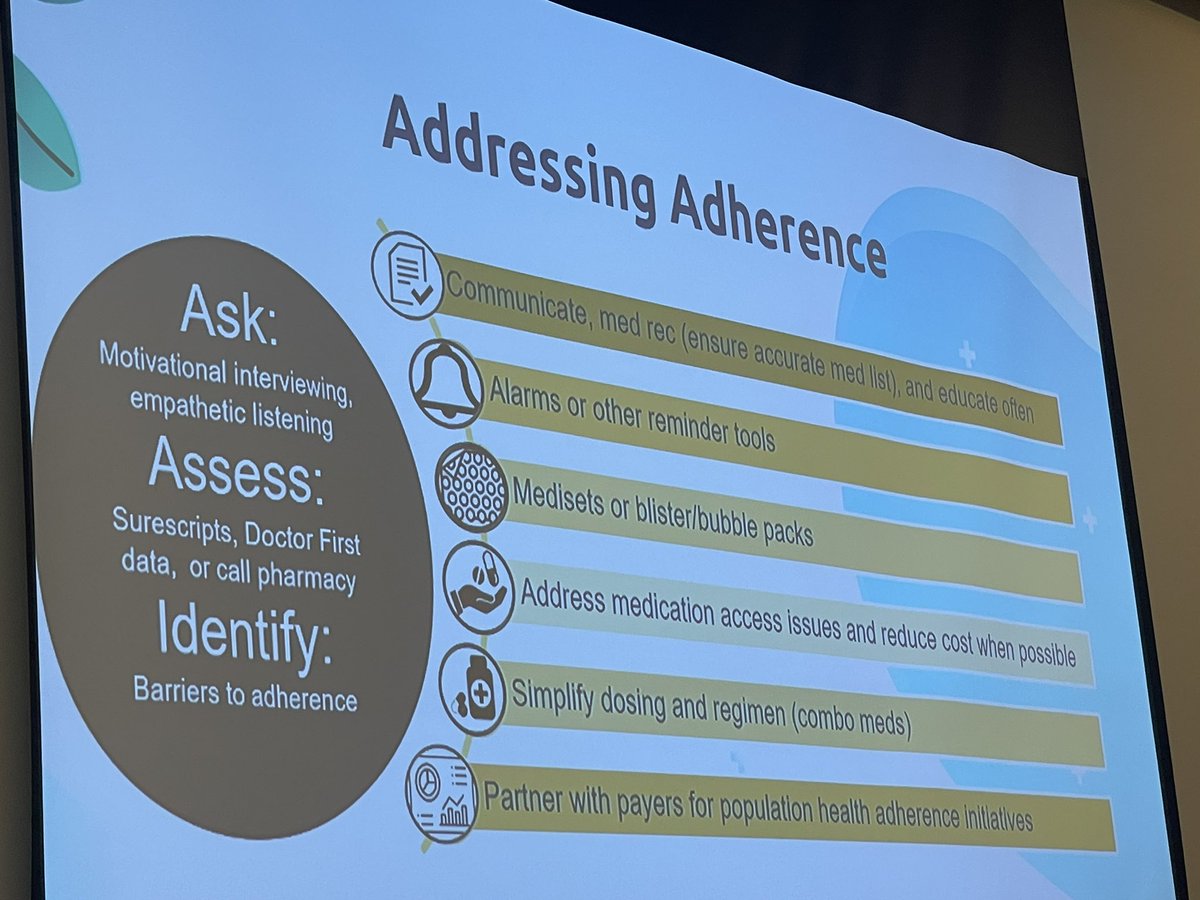
✅ Better use, dosing, adherence, and persistence
✅ Safe, well tolerated, less HF events
In both the 🏨 and outpatient clinic setting
🎯STRONG-HF
🎯 SHORT

1
7
26
1,487
Jonathan Davis, MD, MPHS retweeted
May 26
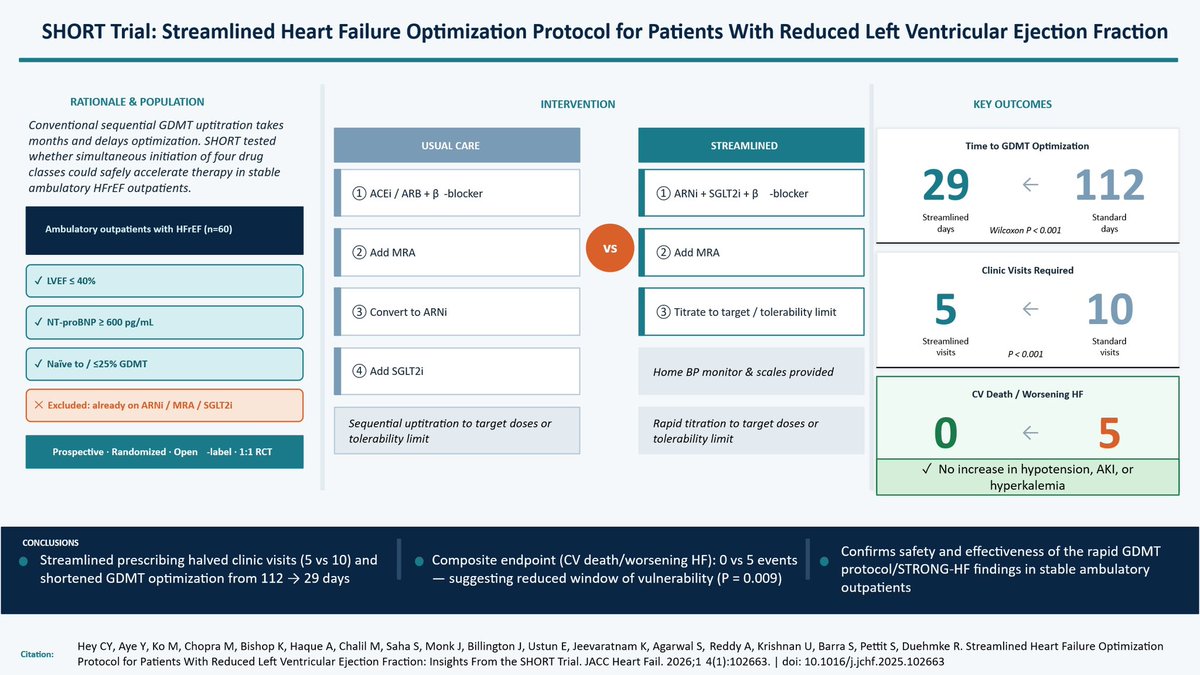
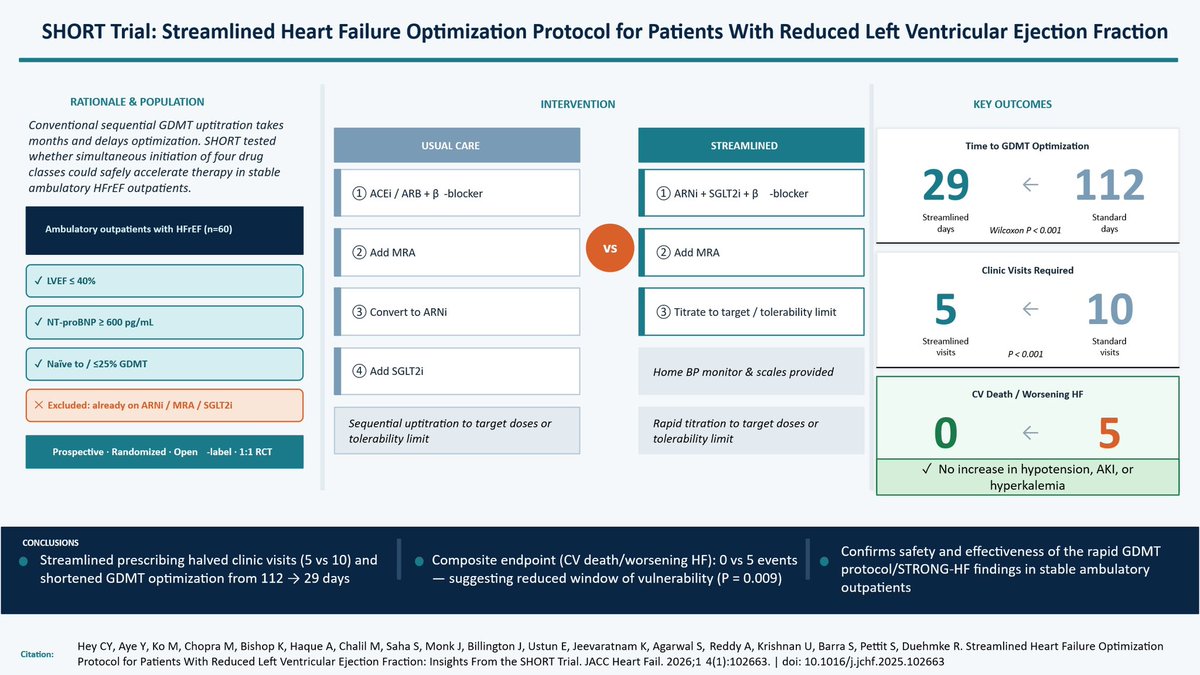
Can quadruple GDMT be simultaneously initiated and rapidly uptitrated in ambulatory outpatients with HFrEF?
The SHORT RCT
✅ Time to quadruple GDMT optimization 29 days vs 112 with usual care
✅ safe, well tolerated, less visits, less HF events
jacc.org/doi/10.1016/j.jchf.…
1
8
22
1,624
Jonathan Davis, MD, MPHS retweeted
May 25
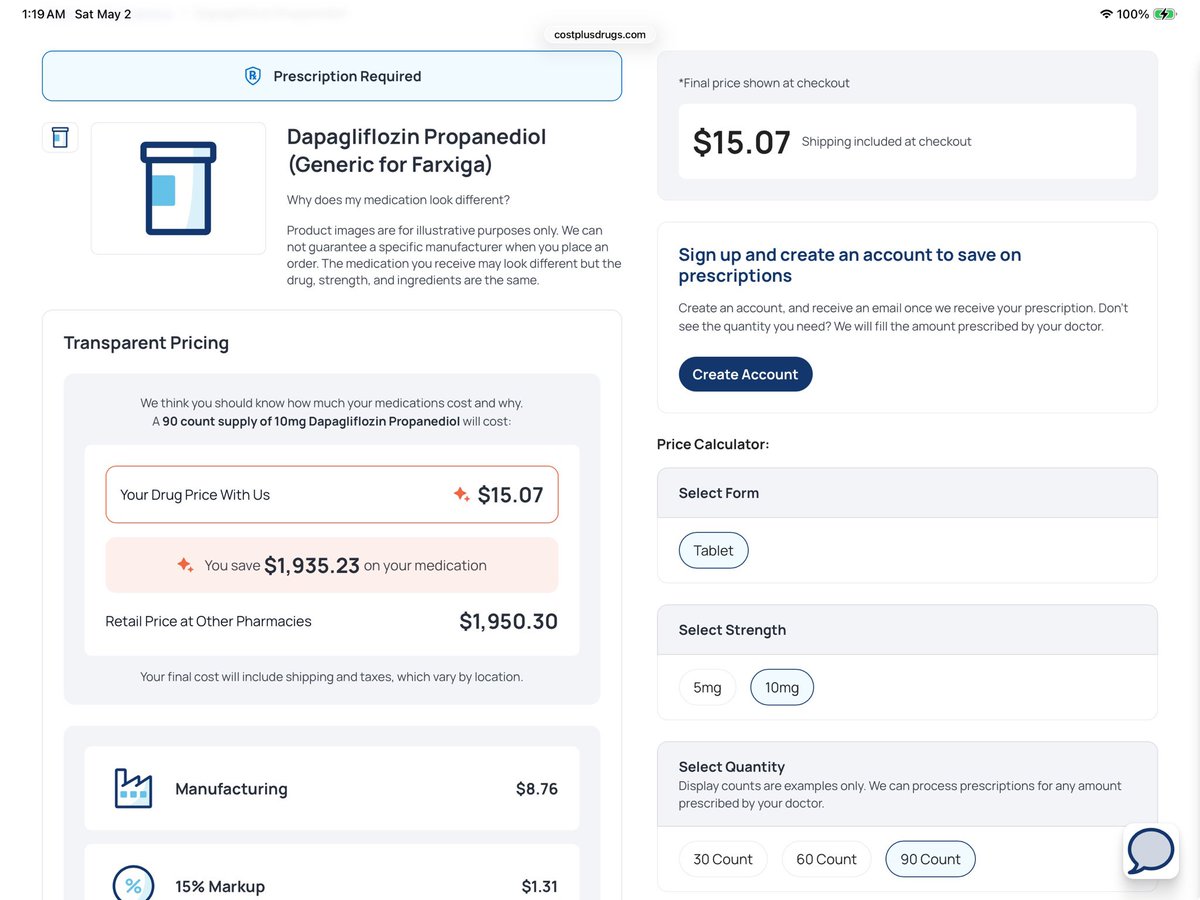
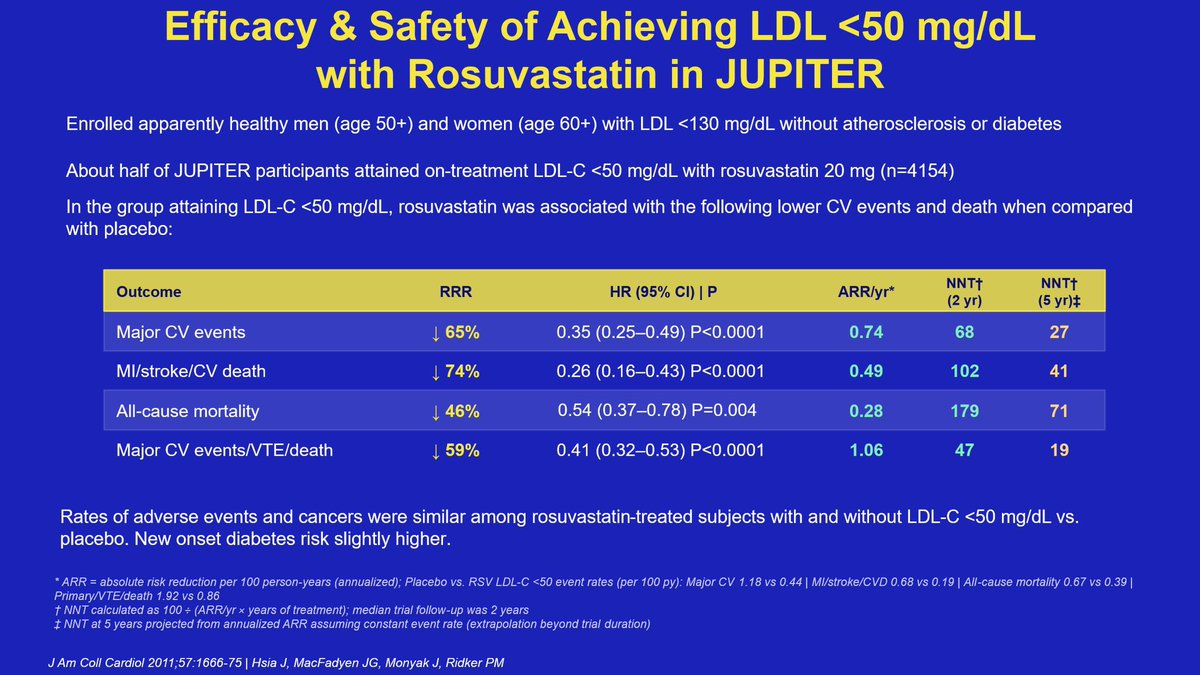
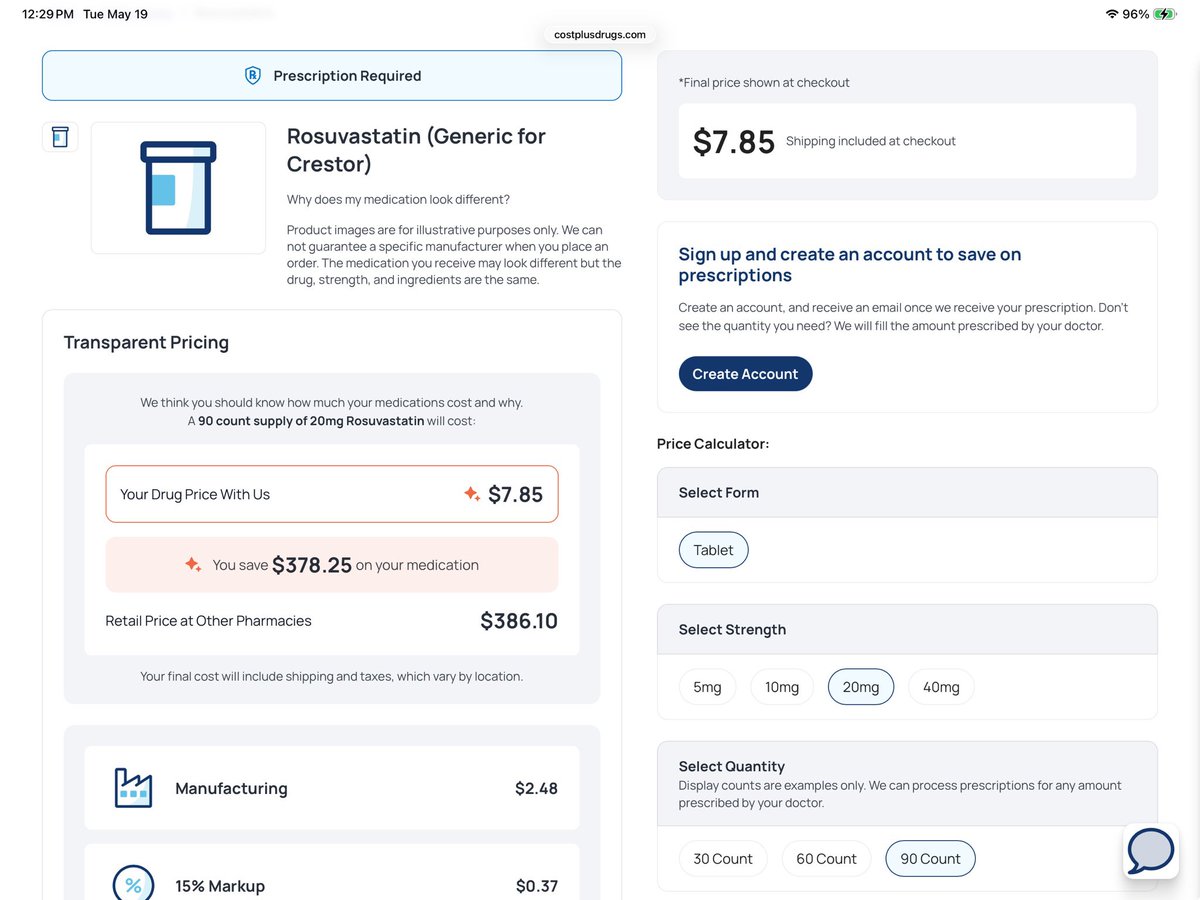
Rosuvastatin 20 mg for primary prevention and achieving LDL < 50 mg/dL
Clinical benefits>>potential risks
Relative risk reductions: large
Absolute risk reductions: small per year, but accumulate over time
Cost:
$31.40 per year
$2.61 per month
9 cents a day
5
10
57
5,737
Jonathan Davis, MD, MPHS retweeted

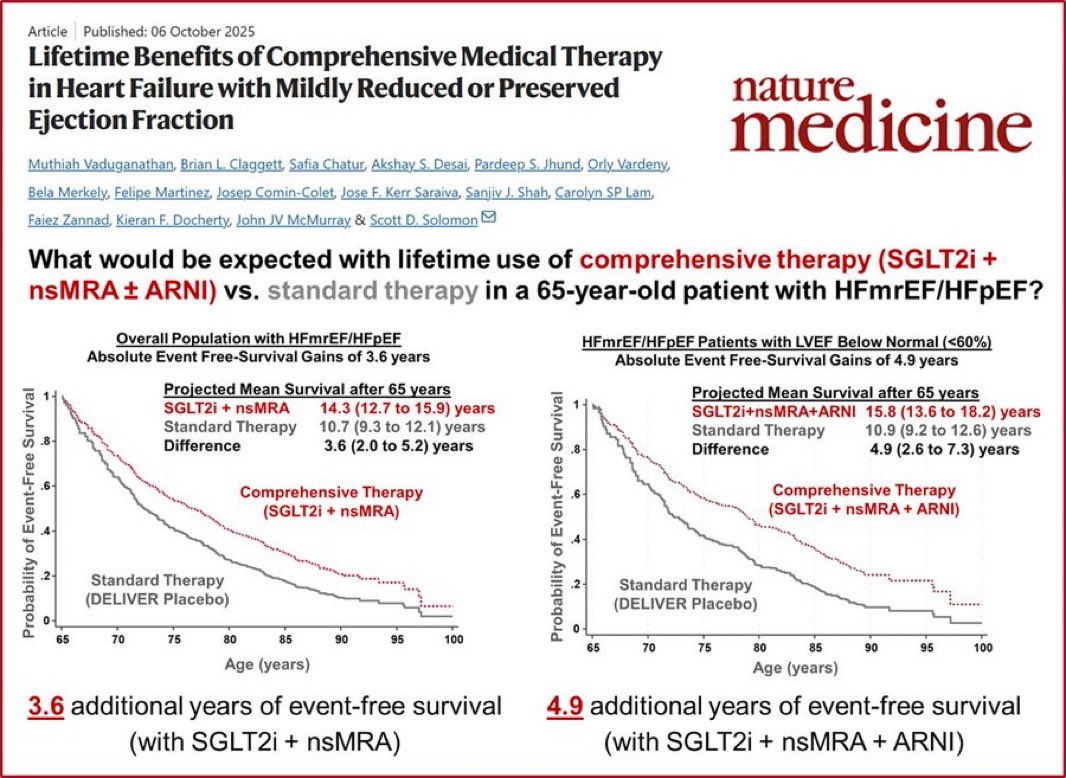
💊🫀 What does optimal therapy actually buy a 65-year-old with HFmrEF/HFpEF?
From Nature Medicine (Vaduganathan et al., 2025):
🔴 SGLT2i nsMRA → 3.6 years event-free survival
🔴 SGLT2i nsMRA ARNI → 4.9 years (LVEF <60%)
vs. standard therapy alone.
Nearly 5 extra years without hospitalization or death.
💡 These drugs exist. They work. Are all eligible patients receiving them?
Vaduganathan et al. Nature Medicine, Oct 2025
@mvaduganathan
#HeartFailure #HFpEF #HFmrEF #SGLT2i #ARNI #Cardiology #MedTwitter #NatureMedicine
3
68
175
11,231
Jonathan Davis, MD, MPHS retweeted
26 Dec 2022
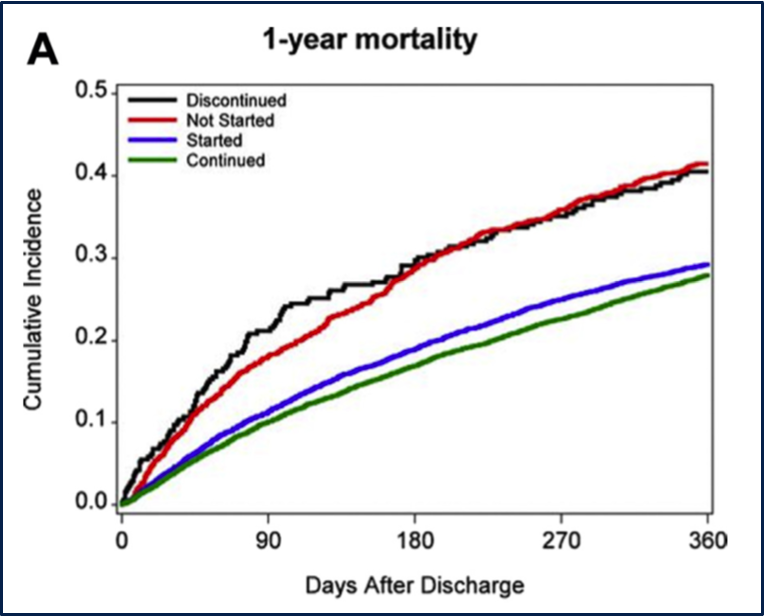
Every admission = opportunity to improve #GDMTWorks! MD, RN, PharmD, etc; QD-BID labs; vitals 4-6x/day... all hands on deck! Take advantage! Major consequences of stopping or not starting! @SJGreene_md @mvaduganathan @gcfmd @JavedButler1 @UCSFIMChiefs
10.1016/j.jchf.2018.06.011
9
27
4,238
Jonathan Davis, MD, MPHS retweeted

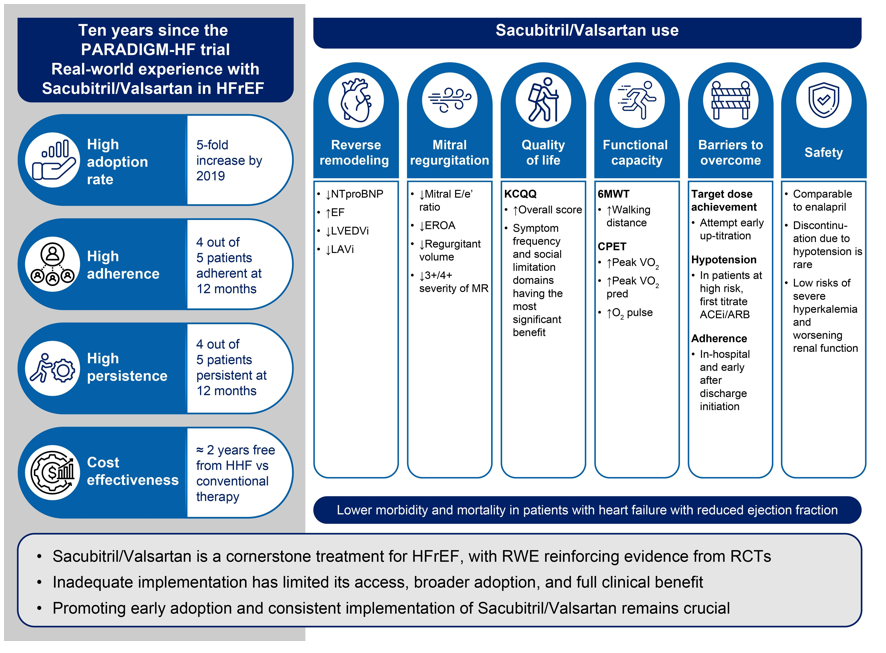
Ten Years Real-World Experience With Sacubitril/Valsartan in Patients With Heart Failure With Reduced Ejection Fraction see @ESC Heart Failure ow.ly/zovq50YKIO1
@EJHFEiC @JanBiegus @Ppponikowski #HFA_ESC @hvanspall @ShelleyZieroth @FudimMarat @gcfmd @MarcoMetra @GianluSava #ESCHeartFailure
3
25
80
5,779
Jonathan Davis, MD, MPHS retweeted
Apr 16
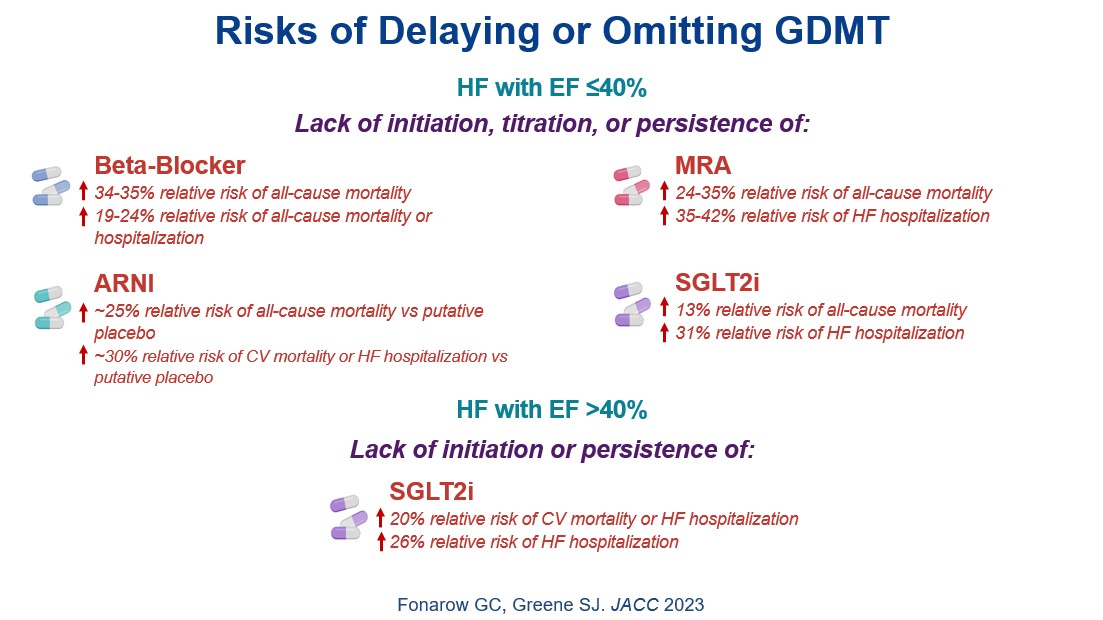
Why are 100% of eligible patients with HFrEF w/o CI or intolerance not receiving quadruple GDMT in 2026?
ARNI BB MRA SGLT2i ➡️
75% ⬇️ all-cause ☠️ (26% ARR, NNT=4, 24 months)
85% ⬇️ HF 🏨 (33% ARR, NNT=3, 24 months)
Extend median survival by 7-11 years
💊 Cost $78/month


2
23
49
4,272
Jonathan Davis, MD, MPHS retweeted

Apr 2
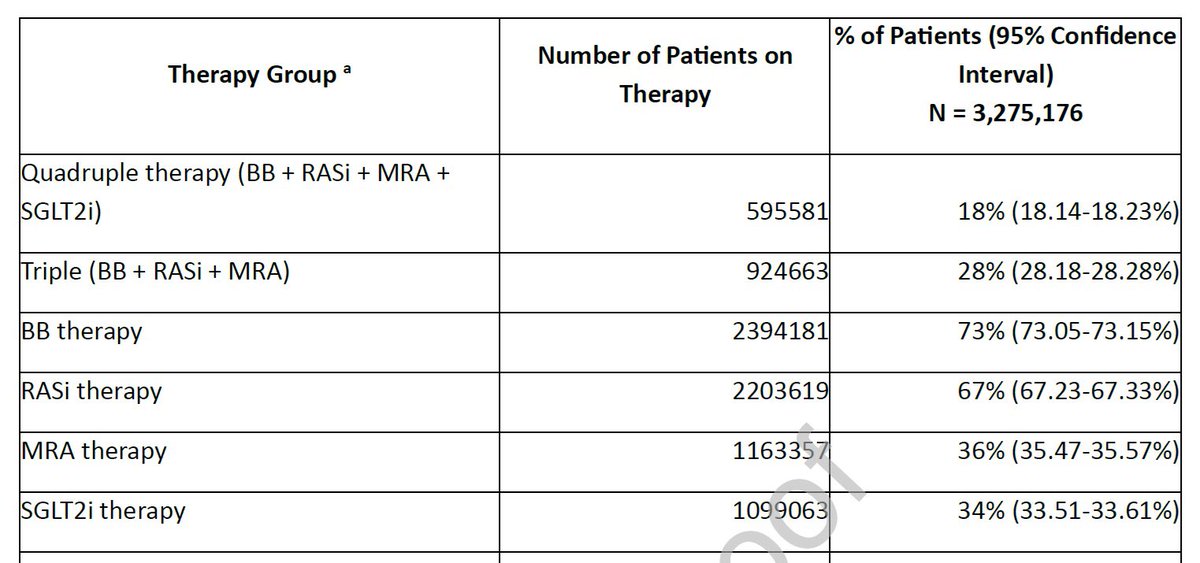
Patients newly diagnosed w/ #HFrEF
>9 of 10 deaths occur among pts who never receive ≥1 💊 proven to ⤵️⤵️⤵️death....
...in a nationwide health system w/ minimal or $0 patient copays for #GDMTworks
🤯🤯🤯
@gcfmd @JavedButler1
jamanetwork.com/journals/jam…
1
21
44
6,664
Jonathan Davis, MD, MPHS retweeted
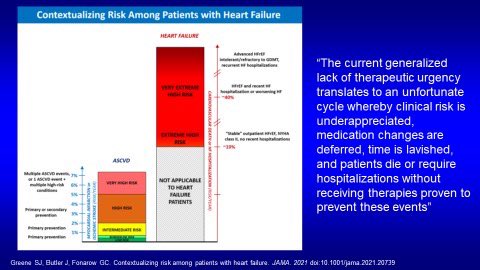
Apr 2
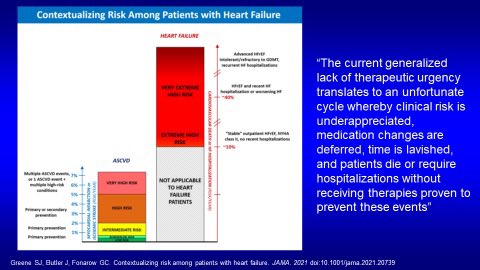
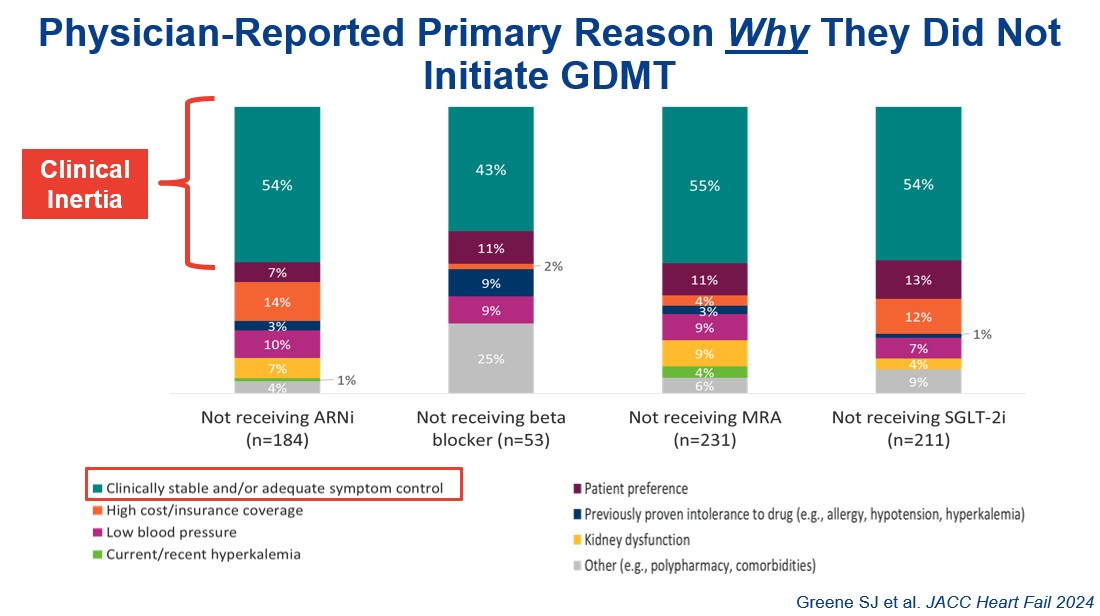
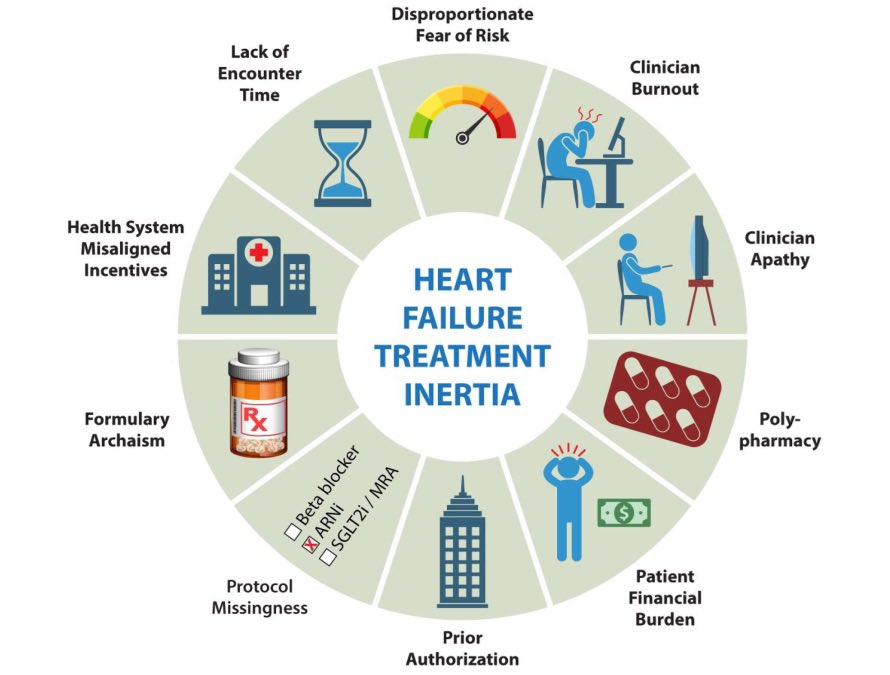
Treatment inertia, misperception of clinical risk, and lack of therapeutic urgency are highly lethal in HFrEF
Take action now!
1
13
32
1,875
Jonathan Davis, MD, MPHS retweeted
Apr 2
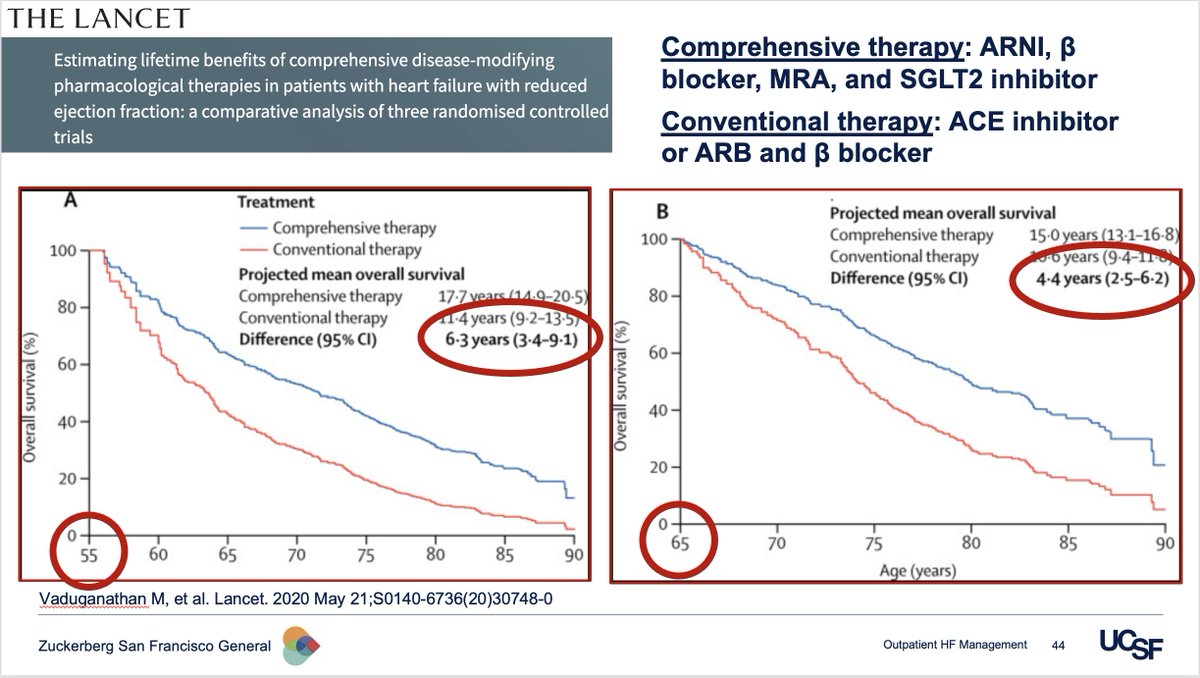
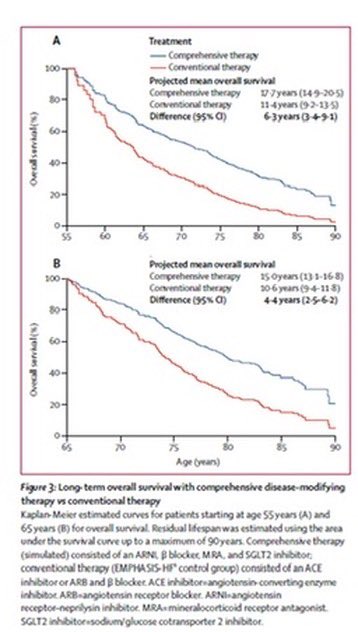
HFrEF in 2026
Most common Rx is use still ACEI/ARB BB, despite Class 1 recommendation for quadruple GDMT
ACEI/ARB BB ➡️ ARNI BB MRA SGLTi
Extends median survival:
6.3 years
75.6 months
2300 days
55,188 hours
3,311,280 minutes
💊s cost extra $70 per month
Worth it?

4
29
80
6,444
Jonathan Davis, MD, MPHS retweeted

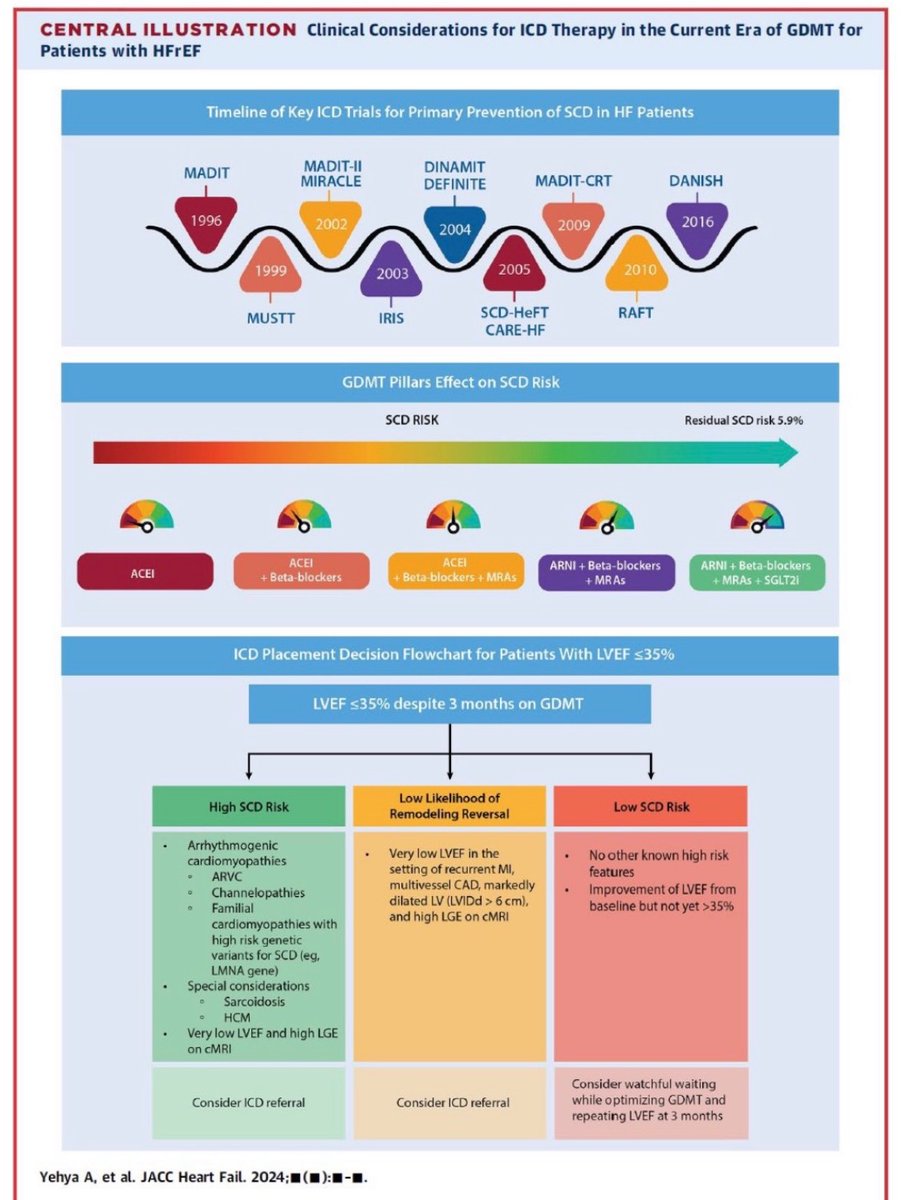
6 Dec 2024
Thankful for my coauthors: Jose Lopez, Andrew Sauer, Jonathan Davis, Nasrien Ibrahim, Rod Tung, Biykem Bozkurt, Gregg Fonarow, and Sana Al-Khatib.
Link: sciencedirect.com/science/ar…
1
2
15
1,609
Jonathan Davis, MD, MPHS retweeted
Feb 27
Considerations for Rx beyond the foundational 4 pillars of disease modifying guideline-directed medical therapy for HFrEF
1
15
40
1,843
Excited to share this news piece about one of our #heartsuccess patients in our Heart Failure Clinic @mercysaintlouis, setting the standard for #heartfailure care in the @STLCounty @STLCityGov region @American_Heart @ACCinTouch @HFSA
youtu.be/8u6CGTniZNY?si=JVXI…
1
3
675
30 Oct 2025
I am speaking at UCSF 29th Annual Management of the Hospitalized Patient. Please check out my talk if you're attending the event! #Bob_Wachter #MHP2025 - via #Whova event app
2
1
6
495
Jonathan Davis, MD, MPHS retweeted
14 Oct 2025
To Mandrola's original point: 🔑is definition of "decompensated"
We should not initiate BB in hemodynamic instability/shock
But "decompensated" is not synonymous w/ entirety of a HF hospitalization.
In-hospital/pre-discharge initiation BB is evidence-based routine approach.
1
9
288
Jonathan Davis, MD, MPHS retweeted

14 Oct 2025
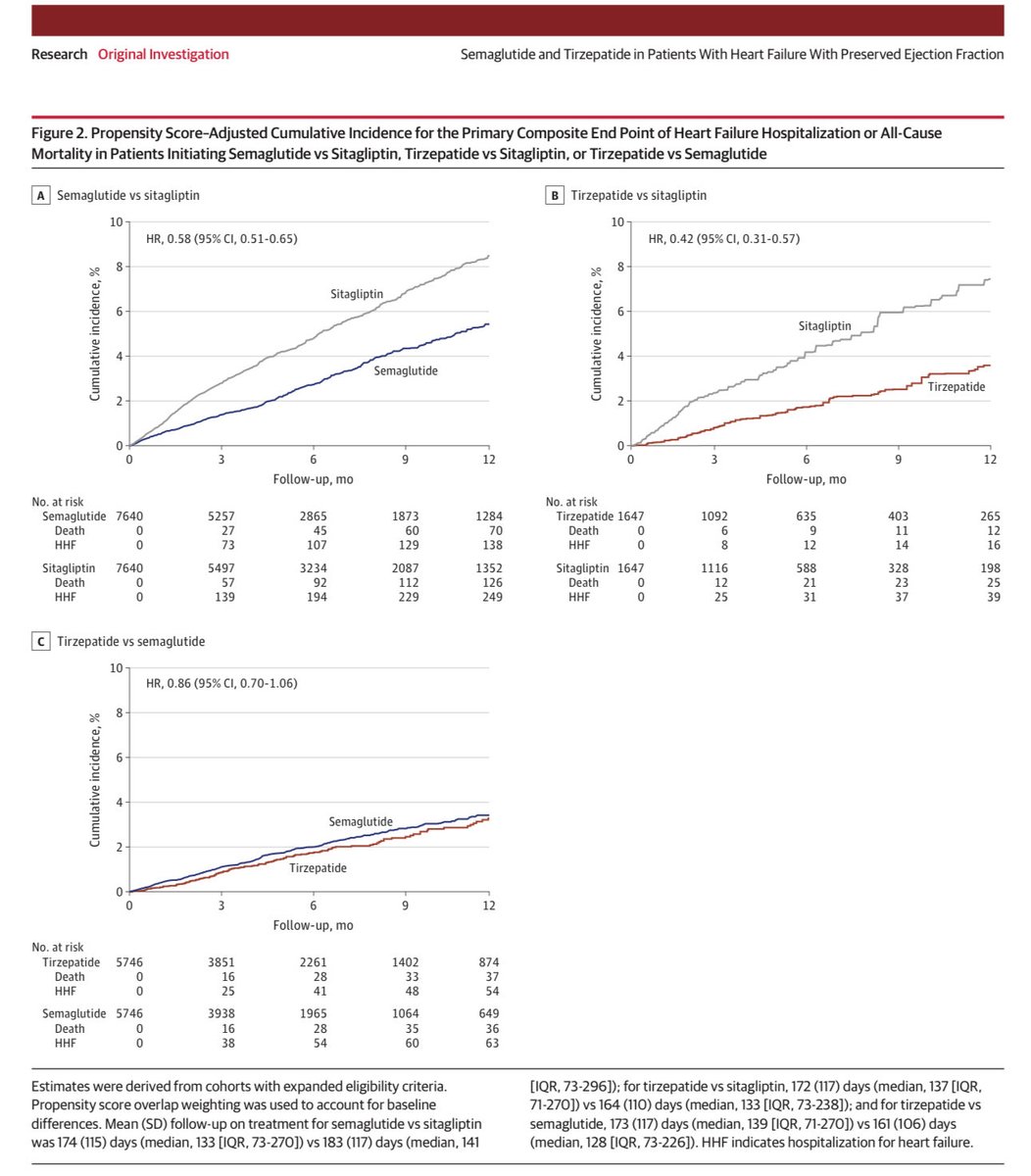
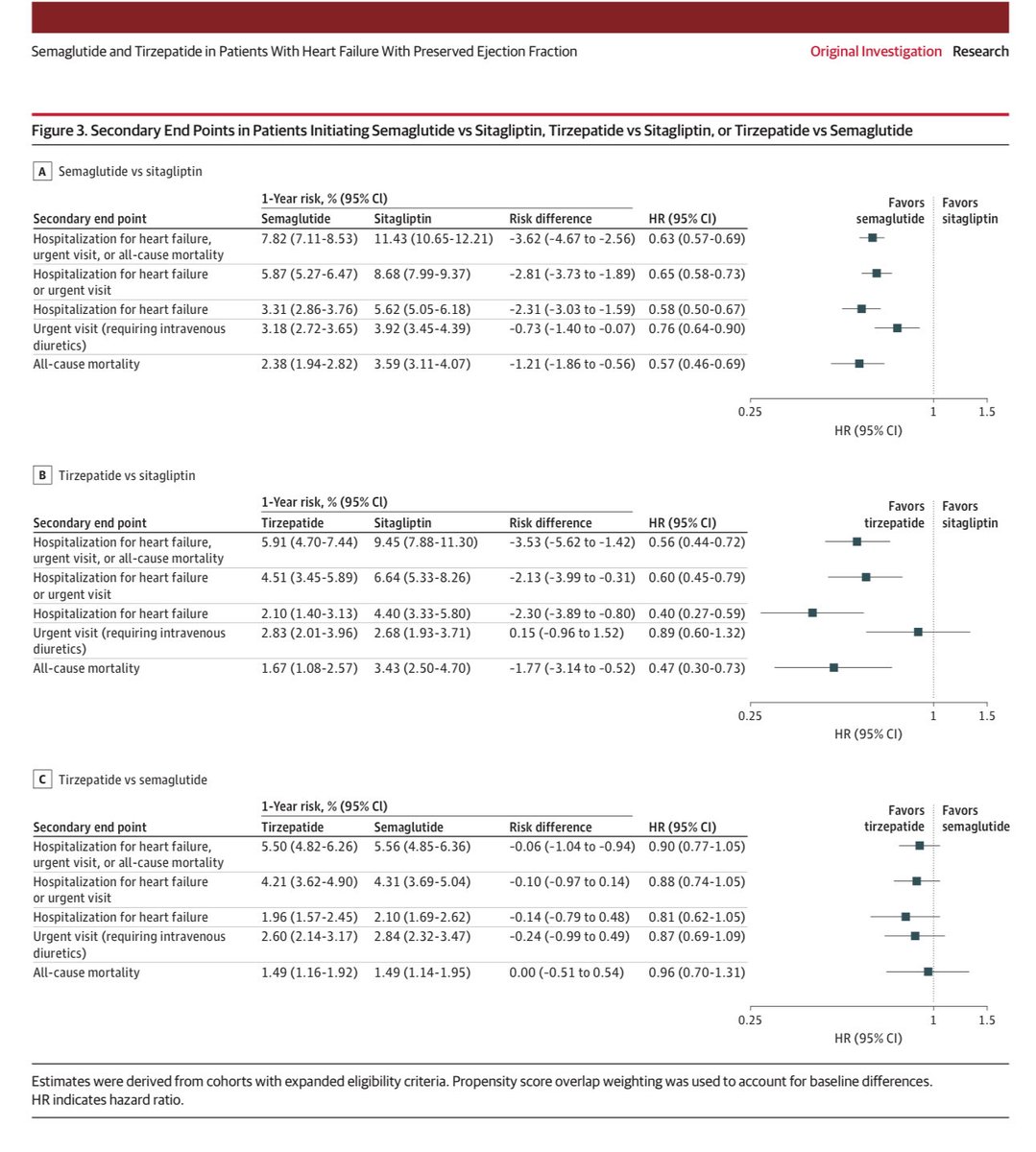
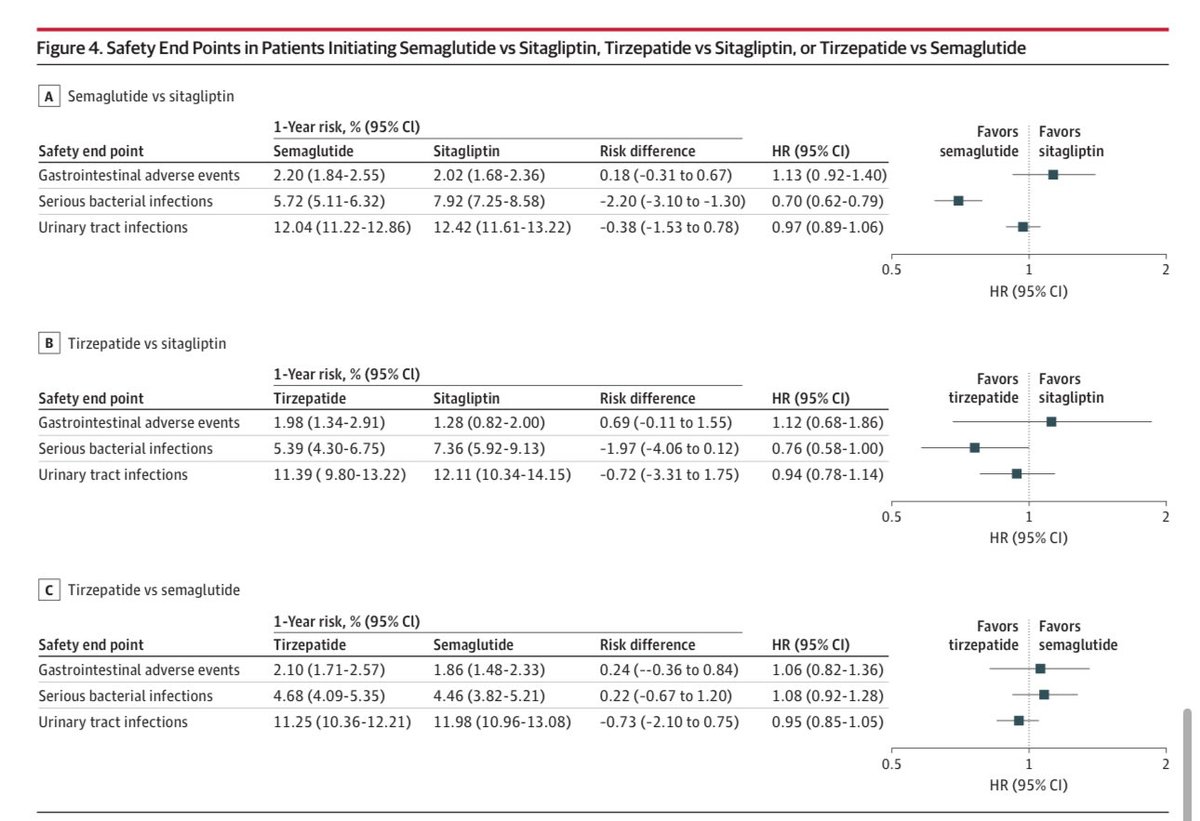
Semaglutide and Tirzepatide in Patients With Heart Failure With Preserved Ejection Fraction
jamanetwork.com/journals/jam…

1
19
67
6,011
14 Oct 2025
Excited to formally launch our #HeartFailure Clinic at @FollowMercy St. Louis. Offering comprehensive, state-of-the-art, guideline-direct care for anyone with heart failure across the ejection fraction spectrum! #heartfunction #heartsuccess
24
1,275
Jonathan Davis, MD, MPHS retweeted

14 Oct 2025
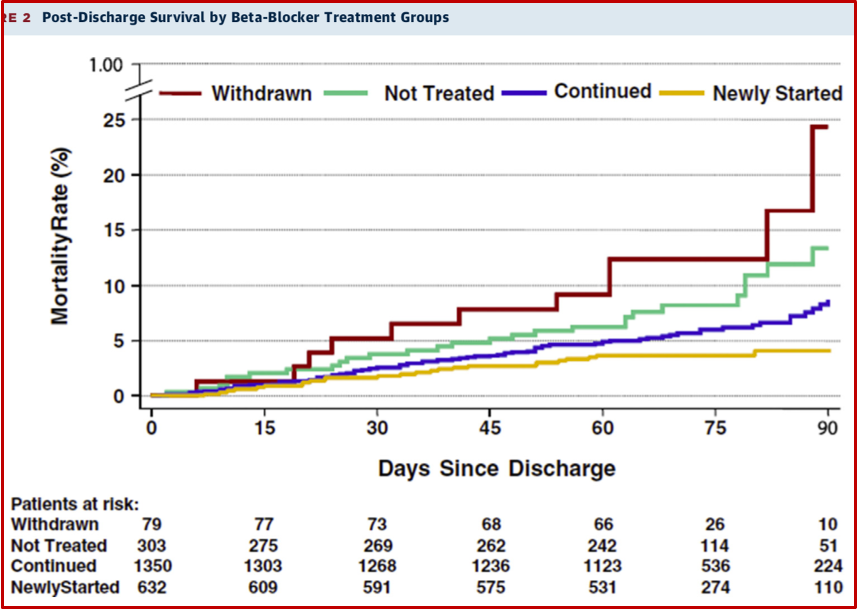
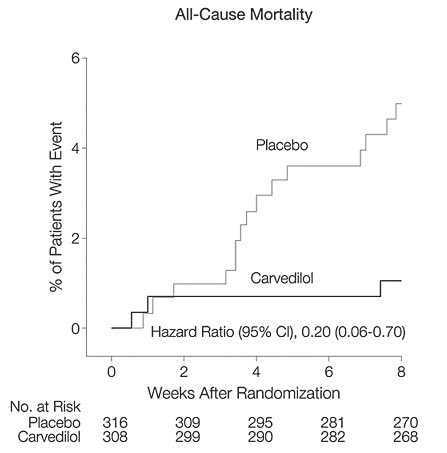
β-blockers safe pre-discharge in #HFrEF
#COPERNICUS ☠️ benefit in recent decomp
jamanetwork.com/journals/jam…
#STRONGHF rapid uptritration ⬇️ events
thelancet.com/journals/lance…
#IMPACTHF ⬆️ Rx persistence
jacc.org/doi/10.1016/j.jacc.…
#BCONVINCED stopping not helpful
academic.oup.com/eurheartj/a…
13 Oct 2025

Heart failure colleagues. I would propose a new focus of emphasis
Re the acute Rx of newly decompensated systolic failure. We should favor afterload reduction FIRST.
Seminal Beta-blocker trials were in ambulatory outpts.
Giving BB to decompensated failure is a mistake. IMO.
4
25
112
19,925
29 Sep 2025
9/29 I start at Mercy St. Louis!
Working at @UCSFHospitals/@ZSFGCare/@UCSFCardiology was a profound privilege. The community, patients, & colleagues gave me more than I can ever express. Please know how grateful I am to have been part of this extraordinary team.
8
3
32
3,177