
Thoracic surgeon, Brigham and Women’s Hospital. Tweets are my own and do not reflect the opinions of BWH or it’s administrators.
- Tweets 52
- Following 181
- Followers 597
- Likes 193













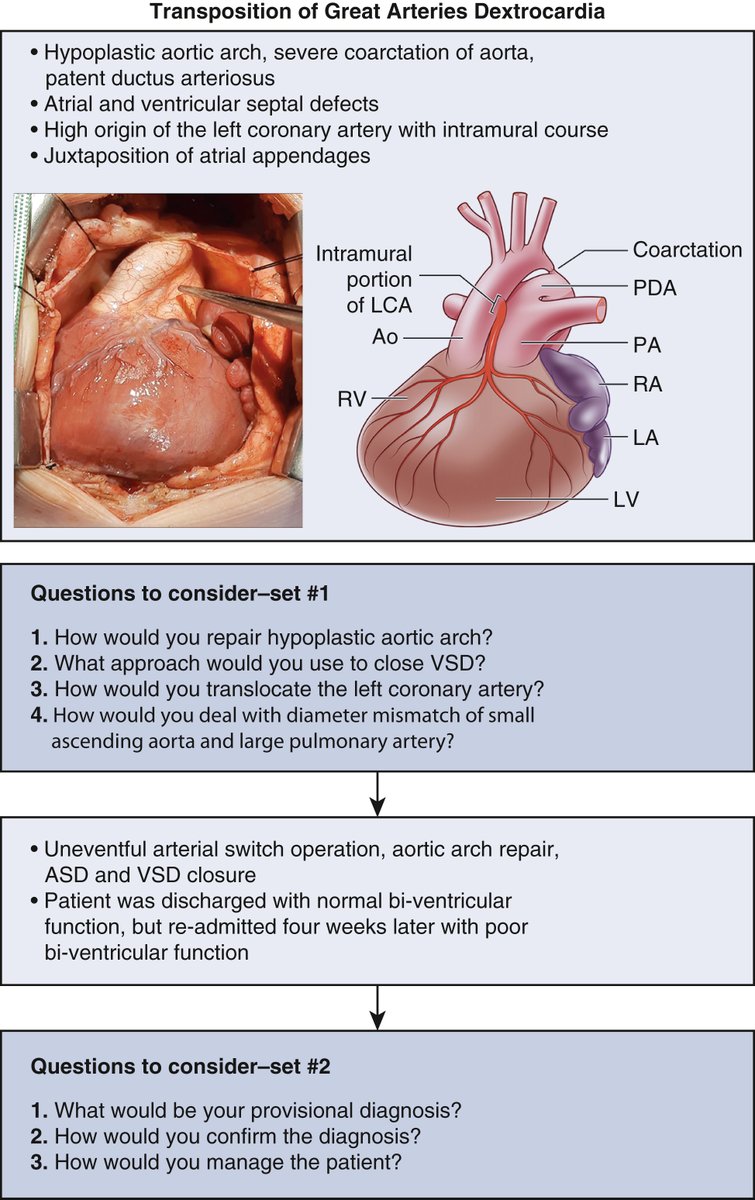
ALT Questions to consider in the management of a rare patient with transposition of great arteries and dextrocardia. PDA, Patent ductus arteriosus; LCA, left coronary artery; Ao, aorta; PA, pulmonary artery; RV, right ventricle; RA, right atrium; LA, left atrium; LV, left ventricle; VSD, ventricular septal defect; ASD, atrial septal defect.

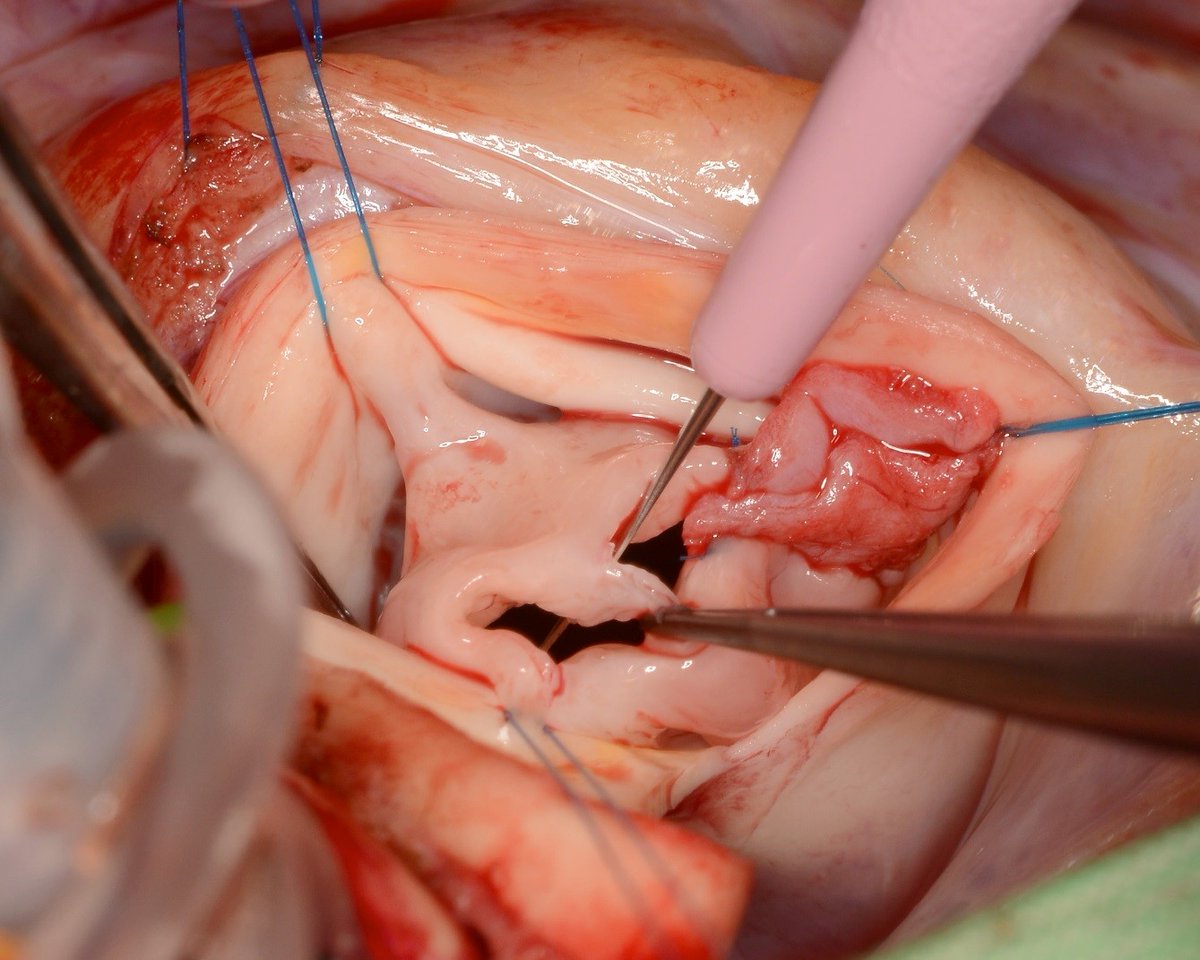
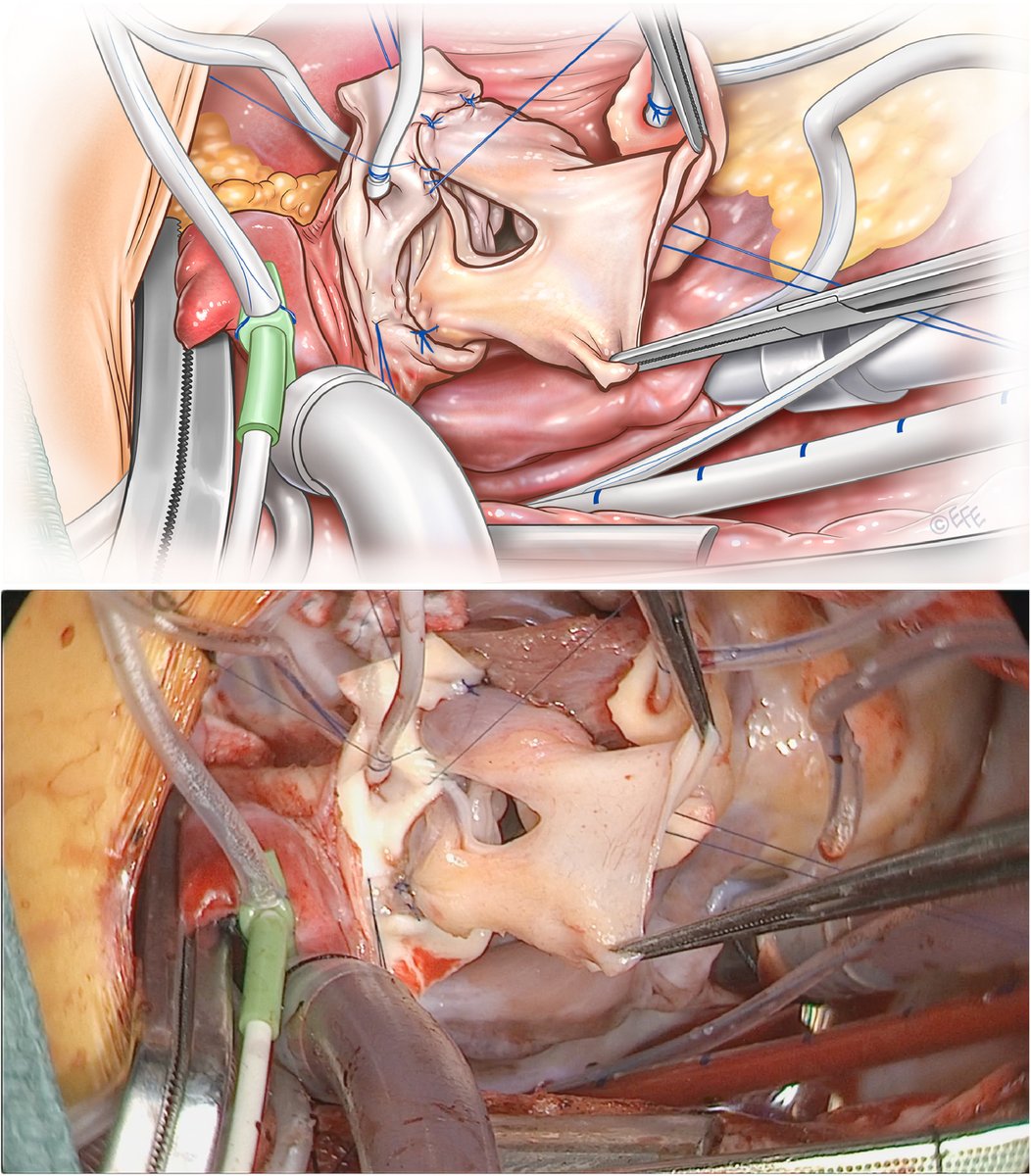
ALT Removal of aortic valve and evaluation of the left ventricular outflow tract.
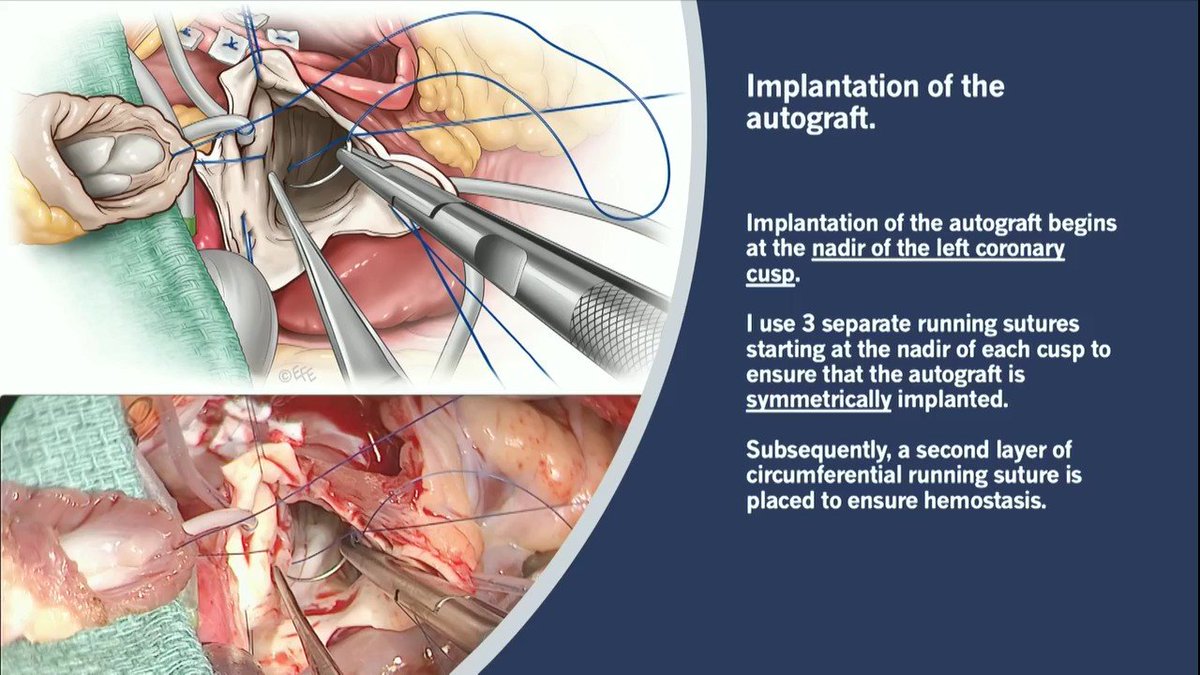





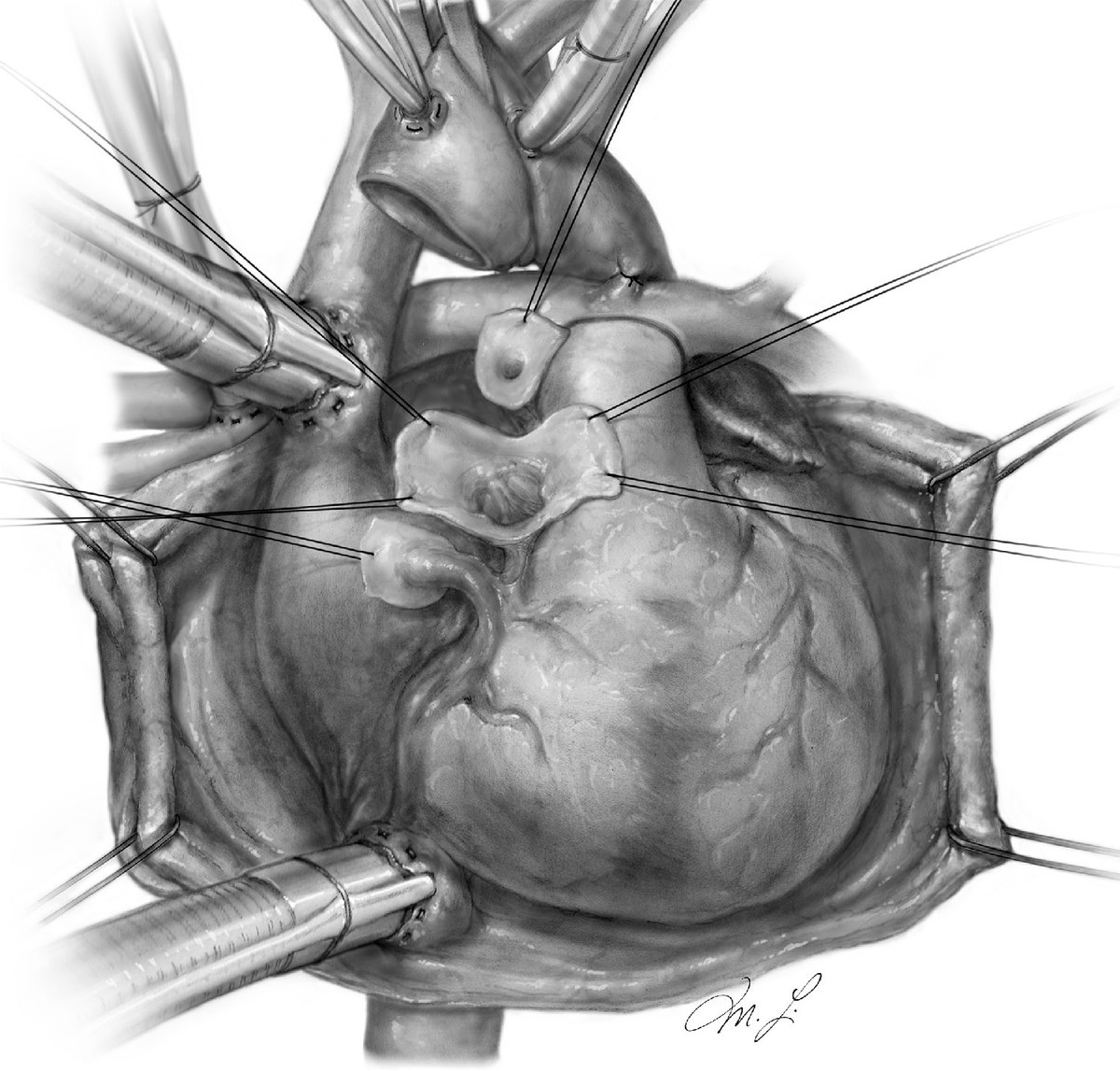
ALT Implantation of the left coronary artery. The left coronary artery is left in situ and implanted into the autograft. Leaving the left coronary artery in its native position eliminated the risk of coronary artery distortion.
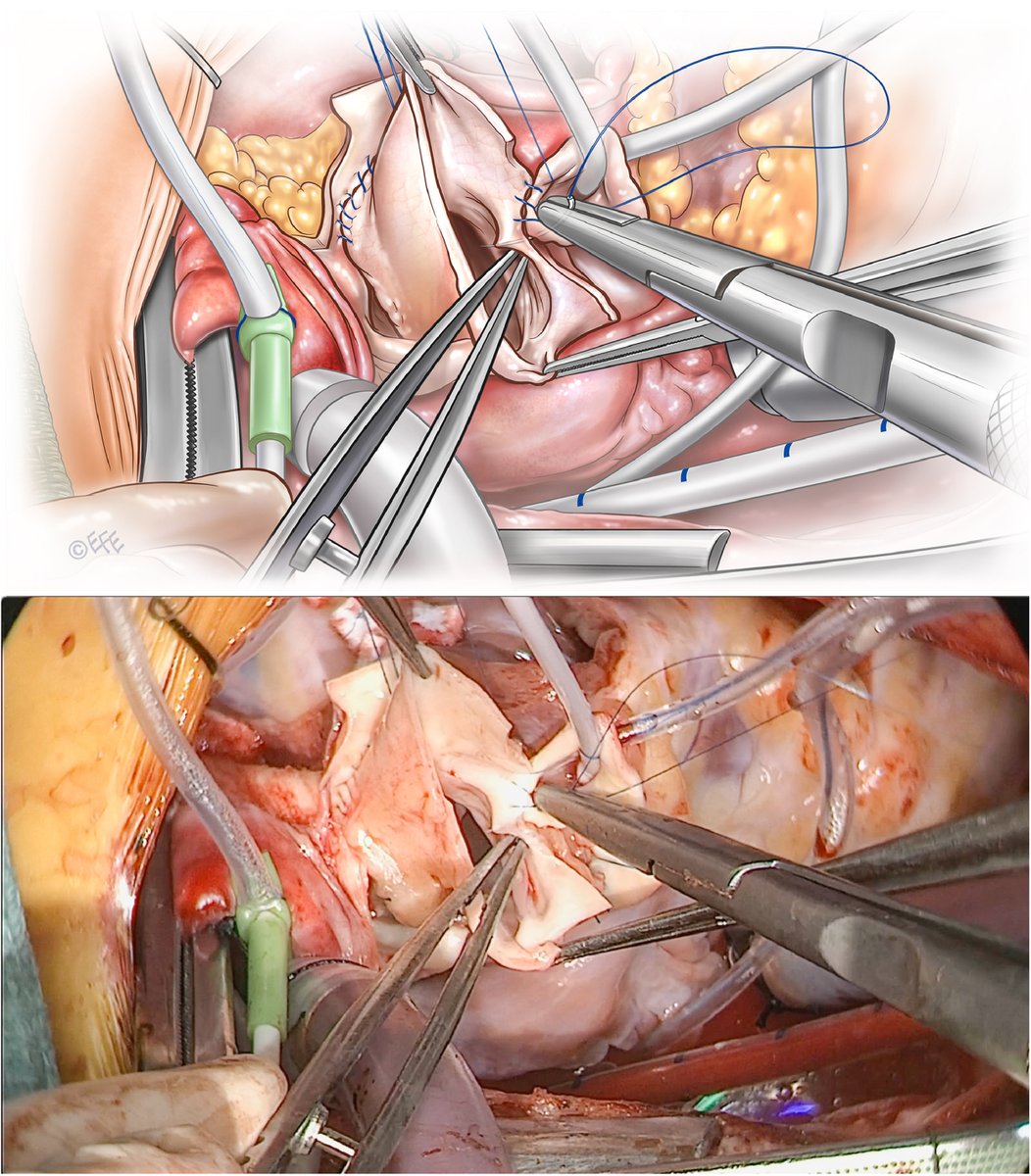
ALT Implantation of the right coronary artery. The incision is made in the middle of the corresponding sinus of the autograft. The right coronary artery is implanted so that the edges of the autograft are connected to each other above the coronary button to avoid inadvertent enlargement of the sino-tubular junction.
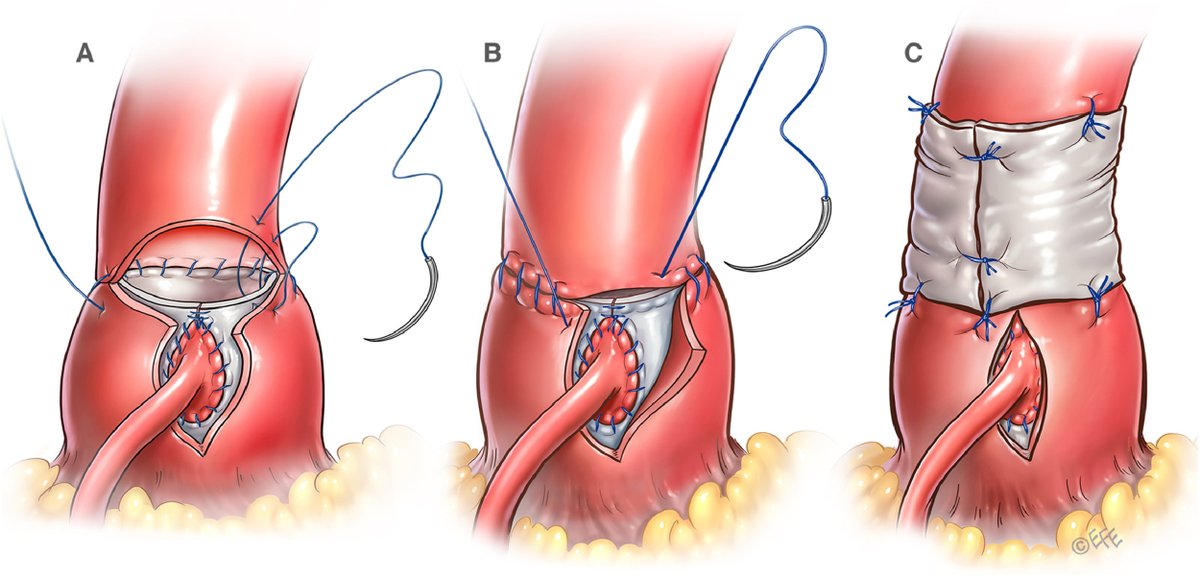
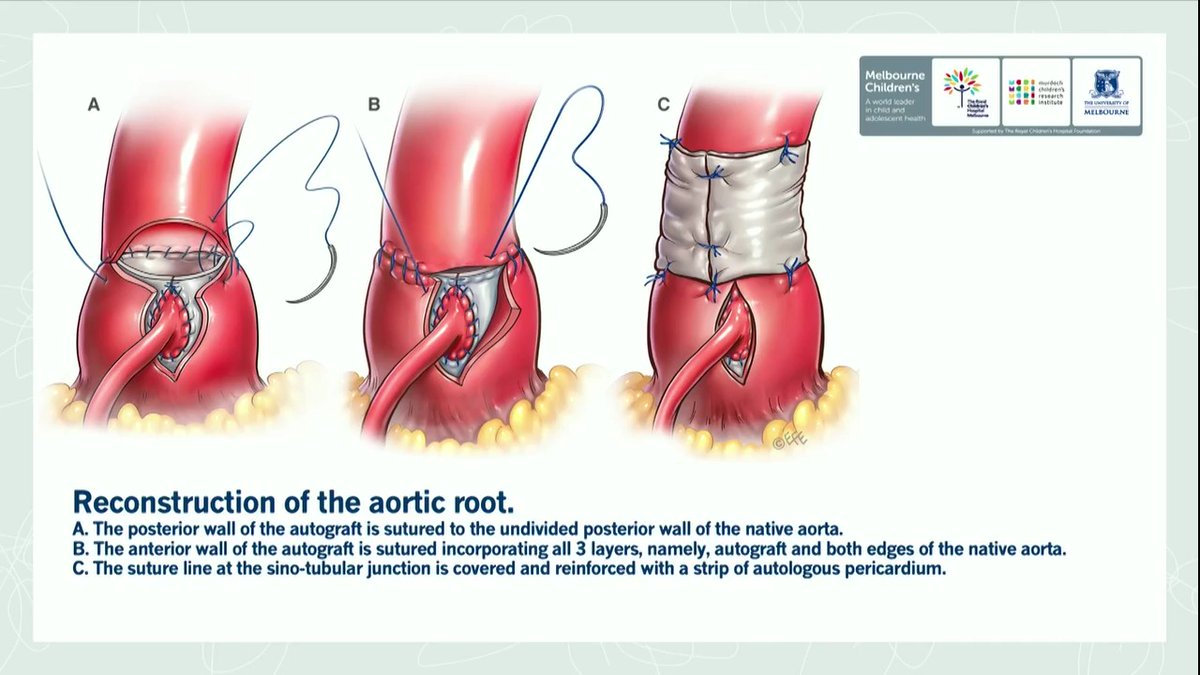
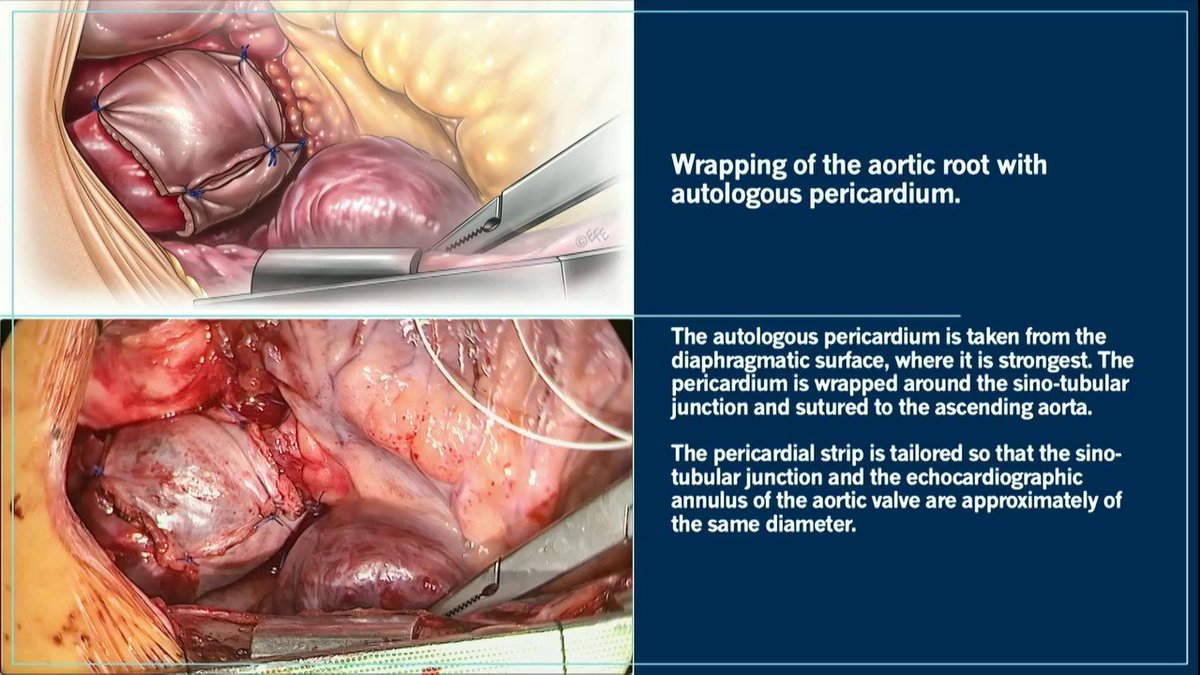
ALT Reconstruction and stabilization of the aortic root. The posterior wall of the autograft is sutured to the undivided posterior wall of the native aorta (A). The anterior wall of the autograft is sutured incorporating all 3 layers (i.e., autograft and the edges of the native aorta) into the suture line (B). The suture line at the sino-tubular junction is covered and reinforced with a strip of the autologous pericardium (C).



ALT The basic tenets of VATS chest wall resection in terms of patient positioning are similar to those of standard VATS procedure for lung resection. Preoperatively, an epidural for chest wall resection is placed. Following successful induction and lung isolation, patient is placed in the lateral decubitus position (with appropriate padding) with the table break maximally flexed at the patient's hip level. Reverse Trendelenburg is used to tilt the table such that the patient's lateral chest wall is in line and parallel to the floor. The table may be rotated to facilitate exposure.
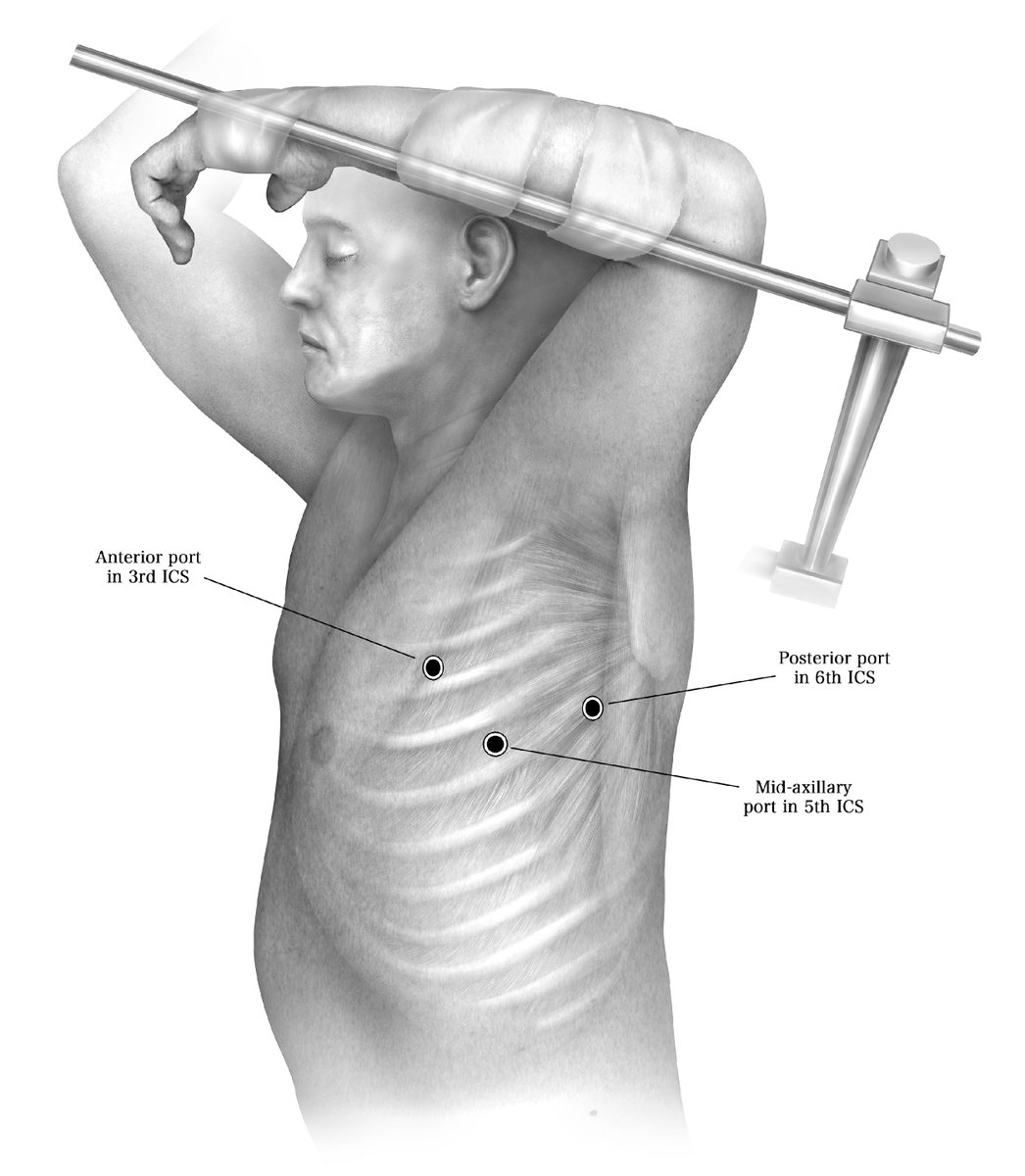
ALT Tumors of the chest wall at the apex requiring resection of the first rib are particularly challenging to manage thoracoscopically due to limited visualization at the apex of the thorax and difficulty of dissection near the thoracic outlet. If amenable to VATS resection, the ports can be placed as shown below: one at the anterior axillary line (Third intercostal space), one at the mid axillary line (Fifth intercostal space) and one in the Sixth intercostal space along the posterior axillary line.
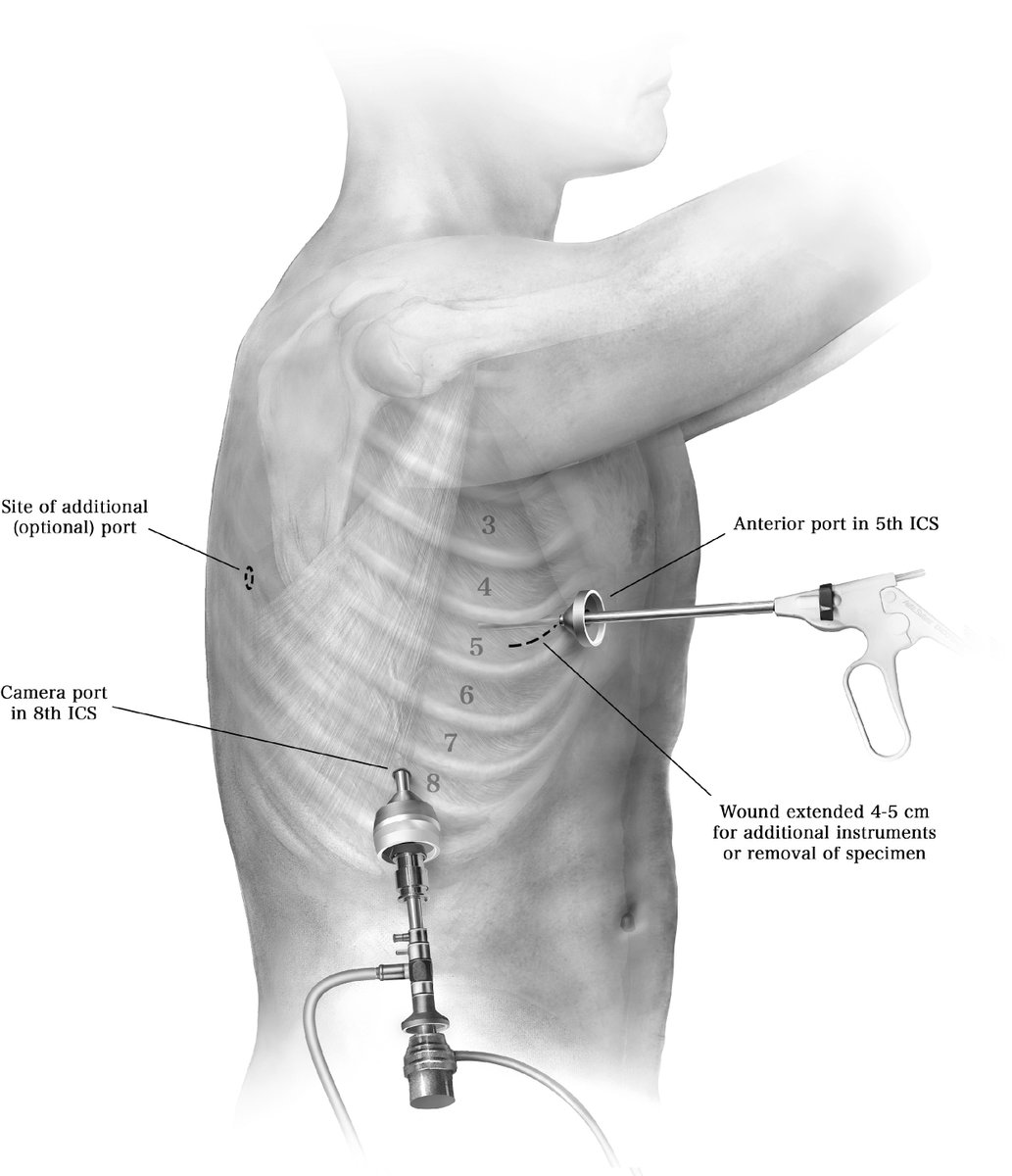
![[Excerpt]: Following port placement, the lung is mobilized away from the chest wall tumor. Any dense adhesions to the parietal pleura are taken down cautiously with blunt dissection to fully visualize the width of the chest wall tumor or extent of chest wall invasion. For resection of primary chest wall tumors, unless the adherent lung is clearly only innocently adherent (with filmy adhesions), a small wedge resection of lung should be included to avoid the risk of violating the tumor and spreading tumor into the pleural space. Once the lung is adequately mobilized, circumferential marginal excision of parietal pleura around the tumor is scored using electrocautery. Adjacent areas along the chest wall are also inspected for presence of any additional lesions. Once the parietal pleura is incised circumferentially, the underlying ribs are exposed. Most often, the ribs are exposed from the most superior border to the furthest inferior border and circumferentially to facilitate resection.](https://venexa.site/media/FctW9OAXkAAftZR.jpg)
ALT [Excerpt]: Following port placement, the lung is mobilized away from the chest wall tumor. Any dense adhesions to the parietal pleura are taken down cautiously with blunt dissection to fully visualize the width of the chest wall tumor or extent of chest wall invasion. For resection of primary chest wall tumors, unless the adherent lung is clearly only innocently adherent (with filmy adhesions), a small wedge resection of lung should be included to avoid the risk of violating the tumor and spreading tumor into the pleural space. Once the lung is adequately mobilized, circumferential marginal excision of parietal pleura around the tumor is scored using electrocautery. Adjacent areas along the chest wall are also inspected for presence of any additional lesions. Once the parietal pleura is incised circumferentially, the underlying ribs are exposed. Most often, the ribs are exposed from the most superior border to the furthest inferior border and circumferentially to facilitate resection.
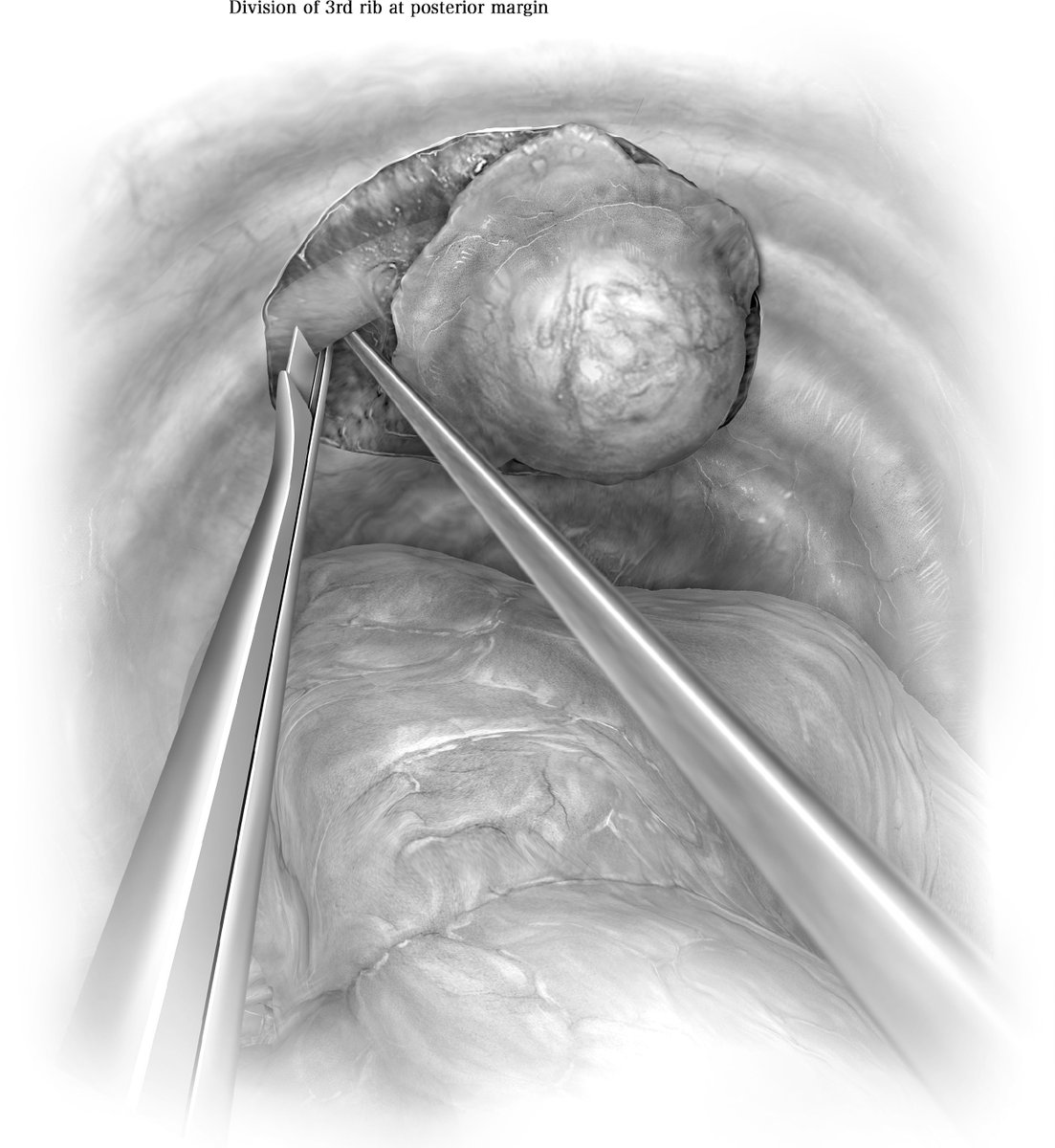
ALT Once the ribs are exposed, the posterior border of the ribs are divided using various instruments such as the rib cutter, long peapod intervertebral disc rongeur, long-handled rib shears (Giertz rib shears) or endoscopic osteotomes (Table 1). Since cutting the posterior rib attachment can be tedious because of increased depth and proximity of multiple bony elements, which may make insertion of bone cutting forceps difficult, an extended length 4 mm burr on a high-speed drill could be useful. If the ribs are adjacent to the sternal border, the costovertebral joints can be disarticulated if needed with an osteotome, allowing thoracoscopic visualization and control of vessels and nerves sequentially. For chest wall tumors near the utility incision, endoscopic osteotomes can be used since they have the most perpendicular angle with the ribs.
