
474 Photos and videos








Mechanical Life Support retweeted

Jan 5
Pleased to share !!!
heart.bmj.com/content/early/…
4
10
1,363
Mechanical Life Support retweeted

19 Dec 2025
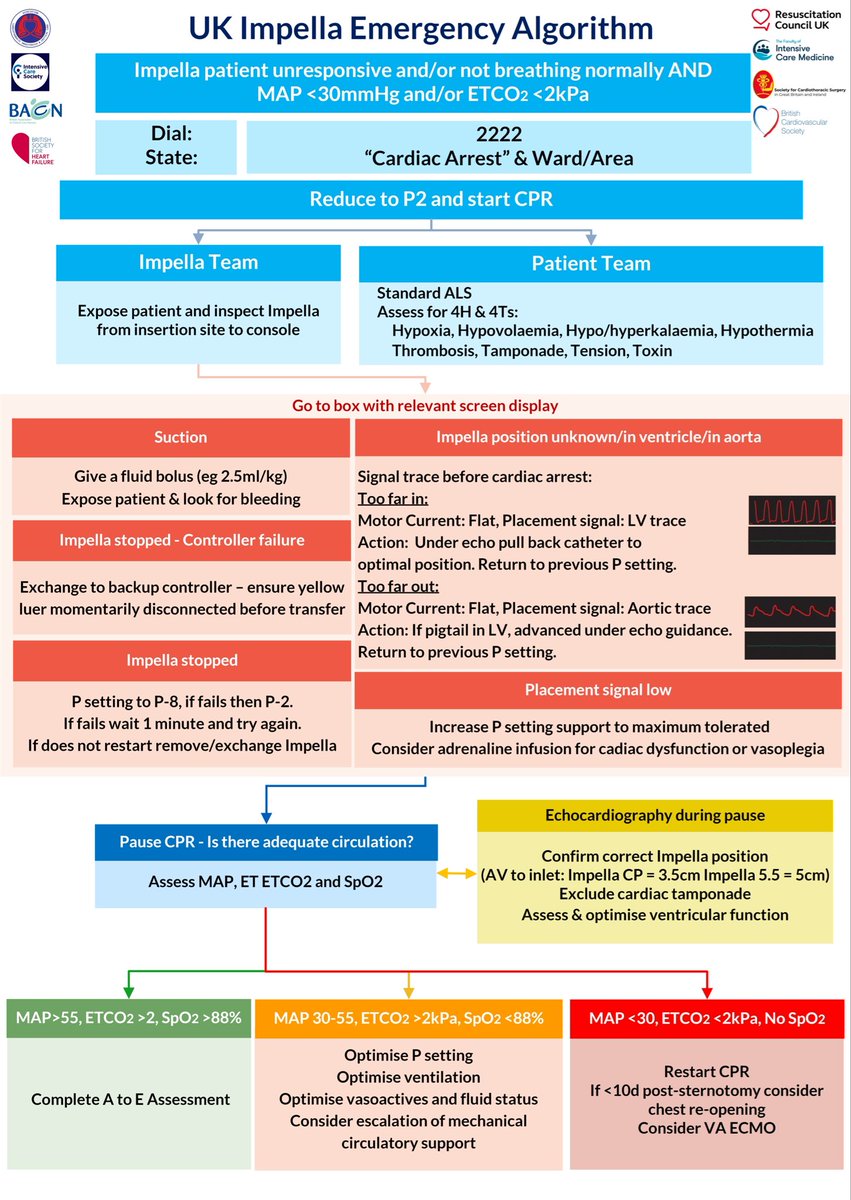
UK multisociety consensus statement on the emergency management and resuscitation of patients with left-sided Impella support
🫀Recognition of cardiac arrest
🏥 Team structure
🕵️ Early troubleshooting
heart.bmj.com/content/early/…
1
8
29
2,700
Mechanical Life Support retweeted
15 Nov 2025
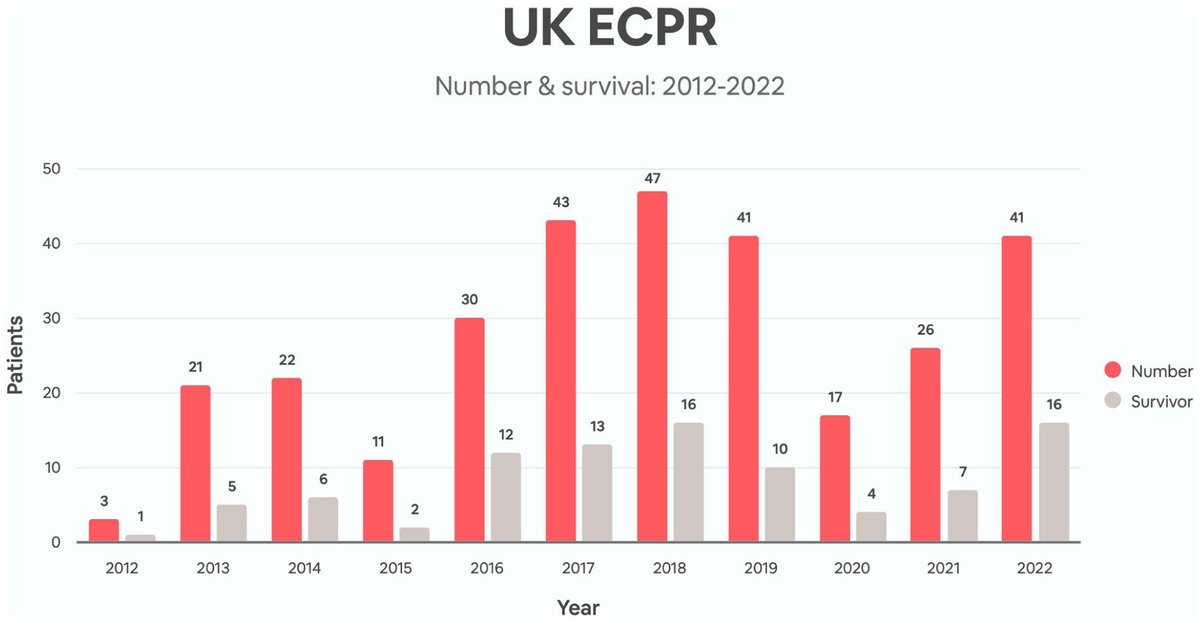
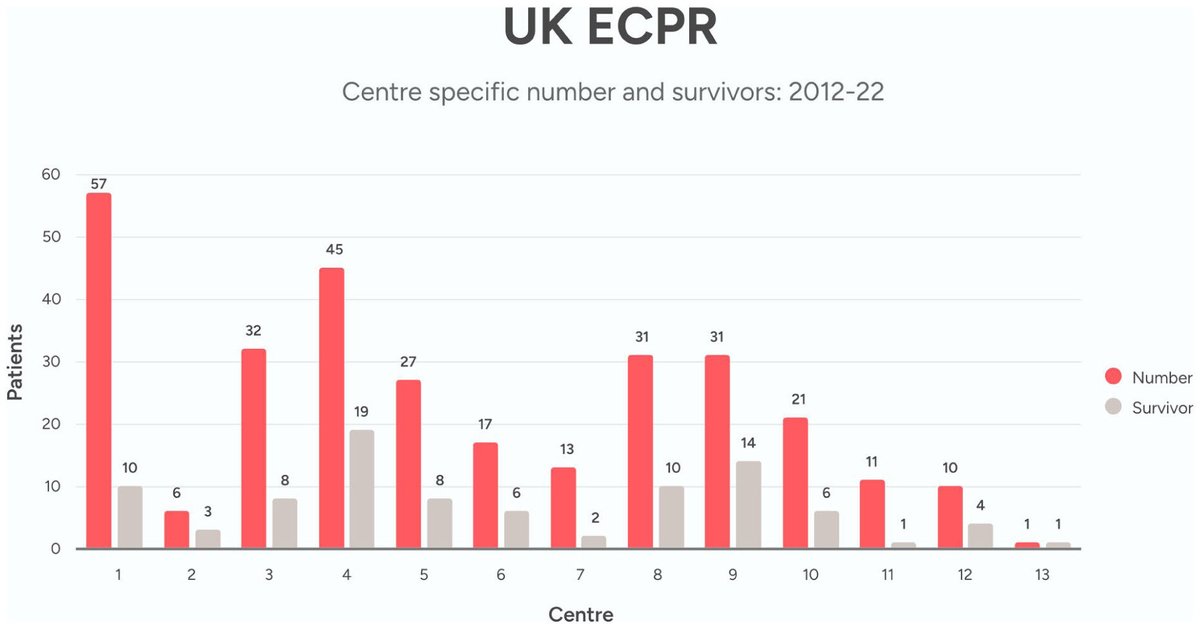
🇬🇧 UK VA ECMO and ECPR data
📆 2012-22
🏥 All 13 centres
2117 VA runs, 45.5% survival
302 ECPR runs, 30.5% survival
journals.sagepub.com/doi/10.…


3
19
53
7,035

21 Oct 2025
RT @ELSOOrg: ◾️In Memoriam of Robert H. Bartlett, MD 1939-2025
Without Dr. Bartlett, there is no ECMO: he saved more than 100,000 patients…
211
Mechanical Life Support retweeted

3 Oct 2025
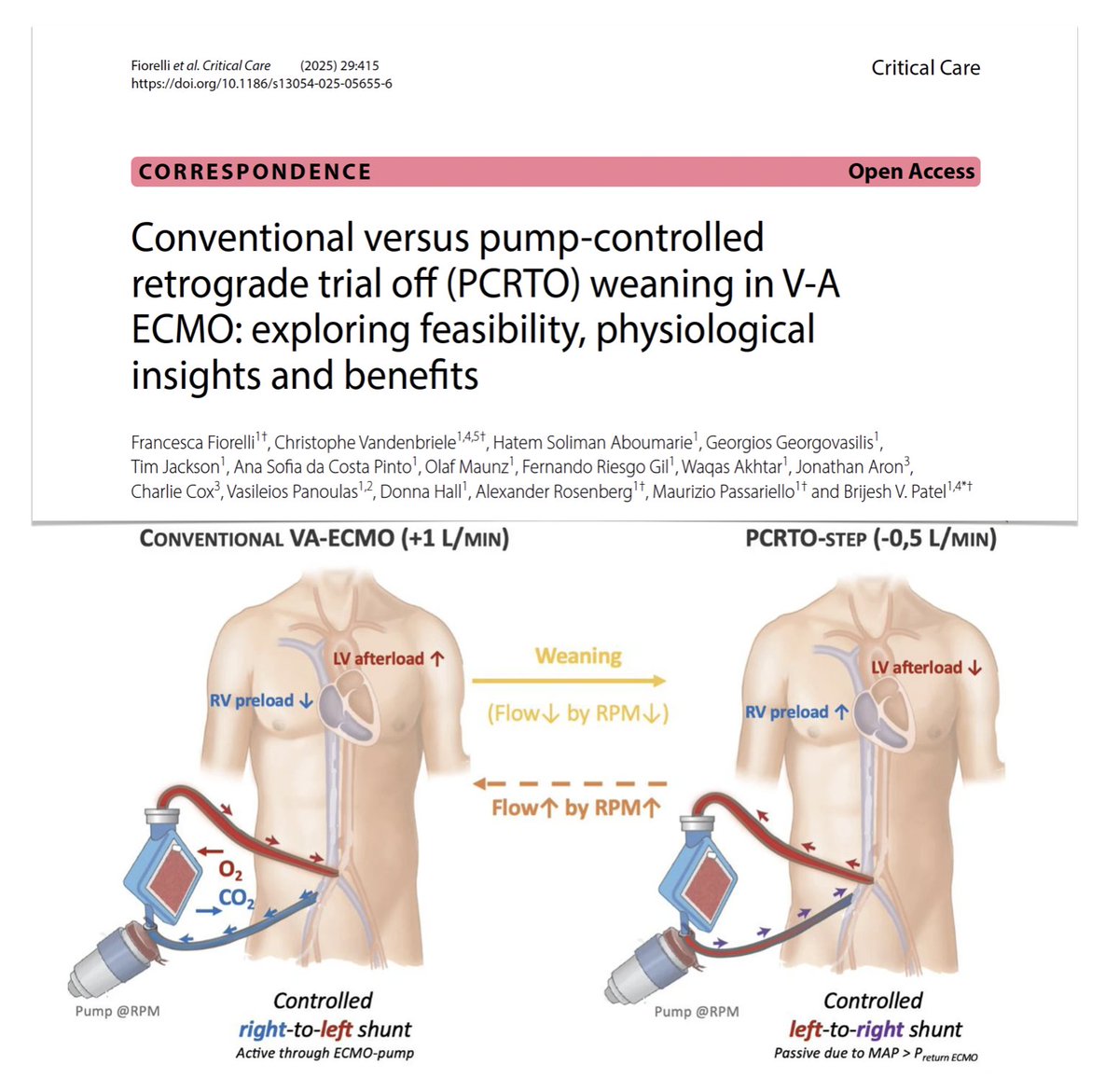
Weaning from VA #ECMO: which approach best reflects true cardiopulmonary reserve??
🔄 PCRTO: retrograde flow through pump, creating controlled VA shunt mimicking native physiology (with regular #POCUS invasive PAC monitoring), challenging RV reducing LV afterload enabling assessment of native lung function
🔍 pilot study: pump-controlled retrograde trial off feasibility, safety, physiological insights vs conventional weaning (reducing EBF to around 1 LPM, leaving residual RV unloading/LV afterload)
🫀 criteria for readiness-to-wean: resolution of underlying cause of CS, evidence of improving renal/hepatic perfusion, lactate < 2 mmol/L, MAP > 60 mmHg, pulse pressure > 15 mmHg, improving LVOT VTI, absence of severe mitral or tricuspid regurgitation
PCRTO appeared feasible, safe, informative complement to conventional weaning. In scenarios with advanced cardiac disease/borderline cases, its loading challenge added relevant information that impacted decision-making on short and long-term strategies ie
- unmasking RV failure, biventricular compromise, respiratory deterioration prompting additional optimization
- unmasking underlying defects enabling pre-explant repair
- confirming stable haemodynamics/pulmonary function supporting safe weaning, avoiding premature escalation to durable #MCS
@Crit_Care
🔓 rdcu.be/eJf91
1
36
138
9,735
Mechanical Life Support retweeted
6 Oct 2025
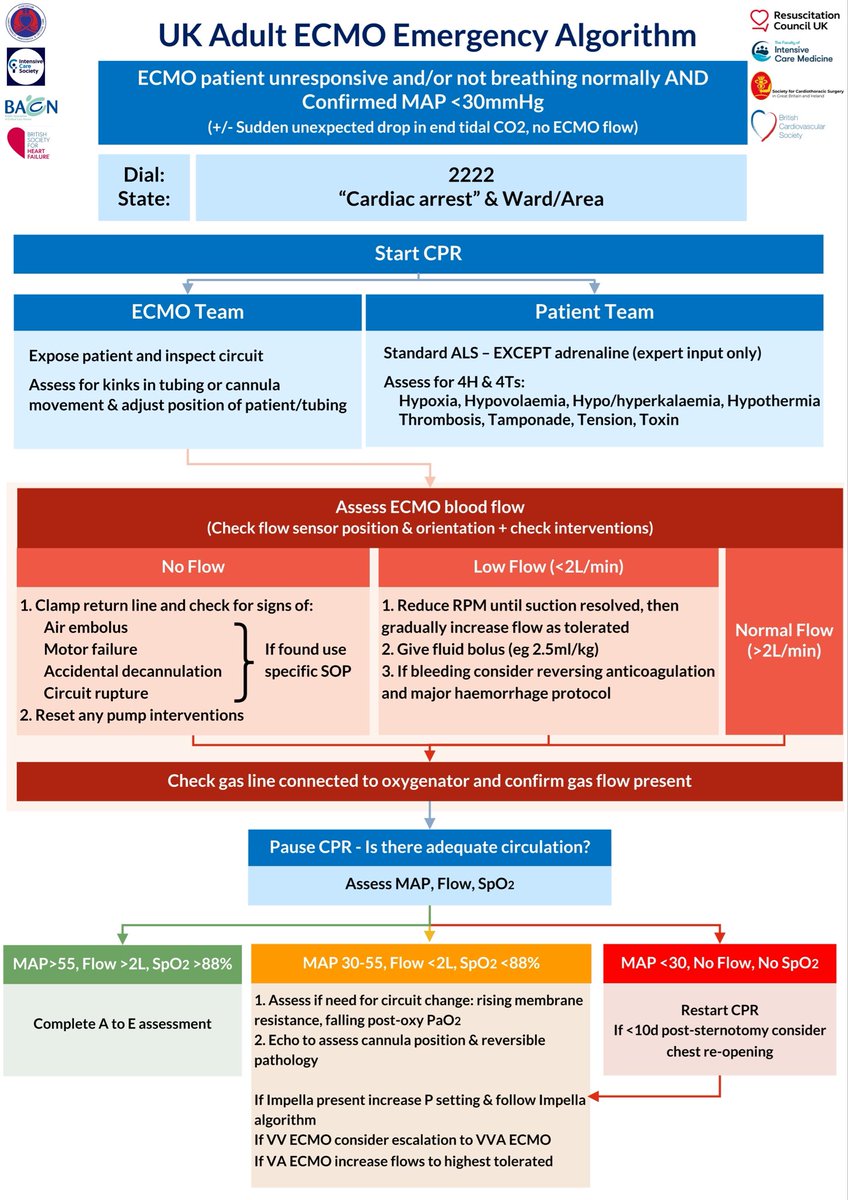
British societies guideline on management of emergencies in patients on ECMO
🫀Recognition of cardiac arrest
🏥 Team structure
🕵️ Early troubleshooting
@BritishCardioSo @FICMNews @ICS_updates @BACCNUK @SCTSUK @BSHeartFailure @ResusCouncilUK @ACTACCUK
link.springer.com/article/10…
4
31
95
9,757
Mechanical Life Support retweeted

23 Sep 2025
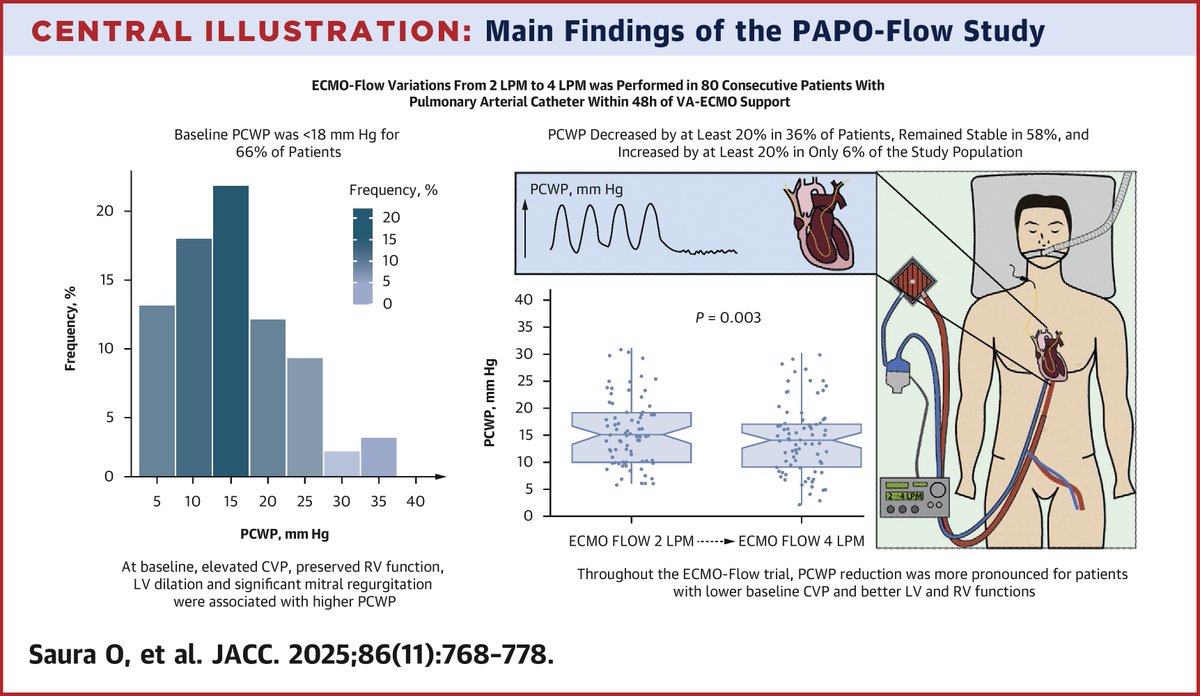
📰 Increasing VA-ECMO Flow Rarely Raises PCWP in Patients With Cardiogenic Shock
Read the journal scan for more ➡️ bit.ly/428CO8H
#JACC #HeartFailure
1
13
33
8,294
Mechanical Life Support retweeted
18 Jul 2025
2025 @ICU_Harefield
Summer Legends 🎸🍗🍦🍹
ECPR 🏆


1
3
6
857
10 Jul 2025
Summer ☀️ @MLSCourse at Harefield
Over 1000 trained at dedicated resuscitation courses for LVAD, Impella and ECMO!
14
754
Mechanical Life Support retweeted

📣Review Sharing:
🧾Extracorporeal Cardiopulmonary Resuscitation: Reviewing the Evidence and Exploring Its Equitable Implementation in the UK National Health Service
👩🔬@DrWaqasAkhtar, Nicholas A Barrett @GSTTnhs
💡Full Text: magonlinelibrary.com/doi/ful…
#ECPR #ECMO #resuscitation
4
8
755
Mechanical Life Support retweeted

13 Jun 2025
🫀 Here’s Case Two from our Cardiac Mass Series—'How well do you know cardiac masses?' 🧐
Watch the video till the end, test your skills, and drop your diagnosis below. ⬇️
Think you’ve cracked it? Find out in the next video! 🎥
#CardioTwitter #EchoChallenge #FOAMed #MedicalMystery
5
12
1,323
Mechanical Life Support retweeted

21 Jun 2025
1/We should consider the additive benefits of #GDMT during MCS for #Cardshock. Recently, we looked at the effect of implementing a protocol for aggressive GDMT uptitration during @jjmt_heartrecov Impella support. There is a free link (only 50 first) to the publication in the end
3
19
53
11,287

Great day seeing friends and learning about LVAD, impella, Ecmo with @MLSCourse at @RBandH with @DrWaqasAkhtar #MLS #MCS #ECMO #ECLS highly recommend the MLS course

1
4
19
1,560
Mechanical Life Support retweeted

8 May 2025
Meet Emanuele, Harefield Hospital's lead nurse for critical care education and workforce, and critical care associate lecturer.
Find out more about his role and why he chose to specialise in mechanical life support in critical care.
Read Emanuele's Q&A: rbht.nhs.uk/careers/what-our…

ALT Emanuele against a black background. He is wearing a nurse uniform with a purple lanyard around his neck.
1
12
1,011
Mechanical Life Support retweeted

6 May 2025
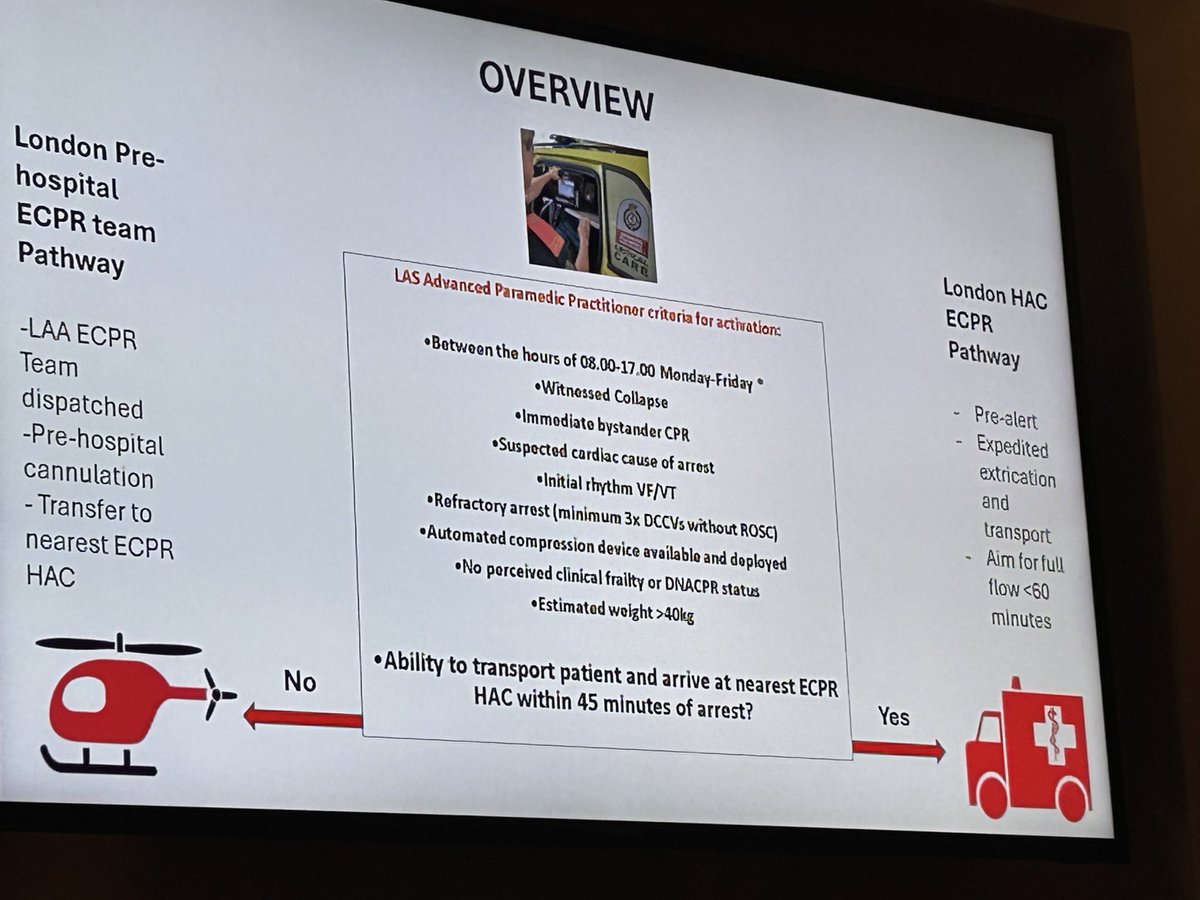
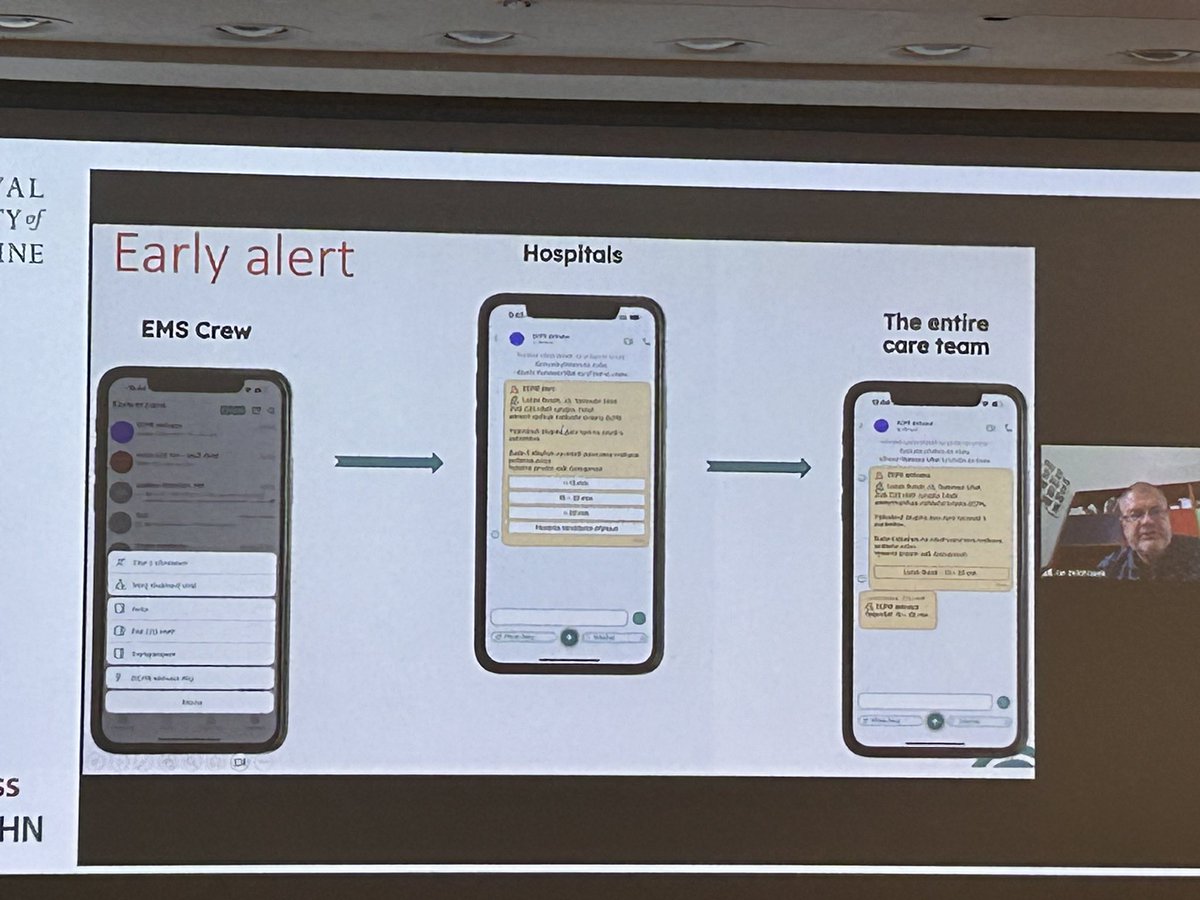
For the first time ever in the UK, we are bringing ECMO to the streets of London, offering hope to patients in cardiac arrest.
londonsairambulance.org.uk/n…


8
64
353
44,720
Mechanical Life Support retweeted

25 Apr 2025
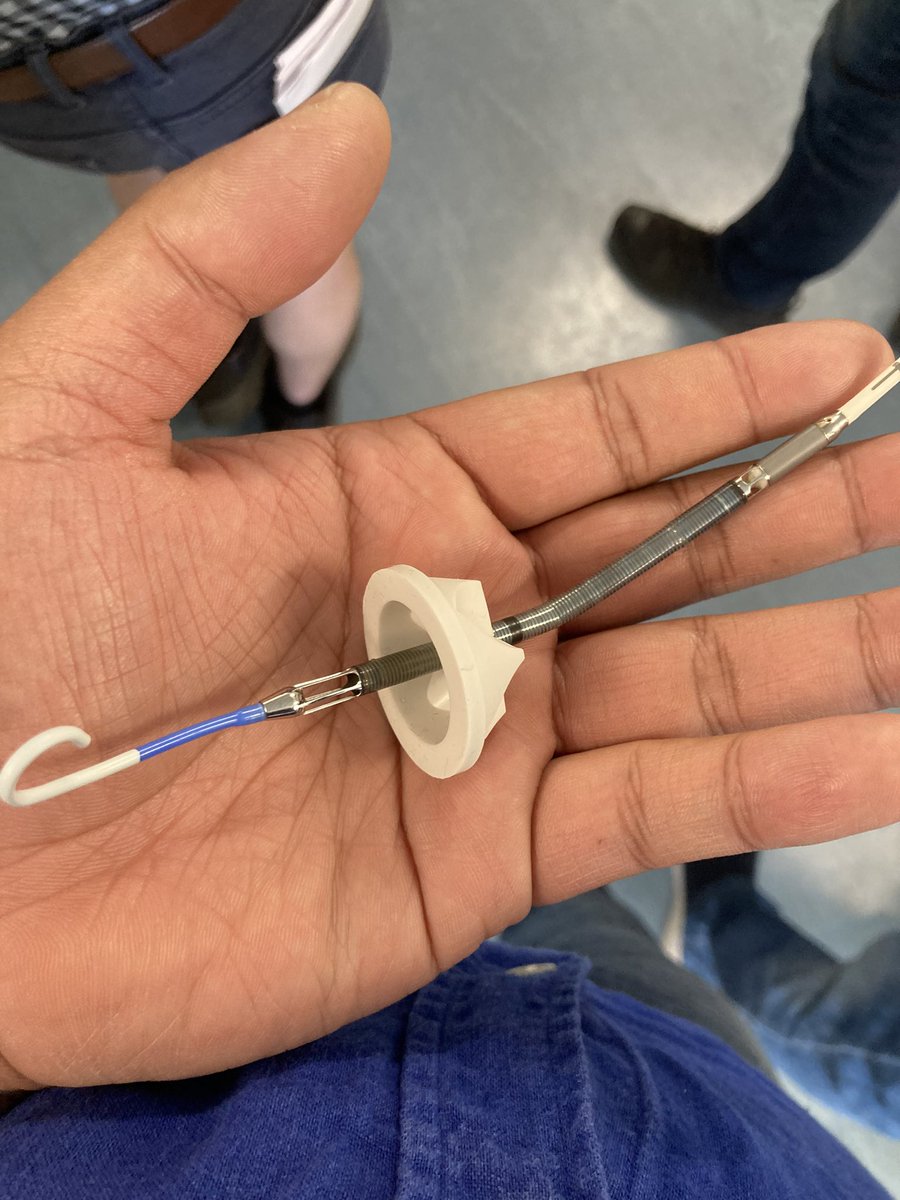
Congratulations to @EduardArgudo and the @vallhebron #ECPR team for winning the @EuroELSO cannulation cup.
I was surprised by the floppy wires but impressed with their skill.
Floppy vs stiff wire for ECPR?
39%
Floppy
42%
Stiff
19%
Whatever’s in the pack
36 votes • Final results
2
4
11
1,445
25 Apr 2025
The 2025 @EuroELSO cannulation cup winners are Barcelona!
@ECMOHUVH @EduardArgudo @mariamtnezm
Thank you to all the teams for sharing their experience in cannulation and ECPR teamwork!



5
8
30
3,405
24 Apr 2025
Come see Milan compete at the @EuroELSO Cannulation Cup 2025 in 15minutes central hall!
@SRAnesthesiaICU @tscquizzato @pacoitaly
3
16
1,202
19 Apr 2025
Hope to see you @EuroELSO for the 2025 Cannulation Cup!
Additional MLS Advanced course dates just released for 2025 at Harefield Hospital: mls.training/programme
1
5
551
Mechanical Life Support retweeted

10 Mar 2025
Interested in ICU management of heart and lung transplants, LVADs, cardiogenic shock and all forms of short term mechanical circulatory support (ECMO, impella, BiVAD)? - applications open for senior clinical fellow posts at Harefield Hospital ICU:
2
10
38
4,470