
Founder/CEO Nutritional Analytics. Specialize in Mineral Balancing, Hair Tissue Mineral Analysis Interpretation & Metals Toxicology.
Joined October 2023
- Tweets 8,844
- Following 687
- Followers 11,137
- Likes 81,946
1,403 Photos and videos






Clark Engelbert retweeted

14 Jun 2025
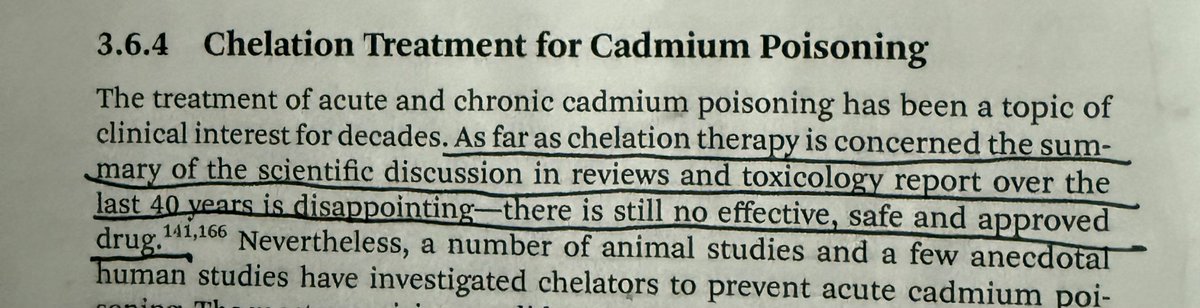
Daily reminder that despite decades of research, there is no known chelating agent for cadmium - the most toxic heavy metal.
However, I now have close to a dozen cases of clients eliminating cadmium on mineral balancing.
With this case study being the most dramatic one.
22 Apr 2025

𝗠𝗜𝗡𝗘𝗥𝗔𝗟 𝗕𝗔𝗟𝗔𝗡𝗖𝗜𝗡𝗚 𝗖𝗔𝗦𝗘 𝗦𝗧𝗨𝗗𝗬 𝗜𝗡 𝗖𝗔𝗗𝗠𝗜𝗨𝗠 𝗘𝗟𝗜𝗠𝗜𝗡𝗔𝗧𝗜𝗢𝗡 (& 𝗔𝗟𝗨𝗠𝗜𝗡𝗨𝗠):
𝙃𝙤𝙬 𝙈𝙞𝙣𝙚𝙧𝙖𝙡 𝘽𝙖𝙡𝙖𝙣𝙘𝙞𝙣𝙜 𝙃𝙚𝙖𝙡𝙚𝙙 𝘾𝙚𝙣𝙩𝙧𝙖𝙡 𝙎𝙡𝙚𝙚𝙥 𝘼𝙥𝙣𝙚𝙖 𝙖𝙣𝙙 𝙇𝙤𝙬 𝙁𝙚𝙧𝙧𝙞𝙩𝙞𝙣 𝙞𝙣 𝘼𝙣 𝙄𝙣𝙛𝙖𝙣𝙩
A thread 🧵

13
16
212
14,985
Clark Engelbert retweeted

Jun 14
7/
You'll observe that as heavy metals in a population rise, sin rises with it. Faith and church attendance decline.
This is the story of Christendom since the advent of the industrial revolution.
How do these chemicals...
1
1
6
430
Clark Engelbert retweeted
25 Nov 2025
This interesting scenario plays out much more than you might think.
So then the question becomes what does one do with zinc in this situation?
The obvious answer would be to withhold the zinc supplement temporarily as one works on balancing the sodium/potassium ratio.
But in mineral balancing the answer is rarely ever so clear cut.
Zinc is needed by almost everyone today, even in those with a low sodium/potassium ratio and this is corroborated by low or extremely high (loss) zinc readings on an HTMA.
Zinc is also THE universal buffer or heavy metal antagonist. So we can use it also to antagonize the heavy metals lead, cadmium, mercury, nickel and aluminum.
To solve this conundrum we give sodium synergists at the same time as we give zinc when one has an existing low sodium/potassium ratio.
These sodium synergist include:
- copper
- manganese
- b6
- vitamin c
What’s most interesting about this scenario is that it highlights something about the zinc and copper relationship that is not well known.
Which is that while copper is a zinc antagonist broadly speaking, in certain situations or contexts, copper can be used as a zinc SYNERGIST.
Taking copper while one has a low sodium/potassium ratio helps to improve this ratio and it facilitates better zinc absorption and utilization as this occurs.
Which implies that mineral relationships are NOT static. They are dynamic and may change based on the entire mineral system shifting in one direction or another.
Zinc and Copper are not ONLY antagonistic, but also are synergistic in certain situations.
This is essence of mineral balancing and what we try to account for when we analyze a hair tissue mineral analysis.
25 Nov 2025
Few possible reasons for this:
1. Zinc is antagonistic to sodium and synergistic with potassium.
If you have an existing low sodium to potassium ratio the supplemental zinc will exacerbate this low ratio through its antagonism with sodium, making one feel worse/depressed, etc.
2. Zinc is also antagonistic to heavy metals like nickel, lead, cadmium and mercury.
If the zinc is antagonizing metals this could cause detoxification reactions from the displacement of these heavy metals, causing temporary low energy or depression.
What’s the dosage you’re taking each day?
2
3
38
4,480

Clark Engelbert retweeted
13 Jun 2025
𝗛𝗘𝗔𝗩𝗬 𝗠𝗘𝗧𝗔𝗟 𝗚𝗘𝗡𝗘 𝗜𝗡𝗧𝗘𝗥𝗔𝗖𝗧𝗜𝗢𝗡𝗦
Yesterday I had a client call with a PhD geneticist and naturally we started talking about the interaction between metals and genes.
This conversation led me to some papers I read last night, one of which was especially interesting.
Tho not for reasons you might think.
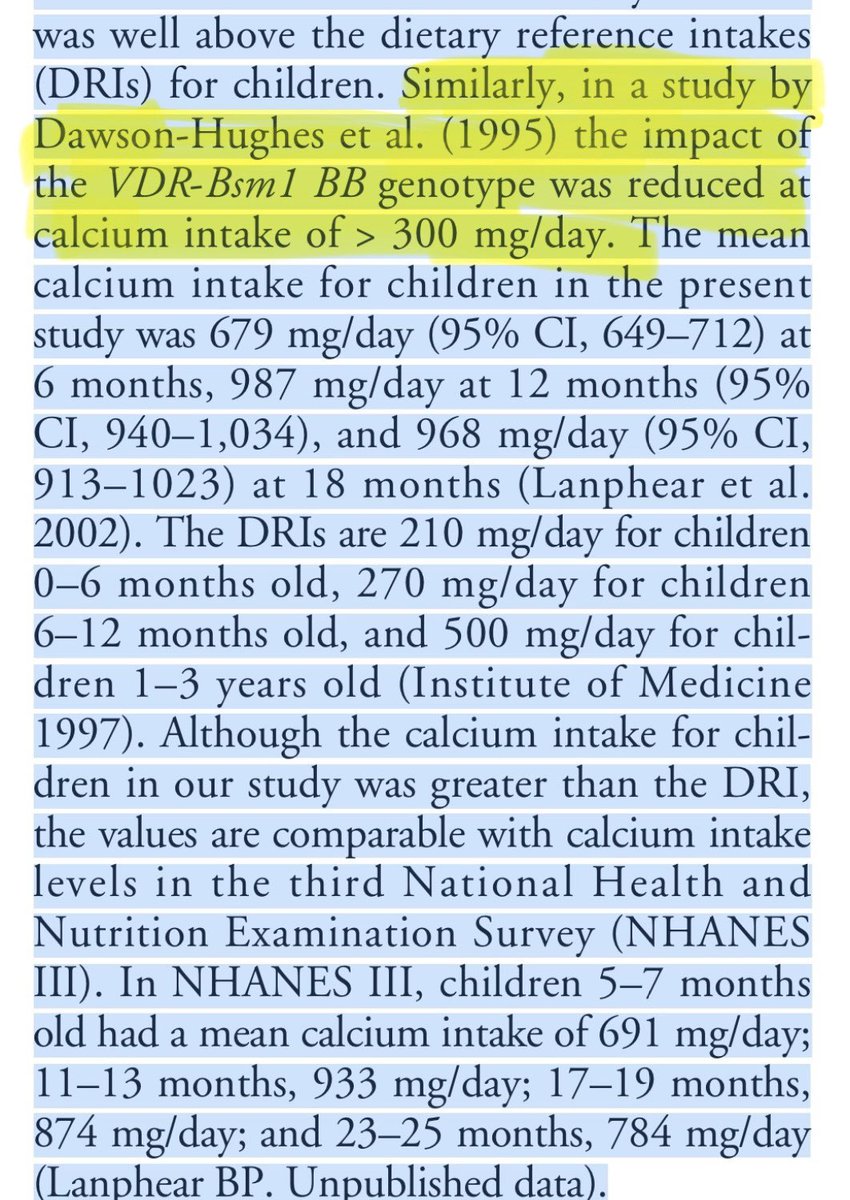
This study was looking at the relationship between blood lead and the vitamin d receptor Fok1 polymorphism.
Because of vitamin d’s very well known synergy with calcium, and because of calcium’s similarly well known antagonistic relationship with lead, researchers postulated there may be some relationship to this specific VDR polymorphism and blood lead levels in kids.
Researchers did find some interesting associations in this specific VDR polymorphism.
But that wasn’t the most interesting aspect of the study, at least to me.
The most interesting aspect of the study was the screenshot attached here, deep in the discussion section.
𝙀𝙨𝙨𝙚𝙣𝙩𝙞𝙖𝙡𝙡𝙮 𝙬𝙝𝙖𝙩 𝙩𝙝𝙞𝙨 𝙨𝙖𝙮𝙨 𝙞𝙨 𝙩𝙝𝙖𝙩 𝙞𝙣 𝙖𝙣𝙤𝙩𝙝𝙚𝙧 𝙨𝙩𝙪𝙙𝙮 𝙘𝙤𝙣𝙙𝙪𝙘𝙩𝙚𝙙 𝙗𝙮 𝘿𝙖𝙬𝙨𝙤𝙣-𝙃𝙪𝙜𝙝𝙚𝙨, 𝙩𝙝𝙖𝙩 𝙜𝙚𝙣𝙚-𝙡𝙚𝙖𝙙 𝙞𝙣𝙩𝙚𝙧𝙖𝙘𝙩𝙞𝙤𝙣𝙨 𝙤𝙣 𝙖𝙣𝙤𝙩𝙝𝙚𝙧 𝙫𝙞𝙩𝙖𝙢𝙞𝙣 𝙙 𝙧𝙚𝙘𝙚𝙥𝙩𝙤𝙧 𝙖𝙧𝙚 𝙧𝙚𝙙𝙪𝙘𝙚𝙙 𝙬𝙝𝙚𝙣 𝙘𝙖𝙡𝙘𝙞𝙪𝙢 𝙞𝙣𝙩𝙖𝙠𝙚 𝙞𝙨 𝙗𝙚𝙮𝙤𝙣𝙙 𝙖 𝙘𝙚𝙧𝙩𝙖𝙞𝙣 𝙩𝙝𝙧𝙚𝙨𝙝𝙤𝙡𝙙.
To me, what this implies is extremely important.
Which is that your mineral intake is more important than your genetic susceptibility to absorbing metals.
Let’s consider why, in the first place, researchers are looking at this particular gene polymorphism in relationship to blood lead levels.
They decided to look at this VDR polymorphism BECAUSE of vitamin d’s association with calcium - THE PRIMARY MINERAL ANTAGONIST TO LEAD.
And then we see, in another study cited here that these gene-metal interactions are overwhelmed by sufficient calcium intake.
So, the most important thing when considering your risk for heavy metal toxicity - and also how to detoxify them - is YOUR MINERALS.
I’m not saying genes don’t matter. They do.
But let’s focus on, not only what we can control (mineral intake), but also the biggest levers we can pull against your heavy metals. Which is, again, your mineral intake.
3
37
1,813
Jun 12
Libtards are so fckin evil man.
They say you’re a racist Nazi for opposing teenage girls getting randomly stabbed by Mytatagaha HbGarainaba for literally no reason at all.
TOTAL REMIGRATION of every turd worlder out of the UK, Ireland and really all of Europe if we’re being real.
This sort of thing is just not worth it.
3
42
1,622
Jun 12
1000% true.
It boggles the mind that medical professionals cannot make this (seemingly) obvious distinction.
Route of exposure for metals matters tremendously.
Ingestion exposure isn’t remotely in the same ballpark as inhalation or injection exposure to metals, as Bryce correctly points out.
To give anther example here, inhalation absorption of cadmium via cigarettes or marijuana approaches 50%, whereas ingestion via food and drink is usually around 5-15%, depending on a few variables.
With aluminum injected in vaccines there’s another effect that we might call 3rd order that is even less well accounted for by medicine than just a difference in absorption profile.
But is related to aluminum distribution to a specific tissue (ie the brain).
Which is that aluminum is in the vaccine in the first place to AMPLIFY the immune response to the antigen (measles, mumps, rubella, etc, whatever it is) so that an immune memory is created for the antigen.
Meaning aluminum is there, specifically to TRIGGER THE IMMUNE SYSTEM.
As this happens, immune cells come and grab or bind aluminum post injection.
These immune cells have preferential or special access to brain tissue when they get triggered and come and bind the aluminum.
So not only is a much higher percentage of the aluminum absorbed through injection versus ingestion, but a much higher percentage of this absorbed fraction of aluminum TARGETS THE BRAIN TISSUE SPECIFICALLY.
Which perfectly explains why some kids have such catastrophic reactions to vaccines.
Jun 12

After my first child was born the pediatrician came in to educate us on vaccines
Immediately he brings up heavy metals:
"Are you worried about the aluminum in vaccines? Because you should know your baby gets more aluminum from breast milk than they do from a vaccine"
I didn't argue, but I did do my research
A single vaccine contains between 0.125-0.85mg of aluminum
In comparison breast milk contains between 0.01-0.05mg of aluminum per liter (34oz or about 4 cups), and infants drink between 16-32oz of breast milk per day
So if we assume the lowest intake of milk and lowest aluminum level in that milk it would take about 25 days to reach the same 0.125mg in some vaccines
If we assume the highest content in breast milk and that the baby drinks a full 32oz per day it takes more like 3-17 days to reach the level in a single dose of a vaccine (0.125-0.85)
Sounds logical, right?
The problem is the pediatrician was completely ignoring an important point, BIOAVAILABILITY
Aluminum from breast milk has less than a 1% bioavailability, meanwhile the bioavailability of aluminum in vaccines approaches 100% absorption
This means we need to take the number above and multiply it by 100x, it would take a year of 1 liter daily breast milk to even surpass the lowest aluminum content in vaccines, and with the current schedule MULTIPLE are stacked together in the first few days of life
This is the kind of thing that frustrates me endlessly, I believe people should weigh risk/benefit and choose what they believe is best for their child, but twisting the facts to give a blatantly false impression ("you're giving your child more aluminum than a vaccine") is pure fear based manipulation
There are examples of this being done to women and parents every single day in the medical system
5
55
3,432
Clark Engelbert retweeted
12 Jun 2025
Mercury is geochemically cycled through three primary point sources:
- Volcanic activity
- Gold mining
- Combustion processes in the 3rd world
What this means is that these activities spew mercury into the air at very high rates.
Mercury starts out as elemental mercury from these point sources.
As it is spewed into the atmosphere it is changed into inorganic mercury where it can hover for up to a year before raining down onto some faraway location and/or the oceans.
This is WHY so much mercury is in the oceans.
It’s in the air in the first place to a significant degree.
Then, once in the oceans, fungal micro-organisms methylate the inorganic mercury into its most toxic and famous form, methylmercury.
And then methylmercury moves its way up the food chain through biomagnification and humans eat bigger fish loaded with this toxic form of mercury.
And keep in mind, methylmercury is absorbed with the highest efficiency of any of the other forms of mercury- usually 80-100% of it.
Once in the body, methylmercury crosses the blood brain barrier via neutral amino acid transporters that normally allows cysteine across the blood brain barrier through a process called molecular mimicry.
Once in the brain, mercury targets the cerebellum with the highest avidity and this can then cause balance, visual and neurological problems in the person.
4
26
1,666
Jun 12
This is what the copper tards sound like when they tell everyone to just indiscriminately take 50 milligrams of copper every day.

10
1
42
6,050
Jun 11
This fucking retard, among many others on this app, confuse acute toxicity and chronic toxicity.
Chronic toxicity is harder to induce because the body down-regulates absorption pathways to counter the chronic excess one is getting from this amount of supplementation on a daily basis.
It’s called ADAPTATION to a stressor.
We have these mechanisms, even for heavy metals, and it’s known we can go on for years with subacute metal toxicity before things start to go wrong.
And the clinical picture is quite confusing at this point because chronic toxicity states are much less well characterized and can be confounded by other toxicants in the system.
So they think because a high dose doesn’t acutely poison them immediately that chronic toxicity can’t be induced.
Toxicity exists on a spectrum.
But truly, it’s only a matter of time before people like this overwhelm the body’s capacity to excrete copper or whatever they’re megadosing and they give themselves liver failure or something else happens.
Apr 9

The lethal dose of salt and copper sulfate is the same.
About 12 teaspoons.
I have been taking 40 mg of copper daily for months now and haven't experienced ANY decline in health.
Only upsides.
But some people are scared of 1 mg copper from food.
1
1
48
3,649
Clark Engelbert retweeted

Jun 10
I think it was @MetalsBrah on here who said potassium is speed sodium is power and it really does look like that from an outside view when I look at their behaviour and business acumen
1
40
2,024

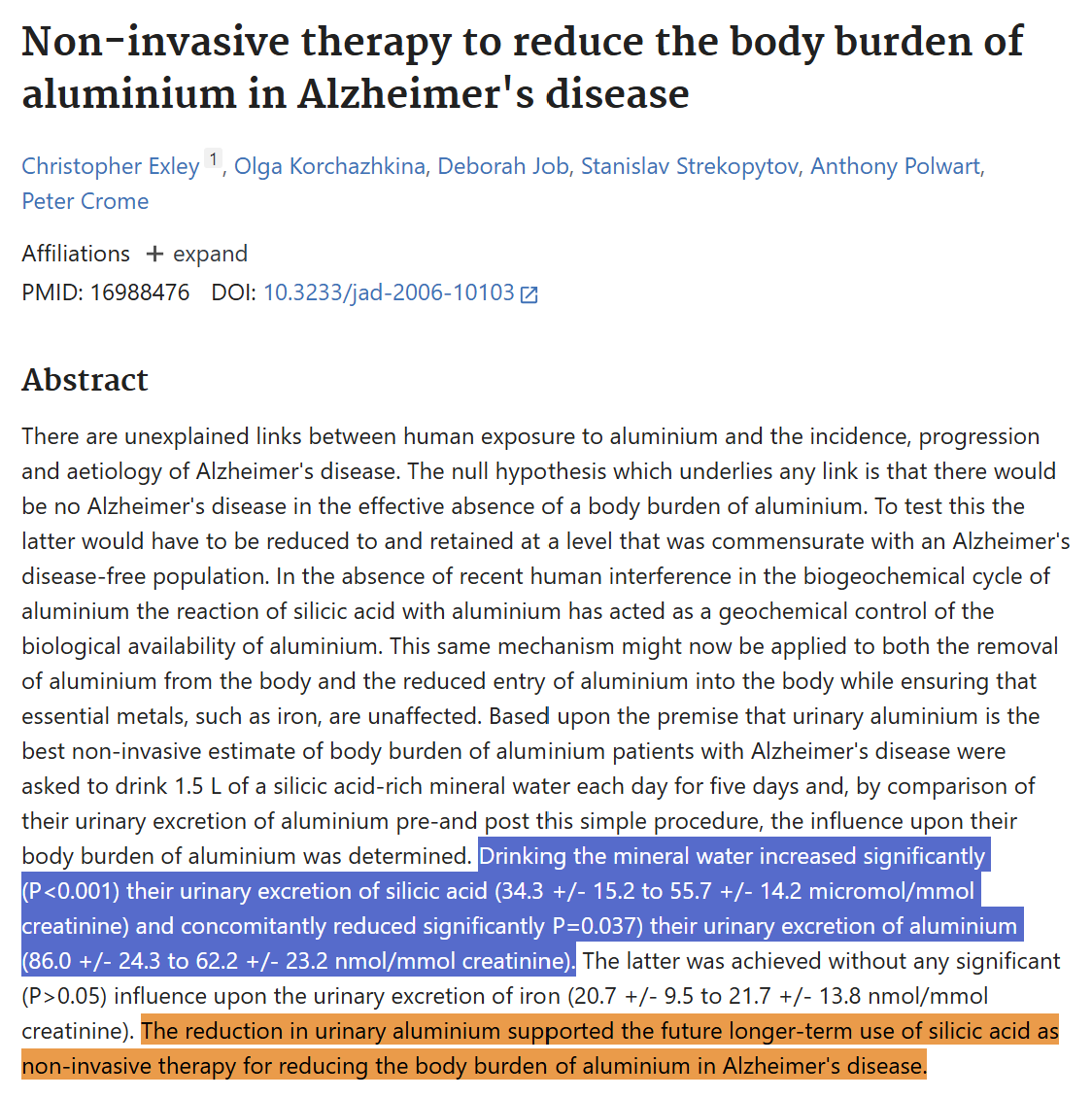
Silica in mineral water has been shown to bind aluminum and help remove it from the body.
In this 5 day study:
10 patients with Alzheimer's disease drank 1.5 liters of Volvic water per day, which contained 31.7 mg of silica per liter.
That provided about 48 mg of silica per day, or about 238 mg of silica over the course of the study.
Results:
After 5 days of drinking the silica rich water, average urinary aluminum measurements decreased from 86.0 to 62.2 nmol/mmol creatinine.
The researchers interpreted these findings as evidence that silica helped reduce the body's aluminum burden.
Ty @MetalsBrah for introducing me to the work of Christopher Exley.
5
19
175
7,107
Jun 10
𝗛𝗧𝗠𝗔 𝗜𝗦 𝗨𝗦𝗘𝗟𝗘𝗦𝗦 𝗪𝗜𝗧𝗛𝗢𝗨𝗧 𝗠𝗜𝗡𝗘𝗥𝗔𝗟 𝗕𝗔𝗟𝗔𝗡𝗖𝗜𝗡𝗚
There are countless practitioners out there these days who use hair tissue mineral analysis testing and what they get out of the HTMA is precisely ZERO.
The truth of the matter is, using this diagnostic testing outside the context of mineral balancing is almost completely useless.
I see practitioners post to social media each day talking about how they “use HTMA” but they either post awful results or none at all with their clients.
This is because they use HTMA decoupled from mineral balancing.
This framework of mineral balancing allows us to interpret and use the HTMA correctly towards the end of 𝗕𝗔𝗟𝗔𝗡𝗖𝗜𝗡𝗚 𝗧𝗛𝗘 𝗘𝗡𝗧𝗜𝗥𝗘 𝗠𝗜𝗡𝗘𝗥𝗔𝗟 𝗦𝗬𝗦𝗧𝗘𝗠 all at once, which massively antagonizes one’s heavy metal burden and results in detoxification that can be evidenced by doing HTMA tests in series.
Anything less than this renders this diagnostic testing useless and is probably a major reason why outside our little niche so few people take HTMA seriously.
Many are simply using it incorrectly and post about their subpar results and the outside world sees this and writes off HTMA entirely.
3
2
33
2,655
Jun 10
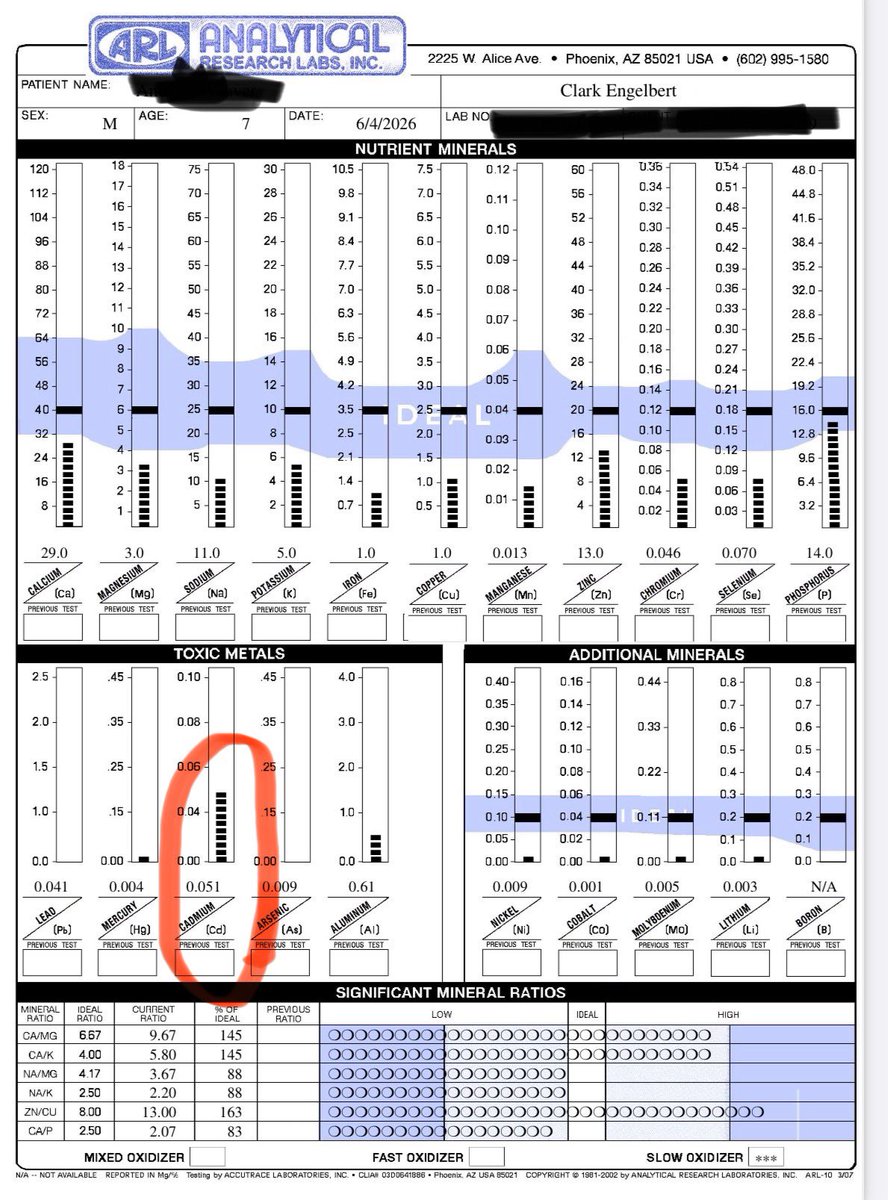
This is an interesting initial HTMA for a 7 year old boy with a diagnosis of Autism.
This is many ASD tests now I’ve seen that present initially with a high cadmium reading.
Aluminum is elevated as well, but this is far more common, especially in the ASD population.
It’s well-documented that lead and aluminum disrupt neurodevelopment, but less well-known that cadmium absolutely can as well.
Cadmium has a massive impact on zinc, especially, because of their physiochemical similarities.
For brain development, zinc is probably the most important mineral.
Other imbalances exist here and are important (low calcium, low magnesium, low zinc, 4 lows, low na/k ratio) but the high cadmium reading is likely the most relevant with respect to the ASD diagnosis.
I’m seeing more of this metal pop up in these developmentally delayed kids.
1
2
36
1,425
Clark Engelbert retweeted

Jun 10
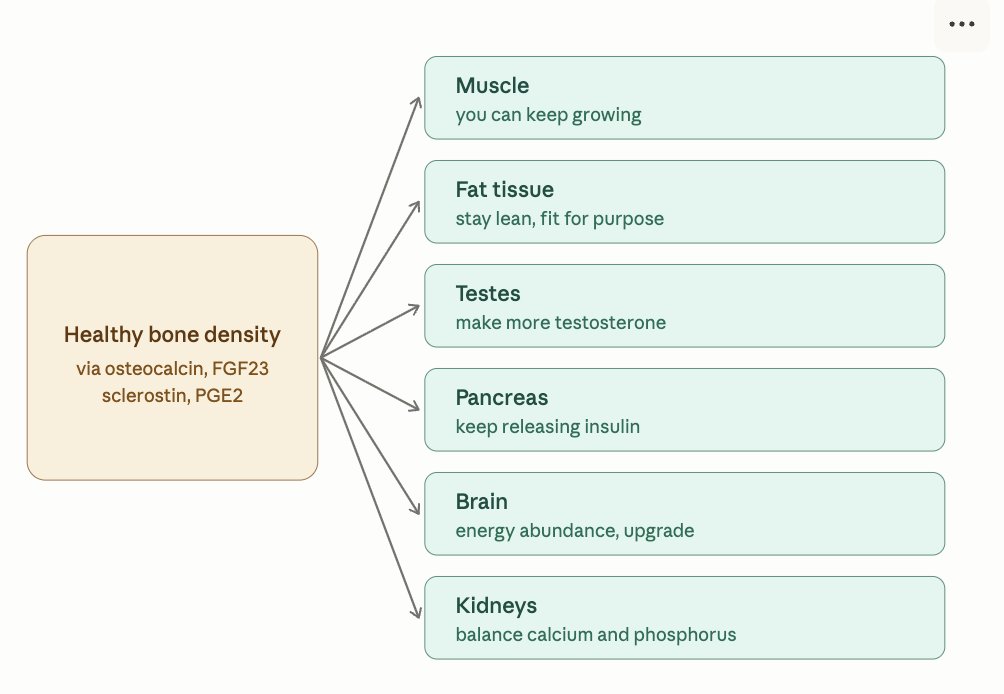
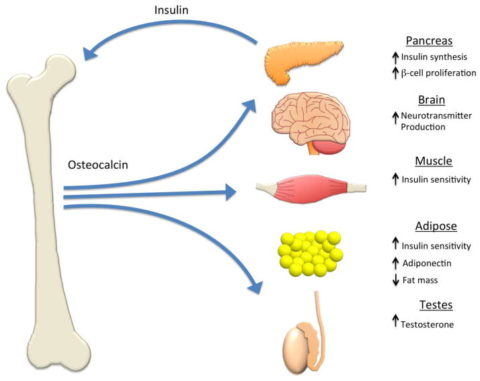
Much like fat density and muscle density — bone density is of equal importance and acts as a signal to communicate with other tissues of the body.
- Fat tissue speaks via leptin, adipokines, free fatty acids, triglycerides, cytokines, and other hormones.
- Muscle tissue speaks via myokines (irisin, IL-6, IL-15, myostatin), lactate, and prostaglandins, and indirectly through its ability to pull glucose and triglycerides out of the blood — acting as the body's largest metabolic sink in the body.
- Bone tissue speaks via osteocalcin, FGF23, sclerostin, RANKL, prostaglandins (PGE2), and cytokines — largely orchestrated by the osteocytes, which make up 90–95% of all bone cells, formed from osteoblasts.
- Fascial networks, alongside blood and lymphatic vessels, and nerves, are the wires that send these signals for communication within their biochemical and bioelectrical structures.
You can think of this as if they're all seeing if trying to achieve optimal homeostasis with one another.
If bone density is solid, then it will tell the muscle "you can keep growing," it will tell the fat tissue indirectly "let's keep you slim, but enough for your biological purpose," and it will tell the testes "you can make more testosterone to build more muscle and keep the fat slim."
It will also tell the pancreas "you can keep releasing insulin, we are metabolically ready to burn glucose and build proteins," and it will even tell the brain "we are in energy abundance down here, you can leverage neurogenesis, neurotransmitters, and neuroplasticity to build up/upgrade the nervous system."
This is how leptin and insulin talk to the brain via the hypothalamic-pituitary axis', which communicates to the associated glands to release hormones like thyroid, cortisol, testosterone, estrogen, DHEA, prolactin, adrenaline, and more.
Jun 10

Bone health is seriously under-rated in comparison to body fat and muscle density.
Your fat tissue speaks to other tissues via leptin and other cytokines. Your muscle speaks to other tissues via myokines, lactate, and indirectly via controlling blood triglycerides/glucose.
And your bone matrix speaks to your body via osteocalcin, FGF23, prostaglandins, nitric oxide, Mg-ATP, mechanotransduction signals, RANKL, and other cytokines.
Bone cells (eg., osteocytes, osteoblasts) release osteocalcin (requires vitamin A D for synthesis, alongside K2 for carboxylation) which increases testosterone and insulin driving anabolism in muscle and optimal body fat. This compound also directly induces myogenesis, and is neuroprotective.
Your bone tissue is saying "hey guys, I'm the structure and I'm currently strong, so let's build everything up."
These cells also releases FGF23 to balance the calcium/phosphorus ratio.
If you have poor calcification in your bones/teeth, you probably have excessive calcification in your soft tissues where you don't want it. This has its own subset of negative consequences like poor blood flow, detoxification, hypoxia, and severe disease states like cardiovascular events, kidney disease, and even hair loss.
Your bone cells also releases beneficial prostaglandins, nitric oxide, and ATP to further drive bone anabolism and remodelling.
Your bone matrix contains mechanosensory receptors like PIEZO1 and integrins that drive microfractures — much like microtears within muscle — to drive that anabolism. This is via all forms of movement like resistance training, running, jumping, etc.
You need an array of nutrients to support all of this:
- Balanced calcium/phosphorus
- Vitamin A, D, K2, alongside proper bile/lymphatic flow
- Magnesium, zinc, and iron
- Balanced arachadonic acid and DHA/EPA intake
- Carbon dioxide
- Cofactors for nitric oxide/NOS (arginine, oxygen, etc.)
- B vitamins for energy metabolism
Excessive cortisol and PTH lead to excessive bone resorption (breakdown) that exceeds formation. Testosterone, estrogen (in balance), and IGF-1 stimulate bone formation. Theoretically, excessive estrogen may have paradoxical effects due to lowering testosterone (via aromatase), and being a subsequent hormonal byproduct of excessive oxidative stress/inflammation (which also induces bone resorption).
Don't underestimate your bone health. Muscle and fat get more attention, but bone might matter way more.

2
5
58
3,150