
Clinical Scientist (HSST) @PublicHealthW - Microbiology. Focusing on #AMR and WGS 🧬 Own opinion only. Fictional cases for education #AMStewardship #MedEd
Joined April 2022
- Tweets 2,296
- Following 777
- Followers 3,495
- Likes 6,378
516 Photos and videos






Jun 13
Oseltamivir was found to be INEFFECTIVE in reducing 90-day mortality compared with no antiviral, and had a *high probability of harm*.
Jun 11

remapcap.org/oseltamivir-cli… With millions of cases of severe flu worldwide annually, this result should have been reached back in the 1990s. Oseltamivir should be withdrawn from hospital formularies. 2/4
1
7
26
6,174
Jun 12
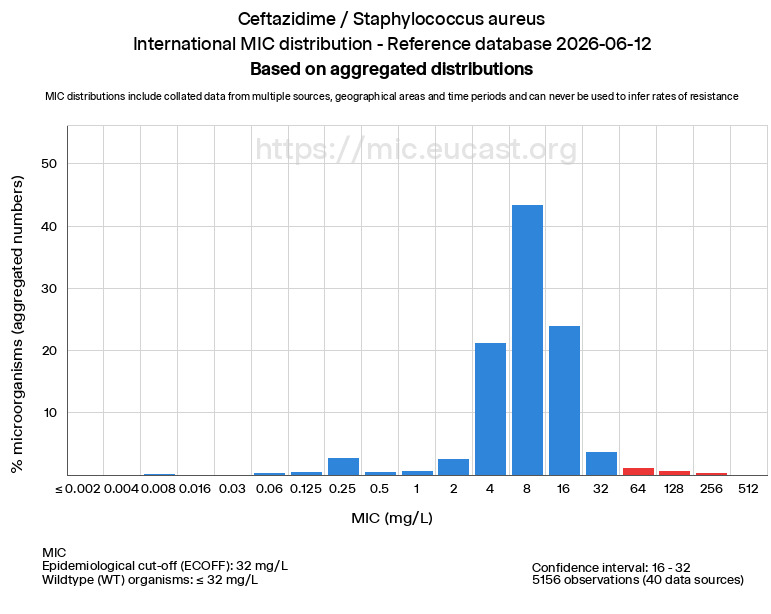
Please don't use ceftazidime to treat staph aureus - even if it is an MSSA.
Jun 11
A patient with an MSSA bacteraemia is put on cefazolin.
Meanwhile, a wound culture grows P. aeruginosa susceptible to ceftaz, taz, and mero.
The team want to cover both with one drug. They figure ceftaz is best-it's a cephalosporin just like cefazolin-covers both orgs right??
1
1
10
3,131
Jun 11
A patient with an MSSA bacteraemia is put on cefazolin.
Meanwhile, a wound culture grows P. aeruginosa susceptible to ceftaz, taz, and mero.
The team want to cover both with one drug. They figure ceftaz is best-it's a cephalosporin just like cefazolin-covers both orgs right??
15
1
24
13,878
Jun 12
Short answer - ceftazidime does not work well against Staph aureus!
Although active in vitro, treatment failures have been reported and so should be avoided.
Other 3rd gen cephalosporins, e.g. ceftriaxone, can be used, but cefazolin (1st gen) is usually the best option.
1
1
5
523
Jun 12
The pseudomonas, as some pointed out, may not need treating at all.
It's a common coloniser and presence in a wound does not equal infection!
However, if the team were convinced it was an infection, then high dose Taz could be an option to cover both here.
1
1
3
448
Luke Turner 🦠 retweeted

Jun 10
I’m a chemist. I need to say this - because it’s getting dangerous out there. The biggest health myth in the world isn’t about vaccines.
Or GMOs. Or fluoride.
It’s the root of all of them.
It’s called chemophobia - and it’s killing science.
Fear of “chemicals” now drives vaccine rejection, GMO bans, food hysteria, and entire political movements.
From tampons to tap water, people have been taught to fear chemistry - the very thing that keeps us alive.
Chemophobia tells us:
“Natural is good.”
“Synthetic is bad.”
That’s a lie.
Botulinum toxin is 100% natural and one of the deadliest molecules known. Aspirin is synthetic and life-saving.
We’ve gone from banning harmful substances for good reason…to banning safe, well-tested molecules for emotional reasons.
You’ve seen the slogans: “If you can’t pronounce it, don’t eat it.” “Paraben-free.” “Clean beauty.”
They sound empowering. But they’re not science - they’re marketing. And they’re making the world dumber, poorer, and sicker.
Your body doesn’t care if a molecule comes from a plant or a lab. Vitamin C is vitamin C.
Formaldehyde is formaldehyde and your body makes more of it every day than any vaccine ever could.
Dose matters. Source doesn’t.
This fear isn’t harmless.
It shapes public policy.
It blocks innovation.
It raises food prices.
It slows down cancer treatments.
Chemophobia is now mainstream and it’s costing lives. Scientists aren’t losing because we’re wrong.
We’re losing because fear spreads faster than facts. Because influencers sell fear for clicks.
Because lawyers monetize doubt. And because scientists are too tired to fight back.
So here’s my message, as a chemist and as a citizen: Learn how toxicology works.
Call out chemical fear-mongering. Support policies based on evidence, not emotion.
Chemistry isn’t the enemy. It’s the reason you have clean water, safe food, and modern medicine.
If we let fear win, we lose all of it.
173
639
1,741
37,198
Jun 4
TSST-1 is a superantigen toxin produced by certain strains of Staphylococcus aureus, and it is the primary cause of toxic shock syndrome (TSS).
👇
Jun 2
Q: Which Staphylococcus aureus toxin is responsible for toxic shock syndrome?
A. Exfoliative toxin
B. TSST-1
C. Staphylococcal enterotoxin A
D. Haemolysin
1
6
1,214
Jun 4
C. Staphylococcal enterotoxin A ❌
Causes food poisoning
Rapid-onset vomiting (within hours)
1
69
Jun 4
D. Haemolysin (α-toxin) ❌
A cytotoxin that:
- Forms pores in host cell membranes
- Leads to cell lysis (especially RBCs, platelets, and leukocytes)
52
Jun 2
Q: Which Staphylococcus aureus toxin is responsible for toxic shock syndrome?
A. Exfoliative toxin
B. TSST-1
C. Staphylococcal enterotoxin A
D. Haemolysin
5
3
26
5,949
Jun 4
Correct Answer: B. TSST-1 (Toxic Shock Syndrome Toxin-1).
TSST-1 is a superantigen toxin produced by certain strains of Staphylococcus aureus, and it is the primary cause of toxic shock syndrome (TSS).
90
Luke Turner 🦠 retweeted

Jun 2
yeah math jokes have to at least work
2
2
65
8,042
Jun 1
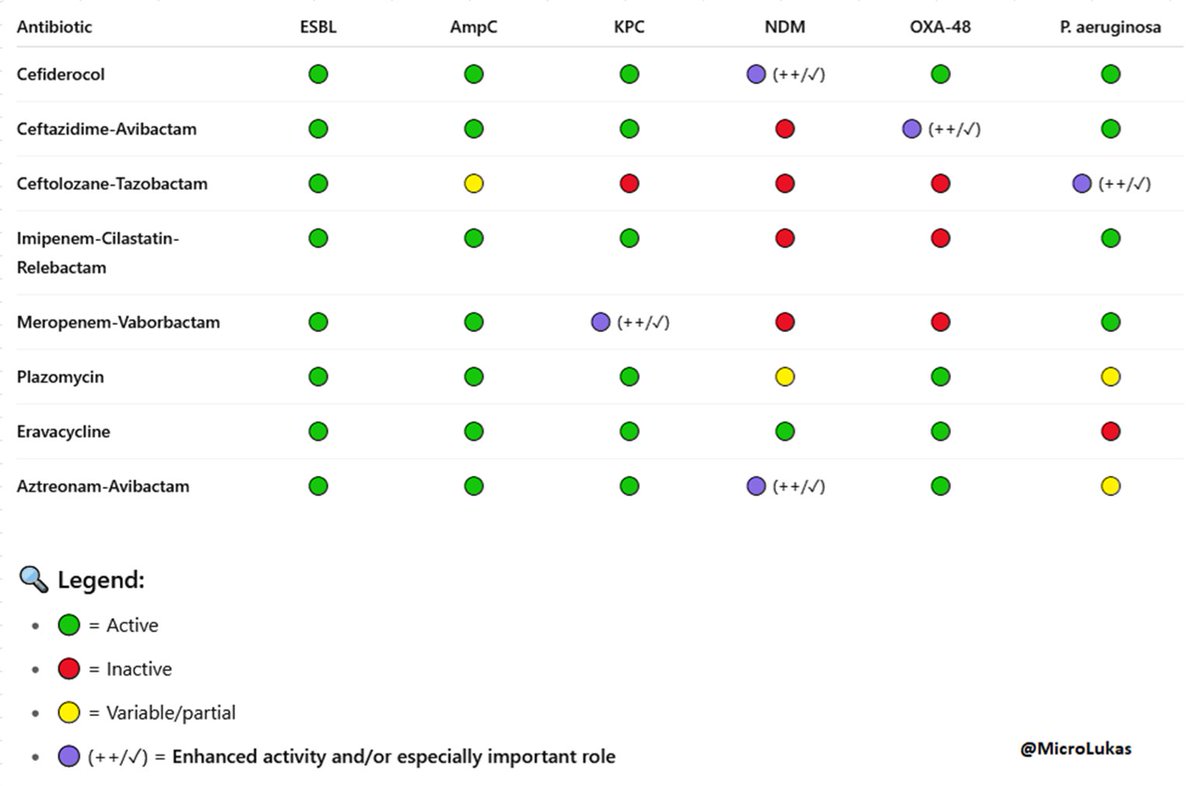
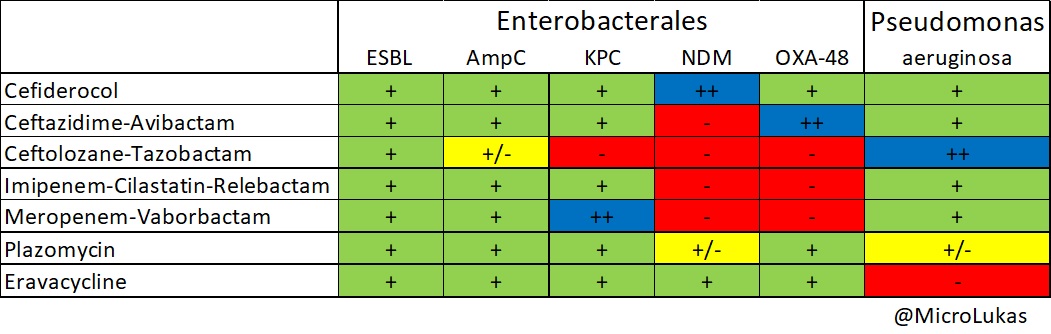
FDA approves cefepime/zidebactam (zaynich) for complicated urinary tract infections (cUTIs), including pyelonephritis 🎉
pharmacally.com/fda-approves…

Buenas noticias!!! 🎉🥳📰 @US_FDA🇺🇸 APRUEBA #Cefepime/ZIDEBACTAM✅ en #ITUcomplicada 🚽
👉🏻SUPERIORIDAD 🆚 #meropenem en Ens Clin F3 #ENHANCE-1 🥇
👉🏻Antibiótico de amplio espectro incluyendo #KPC, #OXA48 y #MetaloBlactamasas (VIM, NDM,IMP)
@pharmacally 🆓🔗pharmacally.com/fda-approves…


2
5
13
2,052
Jun 1
It combines cefepime’s activity against penicillin-binding protein 3 (PBP3) with zidebactam’s selective inhibition of penicillin-binding protein 2 (PBP2).
1
2
358
Jun 1
Which of the following has an extremely slow doubling time of ~12–14 days? ⏰
6%
Yersinia pestis
9%
Clostridium perfringens
86%
Mycobacterium leprae
35 votes • Final results
1
3
11
1,560
Jun 1
Yersinia pestis ❌
Intermediate-fast grower
Doubling time: ~1-2 hours
Grows well on standard media (e.g., blood agar, MacConkey)
Slower than Clostridium perfringens but still a relatively rapid pathogen compared with most bacteria
1
1
1
603
Jun 1
Mycobacterium leprae ✅
Extremely slow 🦥
Estimated doubling time: ~12-14 days
Cannot be cultured in standard artificial media
Requires intracellular growth in host tissues (e.g., Schwann cells)
1
1
180