
Professor of Psychiatry & Beh Sciences @StanfordMed decreasing stigma/increasing evidence/improving care. Food tweets. Digital Ed @BMJMentalHealth Opinions mine
Joined January 2013
- Tweets 21,667
- Following 1,009
- Followers 4,021
- Likes 46,647
1,744 Photos and videos








Pinned Tweet

14 Mar 2023
Just had a patient tell me today that my prescribing acamprosate saved his life. Hasn't drank since. "I just don't think about it anymore." Never had someone taking gabapentin tell me that, so just a reminder to all of you out there to follow the data and to watch your biases.😀
30
32
252
44,109
Michael Ostacher, MD, MPH retweeted

There are people in anti-psychiatry spaces who deny the existence of mental illness…
who invalidate the lived experience of patients…
and who shame people for taking medication.
No one deserves to experience stigma due to mental health illiteracy. ✌️
9
23
80
1,613
He should give the government stock options instead

elon being worth $1 trillion does not mean elon has $1 trillion in the bank.
most of the people i see arguing for a 5% annual wealth tax appear to be willfully misunderstanding this.
202
Michael Ostacher, MD, MPH retweeted

Jun 13

Jun 13

Some Predictions About the Future of “Withdrawal Studies”
What we talk about when we talk about antidepressant withdrawal
psychiatrymargins.com/p/some…
3
15
1,283
This is important to read. 👇🏼👇🏼👇🏼
Even as I disagree with many parts of it (the permanent neurological injury and lived “saved” parts, for example, I wouldn’t assert), this is a necessary perspective. No absolutes, let’s not cancel each other out but try to do better.

Dear anti-psychiatry, this "mental illness isn't real" narrative is making us look bad.
SSRIs can cause permanent neurological injuries that destroy lives via mechanisms we don't understand, and those experiences are not canceled out by the lives they 'save'.
That fact doesn't mean that mental illness isn't real, or is just a simple result of not enough sunshine or human connection. There are many forms of severe idiopathic mental illness that people suffer from, and those diseases are also deserving of legitimate treatment.
Has psychiatry exploited this and gone too far in some instances? Yes. Absolutely. Diagnosing every kid who can't sit still or focus with ADHD and medicating them is a criminal example of this.
However, there are many people who chronically struggle with severe mental illness that cannot easily be cured by natural remedies, and those people are desperate for help. The problem is that those people are just as vulnerable to SSRI neurological injury as those who 'didn't need' them. The mechanisms behind these injuries need to be fully understood, predictable and preventable before they continue to be carelessly given, period.
In the meantime, psychiatrists need to stop writing SSRIs off as merely "less than perfect", and the anti-psychiatry movement needs to stop promoting the idea that the mental illness that MI sufferers sought relief from isn't real in the first place.
The way forward is to simultaneously acknowledge that mental illness is real, and med harm is not just a necessary and unfortunate byproduct of trying to fix it. Med harm is real and a crime against humanity, and the suffering that leads people to become med harmed in the first place is equally real.
To reconcile these two outcomes by saying "they save lives, but they're not perfect" is not good enough.
Neither is saying "all mental illness isn't real, you just need more sunshine and meaning".
Psychiatry and anti-psychiatry needs to do better if we ever want this situation to progress.
5
2
10
1,261
I doubt it.

Pessimists sound smart.
Optimists build the world.
192
Everyone is entitled to their opinion about the cause of their suffering. Let’s support all who need it, what ever way works best, and to advocate for research into better understanding how to avoid and how to treat this.

While certain psychiatrists on X, argue definitions, time frames and each other's word salads, there's real people suffering through real long-term withdrawal as a necessity to prevent the seizures and other destabilizing WD from irresponsible Rx rapid tapers. I've been tapering for 66 months in total. I'm off 11 psych meds (yes, my ex GP was Big Pharma's best sales woman). I'm down to 6.25mg Seroquel with another year or so to go and then I've still got to taper another 2 psych meds.
Not rare! Just rarely acknowledged by those profiting off the harm.
4
401
Michael Ostacher, MD, MPH retweeted
Paccheri al ragù di coniglio but without the paccheri and without the coniglio. Calamarata and (dare say it) turkey instead. Rabbit is hard to find and it would upset @Noahpinion anyway. It’s really for @adamcifu. Umbria was great. #twittersupperclub

1
3
6
668
Paccheri al ragù di coniglio but without the paccheri and without the coniglio. Calamarata and (dare say it) turkey instead. Rabbit is hard to find and it would upset @Noahpinion anyway. It’s really for @adamcifu. Umbria was great. #twittersupperclub
1
3
6
668
I can’t believe @ElvinBen liked this tweet during the last few seconds of the Knick game.
1
1
404
I thought the argument was that trust was going to increase in the people who didn’t have trust in the government on health. Not much better at all, and much worse amongst everyone else. thehill.com/policy/healthcar…
2
798
Michael Ostacher, MD, MPH retweeted

Jun 9
My daughter sends. She knows all about this. Also please come over so I can feed you
43
6,695
60,042
613,143
It’s good to compare different benzodiazepines for alcohol withdrawal, but this study is decidedly not a study of symptom driven dosing. Symptom driven benzodiazepine dosing using CIWA-Ar scores is the standard of care. psychiatrist.com/pcc/lorazep…
4
2
15
5,577
If only more people around here were like this…
Jun 7

Yes, I had a very severe reaction to my second Moderna shot. But part of being a responsible scientist with a large platform is not extrapolating my personal experience to the entire population.
I also have a rare autoimmune condition called Parsonage-Turner syndrome (diagnosed in 2013), so I may have been particularly vulnerable to side effects.
Given my bad experience with the first mRNA vaccine I've ever taken, I have made the personal decision to avoid them in the future.
However, it would have been incredibly unscientific and highly irresponsible of me to take this personal experience of mine and start telling millions of people online to not get vaccinated for COVID.
There's a reason quack alternative medicine practitioners plaster personal testimonies all over their websites. They sound convincing to a lot of people. But it's purely manipulation. Personal testimony, even a large collection of them, isn't a substitute for real, population-level data.
I am not an expert on vaccines, the COVID vaccine, or epidemiology in general. So when I experience a serious side effect taking something with a non-zero rate of serious side effects, I understand that my personal experience likely isn't an indication that we're all being lied to about safety.
You should understand that as well.
The impulse to extrapolate a very negative personal experience to the entire population is very strong. But responsible scientists, and especially those with large public platforms, should resist that impulse.
9
1
22
3,087
Really interesting piece by John Campo. I do find it disconcerting for him to say that the field of psychiatry discounts religious experience, as I find the opposite to be true. Perhaps it’s because of my position in addiction treatment, where spirituality and religion are an important part of care, because the integration of people’s religious and spiritual lives into their recovery seems the foundation of the work that I (and the people I work with) do. And yes, our bodies will one day fail us, but that is a universal truth. washingtonpost.com/opinions/…
3
2
19
934
Michael Ostacher, MD, MPH retweeted

You are correct. Is the withdrawal theory built on a misinterpretation of the original paper? 🚨
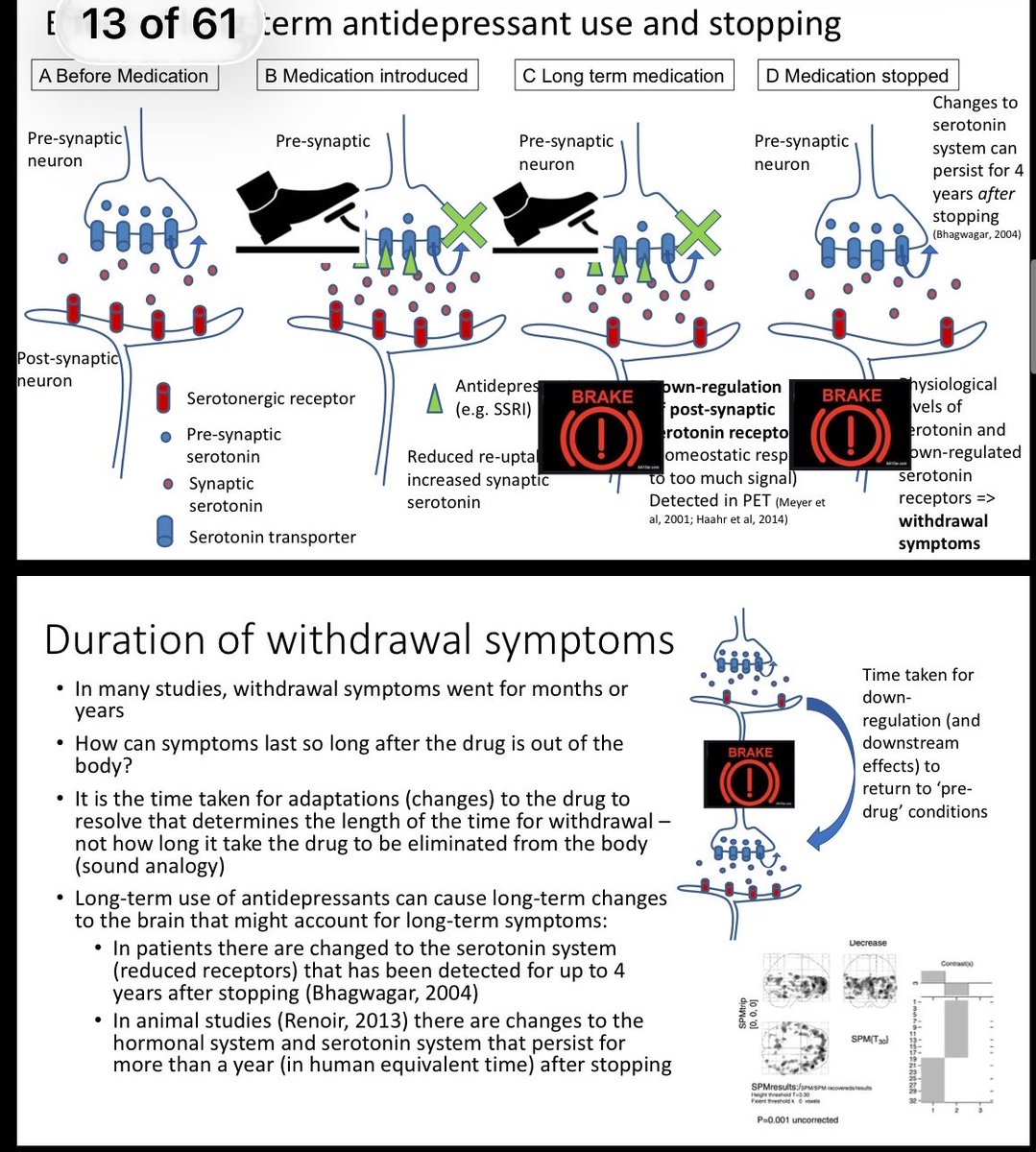
One of the basic foundations of the theory is see Top Right and then on second slide as well ( slides from his talk - publically available)
Exhibit 1:
slide - “Changes to serotonin system can persist for 4 years after stopping.”
Bhagwagar, 2004
Bhagwagar conclusion 👉 “Lowered 5-HT(1A) receptor binding availability could represent a trait abnormality that confers vulnerability to recurrent major depression.”
See the issue ?
It did not demonstrate that antidepressants caused the receptor finding. It did not study withdrawal. It did not establish a pre-medication baseline. It did not show that receptor change caused post-cessation symptoms.
Exhibit 2 :
Slide 2 “In Animal studies there are changes to the hormonal and serotonin
System that persist for more than a year ( human equivalent) after stopping “
Renoir paper 👉 no such extrapolation
“The majority of studies to date have been based on “normal” animals, whereas the clinical population who develop the discontinuation syndrome are typically taking SSRIs for treatment of depression, anxiety, etc. As such, future studies of the SSRI discontinuation syndrome in rodents should encompass well-established animal models of depression, chronic SSRI treatment, followed by an appropriate period of drug withdrawal.”
Exhibit3:
Abstract from Lancet paper ( Horowitz and Taylor ) - “therefore suggest that SSRIs should be tapered hyperbolically and slowly to doses much lower than those of therapeutic minimums, in line with tapering regimens for other medications associated with withdrawal symptoms. Withdrawal symptoms will then be minimised.”
Will be minimised? WILL ?
How is it ok to run with these loose interpretations?

More insults from Mark Horowitz. He doesn’t like that I think he’s quite wrong about the prevalence of “incapacitating” withdrawal or that there isn’t actual evidence for his tapering theories but so be it.
2
6
17
2,420
Who is this woman and why is she criticizing me and then blocking me. Don’t worry lady: unless you are a United Stats Veteran you don’t have to worry about with treated by me.
11
3
25
3,102