
Associate Professor in Psychiatry (AdelaideU). Maudsley Deprescribing Guidelines: amzn.to/3tTQq9s (US) amzn.to/40o3wrI (UK)
Joined April 2013
- Tweets 6,866
- Following 367
- Followers 13,133
- Likes 12,629
230 Photos and videos






Pinned Tweet

31 Jul 2025
I've written a blog in response to @awaisaftab's misleading blog about Kalfas: "No, the Kalfas Meta-Analysis Doesn’t Prove Antidepressant Withdrawal Is Modest: Nonsense Disguised as Nuance" bit.ly/4ofhd7S

13
43
156
40,198
It’s good to see wider discussion of withdrawal and hyperbolic tapering, including critiques. My observation is that whenever a clinician who is minimising the existence of withdrawal or the need for hyperbolic tapering is asked about their deprescribing experience they give vague answers like ‘I stop drugs all the time’ but when pressed for details trail off. Of course reading the literature is a part of being informed but actual first hand experience of large volumes of deprescribing teaches you a lot more. Everyone is entitled to an opinion but I think it is worth probing how informed such opinions are. Most friends of mine in psychiatry who are not invested in this debate either way rarely if ever stop long term drugs without switching to another or are seeing people on large numbers of drugs which buffer withdrawal effects. In other words they rarely have the chance to see withdrawal effects. I don’t want to make generalisations but I wonder where some people derive the confidence in their opinions? For example I have overseen about 4000 people coming off their drugs and I have very little idea what these drugs are doing in long term to the brain but there are some let’s say concerning signals - I would like to learn from people with much greater confidence than me what the source of their insights are.
3
19
55
1,144
Who could have seen that coming!
Jun 12

I just saw an akathisia-like report of someone on the new COBENFY drug that was claimed to not cause akathisia based on clinical trial data.
There’s angry people online discussing being gaslit by healthcare professionals over this.
How many have to die before acknowledgment?
2
3
23
978
Yes no need for all the hyperbolic guff, the product of the frenzied imagination of a few ideologues and hundreds of thousands of hysterical patients, several clearly irrelevant cohort studies, suggestive meta-analyses (which find slower tapering reduces apparent relapse rate) and totally plucked out of thin air fundamental laws of pharmacology (the equivalent of law of gravity in physics).
What makes sense is a linear taper that has never been shown to be safe or effective and does not cohere with basic laws of pharmacology and which (clearly hysterical) patients keep on saying has caused them protracted withdrawal syndrome (which is another term that hysterical patients give to their hysteria. Have I mentioned that hundreds of thousands of non-hysterical people suddenly become hysterical a few days or weeks after stopping antidepressants? That new-onset hysteria just hits hard. )
However, I do agree with Awais that there is a group of hysterical people on the internet who are having trouble accepting reality.

The quasi-linear I’ve described is an intersection of two lines that have different slopes. If that’s sufficient, great! No need for all the hyperbolic stuff.
7
13
48
3,276
The inimitable @doctor_benji summarising his conflicted feelings about being a psychiatrist with his signature dark humour. Good to see @bmj_latest publishing high impact material.
Jun 11

|cw: self-harm|
Medical Stand-up: Google Reviews of a Psychiatric Hospital with comedian @doctor_benji in support of @DoctorsDistress
5
2
20
1,589
Mark Horowitz @markhoro.bsky.social retweeted

While certain psychiatrists on X, argue definitions, time frames and each other's word salads, there's real people suffering through real long-term withdrawal as a necessity to prevent the seizures and other destabilizing WD from irresponsible Rx rapid tapers. I've been tapering for 66 months in total. I'm off 11 psych meds (yes, my ex GP was Big Pharma's best sales woman). I'm down to 6.25mg Seroquel with another year or so to go and then I've still got to taper another 2 psych meds.
Not rare! Just rarely acknowledged by those profiting off the harm.

There are hundreds of thousands of members in withdrawal-related support groups and that figure does not include the countless individuals who never formally joined these communities or those who suffered in isolation, never finding them at all.
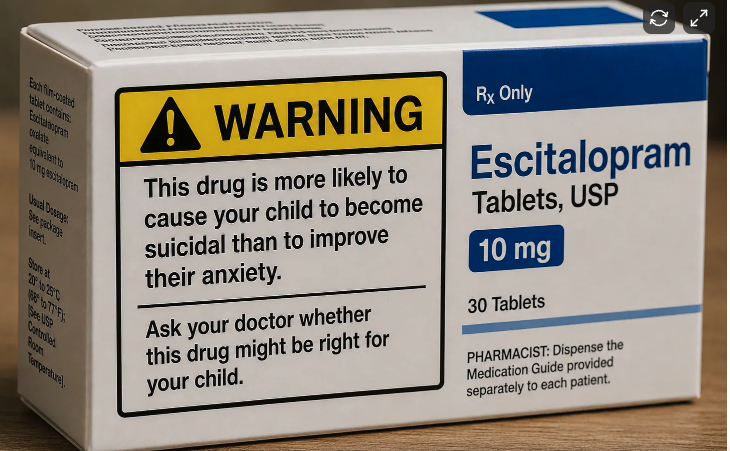
It is a profound failure that drug manufacturers and regulators did not adequately warn patients, people who simply trusted their doctors, about the possibility of severe, life-altering withdrawal and the need for careful, often years-long tapering. For many long-term users, tapering is not a passive process. It requires measuring tiny amounts of medication (crumbs, beads, or drops) with extraordinary precision to avoid debilitating symptoms.
In the absence of meaningful medical guidance, patients have become the experts, creating makeshift laboratories in their kitchens and developing tapering methods through necessity and lived experience. Attempts to dismiss these experiences as mere anecdote, or to discredit patients’ accounts of their own bodies and minds because they have a mental health diagnosis, are fundamentally anti-patient.
9
18
67
2,691
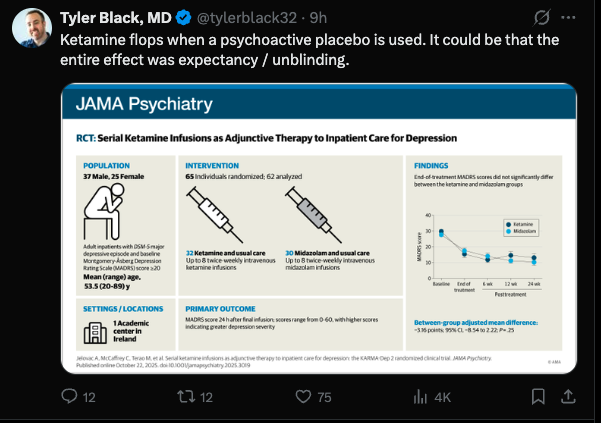
This comment is a clear symptom of relapse. This person sounds unmedicated.
Jun 11

My Lamictal taper is a clear example of withdrawal—there's nothing to "relapse." I was prescribed it off-label for misophonia, which it never helped with.
Yet since stopping, I've had panic, akathisia, and heart palpitations right after a cut—all of which fade with time.
4
2
28
3,649
Very useful article in @TheBJPsych evaluating different off-lablel techniques for making small doses to make hyperbolic tapering feasible: reassuring that all were found to be within 90-110% of target values (the same standard used for manufactured tablets).

Hyperbolic tapering is increasingly recommended for the gradual reduction of psychiatric drugs to minimise withdrawal symptoms, yet available formulations rarely accommodate the small dose regimens required. cambridge.org/core/journals/…
5
13
28
2,362
Mark Horowitz @markhoro.bsky.social retweeted

Jun 10
If it is not controversial why does it need to be said by an anonymous account? Both the empirical authority and moral high ground reached for here are immediately ceded by the creation of a sock account.
5
8
40
1,485
Not only is Nicolas a wonderfully polite man to call his interlocutors ‘advocates’ but Cochrane reviews find nnts of more than 9. But more importantly these measures are made after 8 weeks of drug or placebo. Lots of drugs look effective at 8 weeks - benzos for anxiety and opioids for pain - but wear off over time because of tolerance. Not to mention all the methodological issues such as unblinding that exaggerate the difference between placebo and antidepressants.
Jun 11

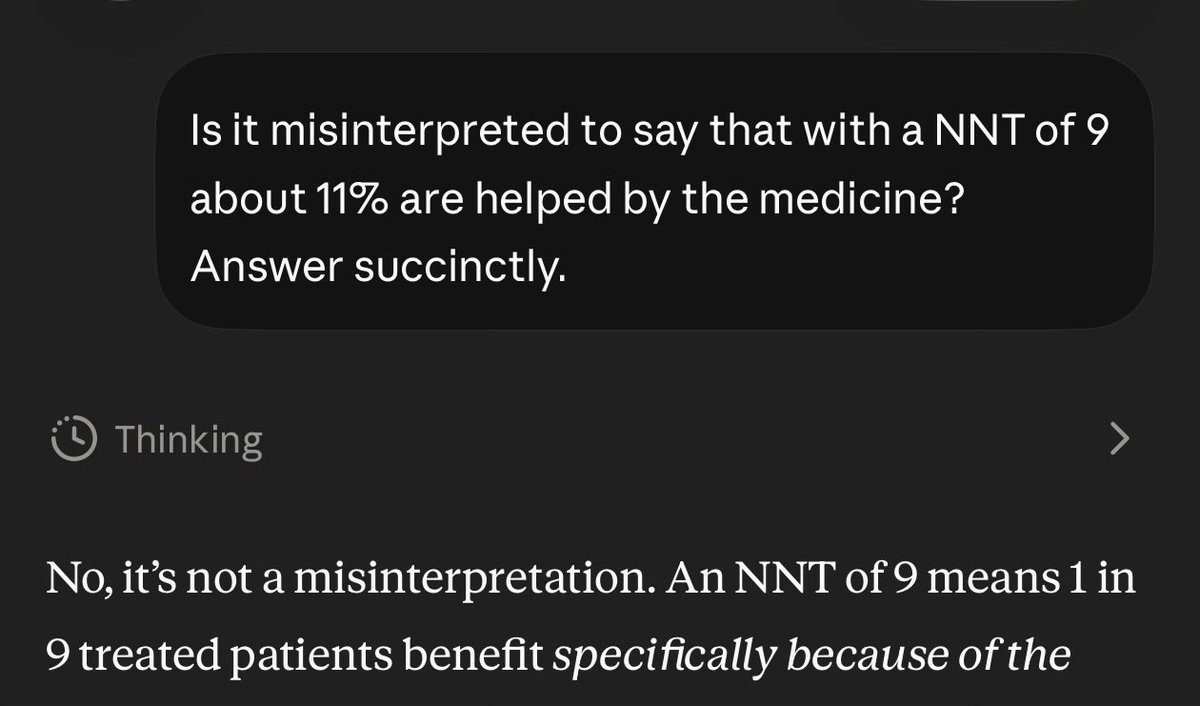
@sanilrege “incorrect” -> Grok “No”
@tylerblack32 “misinterpreted” -> Gemini “No”
@vitorborin_ “inaccurate” -> Claude “No”
Look, I appreciate those advocates doing their thing, but I am not an advocate. I don’t try to interpret things in a positive light but an accurate one.
Psychiatry deals with very fraught issues. We should be honest about our limitations and not spin things positively.
I would have been fine with them saying the NNT could be interpreted in other ways, or that placebos don’t exist in the real world, but instead they used precise words which IMO ended up being more inaccurate. I don’t think that 11% helped is that bad; it just is what it is.


1
7
27
1,948
It’s expensive to do research
Jun 11

Criticizing the pharmaceutical industrial complex WITH evidence is almost impossible.
This is a feature, not a bug.
There is decades of published research supporting the notion that medication intervention is indicated and optimal.
Research in the opposite direction is purposely suppressed.
4
7
27
2,303
Mark Horowitz @markhoro.bsky.social retweeted

Jun 11
“I rarely see this in my clinical practice”
All it takes is to ask around one’s social circle and you start to realise how common this is…

Posted on Instagram about the pains of tapering off Cymbalta, and THREE friends out of the 200 who viewed it reached out to share that they've been through this with antidepressants too. One had to take off work because it was so brutal.
This is happening all around us.
2
10
48
2,724
Mark Horowitz @markhoro.bsky.social retweeted

Posted on Instagram about the pains of tapering off Cymbalta, and THREE friends out of the 200 who viewed it reached out to share that they've been through this with antidepressants too. One had to take off work because it was so brutal.
This is happening all around us.
16
14
138
11,558
Mark Horowitz @markhoro.bsky.social retweeted

Jun 11
Calling proponents of informed consent "anti-psychiatry" is a convenient way to shut down dialogue around medication risks.
Many of us can hold nuance—meds help people and harm people. Everyone has the right to understand that and choose the best option for them.
5
8
41
2,134
I think kaddles speaks for a lot of patients here. A lot of clever psychiatrists on here missing the point because they are blind to the scale of the issue for reasons I outline in this blog. Unfortunately this leads to so many people's lives upended or worse from mostly preventable harm. mhorowitz.substack.com/p/why…
Jun 8

What I think about when I see psychiatrists on social media debating semantics and deftly diverting attention, as someone whose life has been profoundly affected by psychiatric drug harm. 🧵 (1/9)

1
22
52
3,934
Good to see deprescribing being taken up by clinics around the world as a particular focus. Hopefully the public system will take up this area of practice and eliminate the need for private services to fix up the mess made by decades of prescribing without adequate attention paid to stopping.

(1/2) A psychiatric clinic in New Zealand is running an advert in a major NZ media outlet talking about antidepressant withdrawal to draw attention to what it calls "medication optimisation" and its wider services. Makes me wonder if this clinic is reading the room...
"Stopping antidepressants too quickly can lead to withdrawal symptoms such as anxiety, insomnia, dizziness, nausea, and mood swings. Clinical guidance recommends a gradual reduction to minimise these issues, mainly because withdrawal can be mistaken for a return of the original condition***. Without proper support, individuals may become stuck: unable to stop, unsure whether they are experiencing withdrawal or relapse, or returning to medication."

5
19
49
2,172
Mark Horowitz @markhoro.bsky.social retweeted

Jun 9
So good to read these thoughtful, caring comments from prescribers who are happy to learn they may not have received all the necessary information prior to prescribing…. ♥️🎉

I received a number of messages appreciative of me sharing feedback from clinicians on the ground (mostly GPs) who I lecture to about withdrawal and deprescribing (most weeks at least once and sometimes up to three times a week) as an antidote to the general defensiveness, deflection, minimisation and denial that mostly characterises the responses of a small group of very vocal, often quite extreme, ideologically driven clinicians on this platform.
So here are some more de-identified comments from 300 GPs that I lectured to in an English ICB as part of their move to reduce inappropriate antidepressant prescribing.
“This very insightful webinar should be made mandatory for all clinicians in primary care in our region. Can the moderators raise this with the ICB?”
“This was one of the most sensible and interesting webinar I have listened to for a while. Thank you “
“Thanks really clear and useful”
“That was so refreshing. Thanks for being so positive. Can you come and speak to our clinical staff?? 23000 patients”
“Excellent session and does raise the valid point of reviewing these along with other medicines/doses for older patients due to pharmacokinetic/pharmacodynamic changes. We need to be more proactive in reviewing long term medicines and the original indication as you highlighted for the AD”
“If there is a down regulation of serotonin receptors naturally through homeostosis, how is the drug even effective? Wouldn't the extra serotonin be pointless? Is it more of a psychological effect from taking the anti-depressant?”
“does this only apply to patients who are on them for their mental health? what about patients who are on them for chronic pain? secondary care are pushing ALOT for SNRI/SSRI for chronic pain - just had a letter from gynae to use it for a lady with endometriosis.....?! “
“this is fascinating and makes perfect sense. I'm very guilty of doing all the wrong things you have mentioned. I do worry that such a slow withdrawal it is not very practical in the real world. It is making me think about the fact that I think we are too happy to start these medications and give little consideration to the risks of stopping. Though I think this reflects the fact that we have few other options given the waiting times for talking therapies. “
“so does this sort of withdrawal effects in terms of the worst happening on the lower doses, same principle for opioids and gabapentinoids?”
Of course there are numerous practical barriers to implementation pointed out by the GPs as well as lots of clinical dilemmas:
“A bottle of sertraline costs £201.80”
“For patients who’ve been on ADs for many years, and reached a roughly steady state, they’re often very reluctant to come off them. Looking at the prevalence and severity of withdrawal in this cohort, I can see their point. How would you advise these patients? Do the risks of ongoing rx outweigh the risks of withdrawal?”
1
7
537
Germane.
Jun 8

“ Apparently, once a belief becomes part of our identity, our brains stop treating information as information and start treating it as a territorial dispute. At that point, facts are no longer facts, they're invading armies.” Seems germane. Full piece facebook.com/share/1HFAZBnpd…
2
4
11
1,705
I don't want to make Professor Ostacher feel he is being persecuted but I am still waiting for him or anyone else to present RCT evidence that linear tapering is effective and safe.
That would be the only reasonable circumstance to demand the high bar of RCT evidence for hyperbolic tapering in order to overturn an 'established' approach.
The only evidence ever offered for a linear approach is 'I have seen it work'. On top of this 'anecdotal' evidence, what possible theoretical principle could be put forward for this approach as default given the known neurobiology?
In other words hyperbolic tapering has biological plausibility, and numerous cohort studies (see Groot and van Os, multiple studies), whereas linear tapering has neither.
Again, for those who wish to erect strawmen, hyperbolic tapering does not have to be extended if someone has no problem. Given the risk of severe withdrawal effects, akathisia, suicidality and protracted withdrawal effects not starting with a cautious approach seems reckless.
The recklessness of that approach is on full show in all the patients reporting the problems that have resulted from such tapers.
I am still waiting....
4
19
61
4,102
To the 'it's all psychosomatic or FND crowd' who seem to be out in full force at the moment: it would be quite peculiar for 100,000s of people to all develop FND a few days or weeks after stopping antidepressants or other psychiatric drugs. That would be some co-incidence!
And for those charming souls who are going for the 'these sort of people are really nutters and not a word they say can be taken at face value': in the US in some states more than 50% of people have been prescribed an antidepressant at some point in their life: that is a lot of nutters out there who can't be taken seriously!
The comments section to my blog is full of clinicians who did not believe stories about withdrawal until they went through it themselves, including psychiatrists, GPs and nurses: mhorowitz.substack.com/p/why…
But this blog probably needs to be updated at this point to include the point that there are none so blind as those who will not see.
13
36
115
8,408
I received a number of messages appreciative of me sharing feedback from clinicians on the ground (mostly GPs) who I lecture to about withdrawal and deprescribing (most weeks at least once and sometimes up to three times a week) as an antidote to the general defensiveness, deflection, minimisation and denial that mostly characterises the responses of a small group of very vocal, often quite extreme, ideologically driven clinicians on this platform.
So here are some more de-identified comments from 300 GPs that I lectured to in an English ICB as part of their move to reduce inappropriate antidepressant prescribing.
“This very insightful webinar should be made mandatory for all clinicians in primary care in our region. Can the moderators raise this with the ICB?”
“This was one of the most sensible and interesting webinar I have listened to for a while. Thank you “
“Thanks really clear and useful”
“That was so refreshing. Thanks for being so positive. Can you come and speak to our clinical staff?? 23000 patients”
“Excellent session and does raise the valid point of reviewing these along with other medicines/doses for older patients due to pharmacokinetic/pharmacodynamic changes. We need to be more proactive in reviewing long term medicines and the original indication as you highlighted for the AD”
“If there is a down regulation of serotonin receptors naturally through homeostosis, how is the drug even effective? Wouldn't the extra serotonin be pointless? Is it more of a psychological effect from taking the anti-depressant?”
“does this only apply to patients who are on them for their mental health? what about patients who are on them for chronic pain? secondary care are pushing ALOT for SNRI/SSRI for chronic pain - just had a letter from gynae to use it for a lady with endometriosis.....?! “
“this is fascinating and makes perfect sense. I'm very guilty of doing all the wrong things you have mentioned. I do worry that such a slow withdrawal it is not very practical in the real world. It is making me think about the fact that I think we are too happy to start these medications and give little consideration to the risks of stopping. Though I think this reflects the fact that we have few other options given the waiting times for talking therapies. “
“so does this sort of withdrawal effects in terms of the worst happening on the lower doses, same principle for opioids and gabapentinoids?”
Of course there are numerous practical barriers to implementation pointed out by the GPs as well as lots of clinical dilemmas:
“A bottle of sertraline costs £201.80”
“For patients who’ve been on ADs for many years, and reached a roughly steady state, they’re often very reluctant to come off them. Looking at the prevalence and severity of withdrawal in this cohort, I can see their point. How would you advise these patients? Do the risks of ongoing rx outweigh the risks of withdrawal?”
3
27
64
3,428