
Instructor @ MGH/ Harvard Med: AD biomarkers | Unraveling heterogeneity in AD | K01 awardee | catch me in the 🏔️ 🥾
Joined June 2009
- Tweets 849
- Following 996
- Followers 753
- Likes 3,550
65 Photos and videos













Pinned Tweet

19 Nov 2024
Work with @MathiasJucker showing neurofilment light chain (NfL) in both CSF and blood are early markers of neurodegeneration, but diverge in symptomatic (autosomal dominant) AD patients -> CSF NfL may be better for monitoring outcomes in symptomatic AD doi.org/10.1038/s41467-024-5…
1
9
933
Stephanie Schultz retweeted

27 Jan 2025
Excited to share our recent paper! We use genetics, bioinformatics, and cell-based studies to determine whether variants of unknown significance act as pathogenic variants to cause autosomal dominant Alzheimer’s disease @alzassociation @WashUMedADRC sciencedirect.com/science/ar…
10
44
2,861
Stephanie Schultz retweeted

7 Dec 2024
Wonderful summary of our results, thank you @alzforum. NfL is becoming so important as a readout in clinical Alzheimer trials! Do CSF and Plasma NfL Diverge After Alzheimer’s Disease Onset? alzforum.org/news/research-n…
1
6
628
Stephanie Schultz retweeted

🎉Congratulations @bettytijms! She has been awarded a @ERC_Research Consolidator Grant. With nearly 3 million euros in funding, she will investigate whether the 5 biological variants of Alzheimer’s disease respond differently to medication: amsterdamumc.org/en/research… @AlzheimerAms
1
4
18
639
Stephanie Schultz retweeted

12 Dec 2024
In preparation for the @ReservePIA year in review webinar in January, we are compiling the most important papers published last year about 🧠 reserve and resilience. Please, consider helping us finding the papers by completing the survey alz.surveymonkey.com/r/SLH6B…
3
5
488

In familial symptomatic Alzheimer's, NfL in CSF may track neurodegeneration more closely than in blood. @MassGeneralNews ow.ly/YKVp50UmNig
1
5
1,065
Stephanie Schultz retweeted

26 Nov 2024
Excited to share our @FraminghamStudy paper in @ANA_journals!🧠 Sex-specific links between stroke risk factors and subclinical vascular brain injury support tailored prevention strategies in aging.👇doi.org/10.1002/ana.27135
Big thanks to @sudha_md, Alexa, Matt, @bucklr01 & team!
4
8
31
2,270
Stephanie Schultz retweeted

26 Nov 2024
🔔👉@CognitionPia members, we need your input! In preparation for our @ISTAART Cognition PIA 2024 Year in Review webinar, please fill out this survey to submit publications & advancements from 2024 that you would like us to highlight. Deadline *Dec 9th*! 🙏alz.surveymonkey.com/r/SLH6B…
2
3
318
Stephanie Schultz retweeted

20 Nov 2024
Beautiful work by Liu et al. highlighting the importance of heterogeneity in amyloid-beta pathology, especially in the era of amyloid targeting therapies. I remember seeing this work at ADPD and am excited to see it published! @ElzHead @M_B_Miller
jamanetwork.com/journals/jam…
1
11
598
19 Nov 2024
Our latest study out today! Findings reveal PSEN2 variants with known PSEN1 homolog variant show abnormal Aβ production patterns strongly correlated with age at symptom onset, while non-homologous PSEN2 variants often exhibit wild-type-like Aβ ratios
doi.org/10.1002/alz.14339
2
18
1,610
Stephanie Schultz retweeted
18 Nov 2024
Trajectories of neurofilament light chain (a presumed marker of neurodegeneration) in CSF and blood over the entire course of (autosomal dominant) #Alzheimer's disease. doi.org/10.1038/s41467-024-5… Great collaboration with @Schultz_SA @DZNE_en @HIHTuebingen
5
29
2,138
Stephanie Schultz retweeted

5 Nov 2024
Having started my career in basic neuroscience research, I have always understood Alzheimer disease to mean the pathophysiology associated with amyloid plaques and tau tangles. As a clinician, I appreciate that the relationship between Alzheimer disease and cognitive impairment is complex.
1. Clinically diagnosing the cause of cognitive impairment is different than diagnosing that the patient has Alzheimer disease (pathology). Many of my patients with cognitive impairment have multiple diagnoses (e.g., sleep apnea, medication-related cognitive dysfunction, depression, previous cerebral infarction), and sometimes have Alzheimer disease (based on biomarker testing). I do what I can to mitigate the effects of all of these conditions, and when Alzheimer disease is present I do not assume that it is the sole or even the primary cause of cognitive impairment. This is true across multiple potential etiologies: for example, I may diagnose someone with cerebrovascular disease and a prior infarct based on MRI findings, but determine that this condition is asymptomatic and not contributing to their cognitive impairment.
2. Given the simplicity of some biomarker tests and the difficulty of clinical assessment, there is a risk that clinicians may diagnose the etiology of cognitive impairment as Alzheimer disease without doing a full work-up. This is why appropriate use recommendations for biomarkers always mandate that biomarker results must be integrated with a clinical evaluation and not used as a “stand-alone.”
3. Alzheimer disease pathology accumulates silently for ~10-20 years before the onset of cognitive impairment. However, during this pre-clinical phase the accumulation of amyloid pathology is associated with many other biomarker changes that appear pathological (e.g., abnormal CSF synaptic biomarkers, brain atrophy, brain hypometabolism). While the brain is remarkably resilient to damage and individuals may or may not develop symptoms, the brain is sick and the pre-clinical phase is a disease state.
4. Suggesting that a disease only exists when organs are severely damaged and failing (dementia) seems counter to what we have learned in other areas of medicine. For example, patients diagnosed with hypertension or asymptomatic coronary artery disease may change their diet and medications to avoid a heart attack. Individuals with asymptomatic chronic kidney disease may or may not go on to require dialysis, but they can be monitored and sometimes treated.
5. There are valid concerns about the stigma and risks of asymptomatic individuals being labeled as having Alzheimer disease given that they may or may not develop cognitive impairment. The solution is simple—we don’t perform biomarker testing in asymptomatic individuals outside of research studies or clinical trials. Again, this has been mandated by appropriate use recommendations for biomarkers.
We can help patients by promoting accurate understanding and appropriate use of biomarkers. #EndAlz
4
46
205
25,135
Stephanie Schultz retweeted

2 Nov 2024
🙌 @DesignDataPIA & @ReservePIA offer you a unique "#Resilience in #CognitiveAging" Webinar Series! Join us if you can 😎
Registration
DEC 6 👉 tinyurl.com/3z8x9f4e
DEC 11 👉 tinyurl.com/y7wmdw6y
@ytquiroz @ERogalskiPhD @RoreBole @ArenazaEider @DrAnaCapuano @DBartres_Faz

1
17
41
3,632
Stephanie Schultz retweeted

24 Oct 2024
Caesar delayed the Rubicon, King Arthur’s still wrangling stats with Merlin 🧙♂️, Michelangelo cracked his marble 🛠️, and Napoleon? He’s fine-tuning his graphs! 📊
SO… we’re pushing the abstract deadline to Tuesday, October 29, at NOON (US ET) ⏳
#HAI2024 #AbstractMadness
2
3
7
925
Stephanie Schultz retweeted

25 Sep 2024
This week, Dr. Reisa Sperling returns to the podcast to explore the different factors that can impact cognitive decline and early-stage #Alzheimers disease. Listen to her conversation with @NathanielChinMD on our website at go.wisc.edu/13yj88 or wherever you get your podcasts.

ALT Graphic design to announce the release of the new Dementia Matters podcast, "Taking a Closer Looka t Cognitive Decline and Preclinical Alzheimer's Disease" with guest Dr. Reisa Sperling.
12
30
1,936
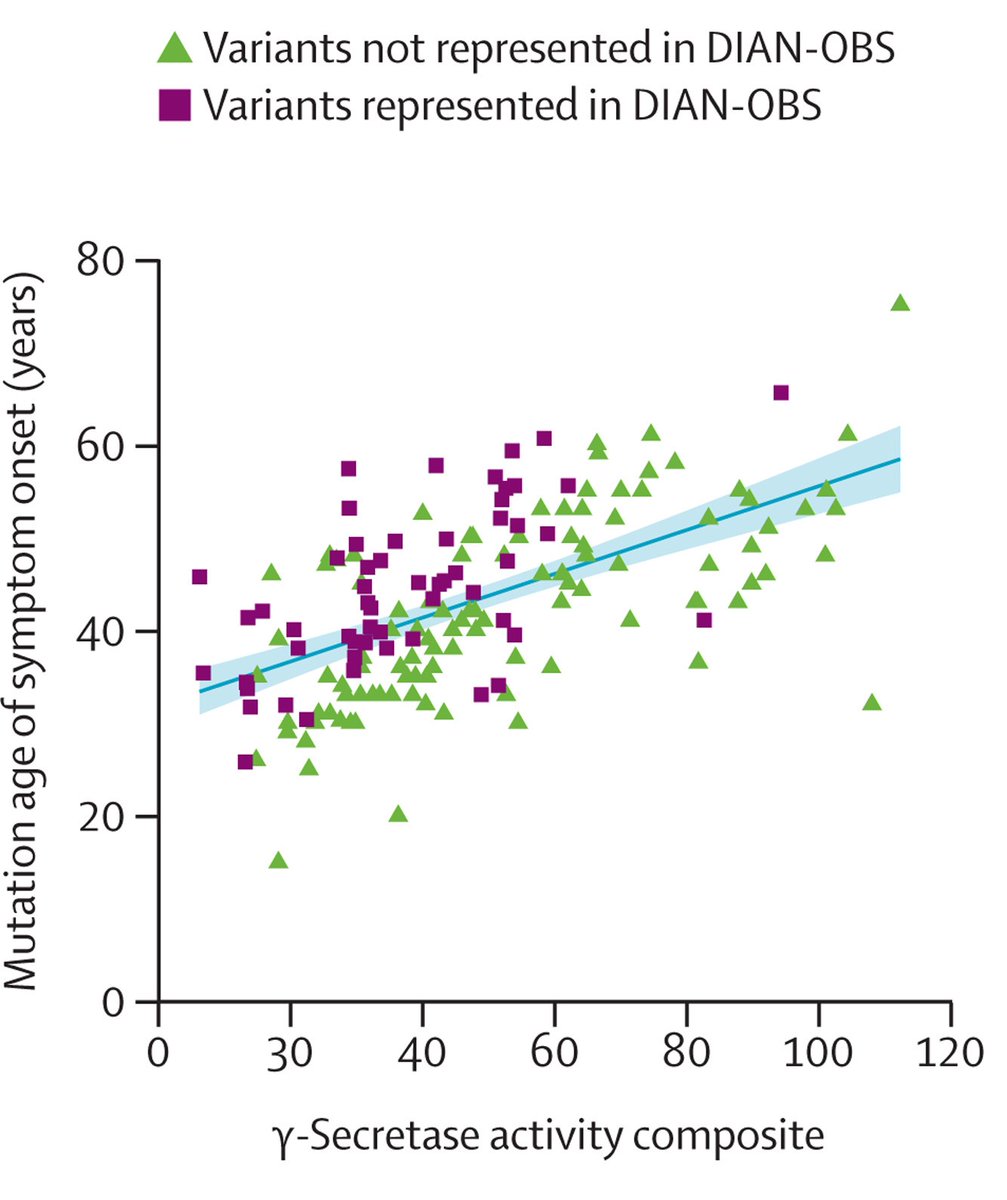
How presenilin mutations shift γ-secretase’s output of short versus long Aβ peptides explains the speed of pathogenesis and age at onset, supporting GSM development. @MGHNeurology @Schultz_SA @alzassociation #AAIC ow.ly/kywN50SZrFm
5
18
2,253
Stephanie Schultz retweeted
31 Jul 2024
I am excited to share our work, out now in @TheLancetNeuro, showing cell-based measures of gamma-secretase activity and amyloid production predict clinical, cognitive and biomarker features in autosomal dominant AD.
Link to paper: tinyurl.com/ye2a3d5u
@alzassociation #AAIC
1
13
49
9,567
Stephanie Schultz retweeted
2 Aug 2024
Happy to have been able to make a tiny contribution to this beautiful work by @ZhaoSun4 and Andrew Yoo…
Modeling late-onset AD neuropathology via direct neuronal reprogramming @WUADRC science.org/doi/10.1126/scie…
1
11
53
3,585
Stephanie Schultz retweeted

1 Aug 2024
An amazing story ❤️
31 Jul 2024

I am excited to share our work, out now in @TheLancetNeuro, showing cell-based measures of gamma-secretase activity and amyloid production predict clinical, cognitive and biomarker features in autosomal dominant AD.
Link to paper: tinyurl.com/ye2a3d5u
@alzassociation #AAIC
1
2
560