
A collaborative space led by GI medical oncologists to share research, learn together, and highlight what's evolving in GI cancers | #GIonc #OncTwitter
Joined June 2025
- Tweets 401
- Following 19
- Followers 581
- Likes 504
47 Photos and videos












Pinned Tweet

Feb 26
The Gut Onc Lab podcast now available on Apple Podcasts and Spotify! @GIMedOnc @TimothyJBrownMD @UGrewalMD
Spotify- open.spotify.com/show/34O9Yd…
Apple- podcasts.apple.com/us/podcas…
Subscribe and tune in! We’re planning to bring many thoughtful discussions to you in forthcoming episodes.
1
7
13
1,416
Gut Onc Lab retweeted
New @TheGutOncLab article.
EOCRC needs a different touch and a different lens.
Grateful to publish our work on symptom patterns in early-onset colorectal cancer.
Screening at 45 matters. But many patients are diagnosed before 45, which means screening alone will never solve this.
In this national inpatient analysis of 18,017 EOCRC hospitalizations, symptom patterns differed from later-onset CRC.
Constipation stood out:
📌 EOCRC: aOR 2.50
📌 LOCRC: aOR 1.12
📌 Women <40: aOR 5.72
One finding that stuck with me:
Among hospitalized adults age 40–44 with constipation, the rate of colon cancer was essentially the same as the overall CRC rate in hospitalized adults age 45–49.
That matters, not because constipation = cancer. It obviously does not. It matters because we have been trained to let age reassure us. And in EOCRC, that can be the miss.
A young patient with persistent constipation, iron deficiency, bleeding, changing bowel habits, or symptoms that just do not fit deserves a real workup.
At the end of the day, there is no such thing as “too young” to have cancer.
Proud to work on this with our resident Ashish Samaddar, @UGrewalMD, @TimothyJBrownMD, @sepideh_gholami , @Deebacca, and @TheGutOncLab
sciencedirect.com/science/ar…
2
8
19
1,051
Gut Onc Lab retweeted

important distinction you make!!!
Screening = expecting to be normal
Symptomatic = straight to standard Dx tools, not expected to be normal (age should never separate risk categories with symptoms)
1
3
65
Gut Onc Lab retweeted

Posted in early onset crc FB group.
Glad to include your analysis
facebook.com/groups/earlyons…
1
3
52
Gut Onc Lab retweeted
Had the chance to give the colorectal cancer update at Best of ASCO Los Angeles.
Always fun to summarize a year of CRC data in ~20 minutes while pretending that is a normal thing to ask of a human being.
4 takeaways (without getting into some of the really exciting drugs that are coming to CRC soon):
🔹 MSI-H CRC in complete clinical response on PD-1
Stopping at confirmed cCR looks safe. Maintenance may add toxicity without clear benefit.
🔹 BRAF V600E MSS mCRC
Encorafenib cetuximab chemotherapy is now a 1L standard. FOLFIRI is a great option, and FOLFOX is reasonable too. Either way, the targeted therapy backbone is here.
🔹 ctDNA / MRD
Not fully in NCCN yet, but increasingly actionable. I escalate select stage II patients, use it to frame de-escalation discussions, and strongly favor trials when possible.
🔹 Exercise
Prescribe it like we prescribe oxaliplatin.
30 min, 3x/week, ~80% max HR improves DFS/OS and is cost-saving.
CRC is moving fast. The challenge now is not just knowing the data, but figuring out how to apply it thoughtfully in clinic.
Grateful to be part of the conversation.
@TheGutOncLab @Onco_Nexus @OncoAlert @TotalHealthConf


1
12
28
1,413
Jun 10
Resharing free access link to the manuscript-shorturl.at/dxpVO
May 20

Managing toxicity is hard.
It is part science, part judgment, and part art. And it is not always fully spelled out in the package insert.
In advanced GI cancers, we spend a lot of time talking about the next drug, the next target, the next trial.
But for many patients, the most important question is more practical:
Can we deliver effective therapy in a way they can actually tolerate?
Dose modifications. Schedule adjustments. Quality of life.
This is the real world of oncology.
Grateful to publish this review with @GutOncLab, @UGrewalMD @TimothyJBrownMD @guildsman on optimizing systemic therapy for advanced GI cancers.
Personalized dosing is not “less aggressive” care.
Done thoughtfully, it is often better oncology.
@OncoAlert @Onco_Nexus
clinical-colorectal-cancer.c…
1
6
9
2,496
Gut Onc Lab retweeted

Jun 8
Finally out!!- A critical appraisal of literature and several practical insights from surgeon extraordinaire @SethConcorsMD and team on the role of primary tumor resection for patients with small bowel neuroendocrine tumors in the setting of metastatic disease @EndoCancer. @WinshipAtEmory @TheGutOncLab
erc.bioscientifica.com/view/…
On a personal note- I do think there is a role for PTR among patients with a symptomatic primary (caveat: symptoms can be very subtle or non-specific and therefore challenging to identify). The role of PTR remains less well-defined in asymptomatic primary tumors, especially among those with relatively indolent disease.

6
16
1,080
Gut Onc Lab retweeted

Thanks for bringing the best of #GIonc to the world ~ Sincerely #CommunityOncology
1
2
8
321
Gut Onc Lab retweeted

Happy anniversary! Thanks for the great content, gents :)
1
3
6
612
Gut Onc Lab retweeted

Jun 6
Nothing like publishing and recording with friends. Honestly, collaborations like this feel like a cheat code to doing great science and moving the needle forward a little bit at a time for patients.
Looking forward to growing the @TheGutOncLab and having some of our higher impact work come out.
Jun 6

It’s already been a year of @TheGutOncLab!! We decided that we wanted to do this a year ago at #ASCO25. Several projects, ideas and a podcast later-here we are! Looking forward to many more. 🍻 🎉 @GIMedOnc @TimothyJBrownMD @UGrewalMD
2
7
24
2,811
Jun 6
It’s already been a year of @TheGutOncLab!! We decided that we wanted to do this a year ago at #ASCO25. Several projects, ideas and a podcast later-here we are! Looking forward to many more. 🍻 🎉 @GIMedOnc @TimothyJBrownMD @UGrewalMD
2
3
29
5,357
Gut Onc Lab retweeted
Jun 3
A key study evaluating treatment sequencing for metastatic pancreatic NETs was just published in @TheLancetOncol
OCLURANDOM is the first randomized trial evaluating PRRT in pretreated, progressive, SSTR-positive metastatic panNETs.
While designed as a randomized, non-comparative phase 2 study, the results are difficult to ignore: 12-month PFS was 80.5% with 177Lu-DOTATATE compared with 41.9% with sunitinib (the study’s primary endpoint)
👉PRRT was also associated with fewer grade 3/4 adverse events (44% vs 72%), lower rates of severe neutropenia (5% vs 30%), and a clinically meaningful improvement in global health status/QoL.
One patient in the PRRT arm unfortunately developed AML.
🤔 An important caveat is that cross-arm comparisons should be interpreted cautiously given the study design.
👏That said, for years many of us have believed that treatment sequence may not substantially impact outcomes in NETs. Studies such as OCLURANDOM and COMPETE are beginning to challenge that notion. Perhaps using PRRT earlier in the treatment sequence is the way to go!?
These trials don’t tell us that our practice should be “PRRT first for everyone” as multi-disciplinary discussion and individualized decision-making remain essential.
👉However, trials like these are adding prospective evidence that seems to indicate that PRRT should be preferentially used earlier in the treatment sequence compared to targeted therapies.
I also eagerly await data from the COMPOSE and NET-RETREAT trials which will further put some of the missing pieces of the puzzle together. It’ll also be interesting to see how the advent of alpha RLT will impact the treatment landscape! @NCFCancer @CureNETs @NANETS1 @TheGutOncLab
Link- thelancet.com/journals/lanon…
5
16
742
Gut Onc Lab retweeted

A huge thank you to @UGrewalMD who’s mentorship and vision made this possible!
His guidance and relentless support has been a huge part of my journey!
Finding a home with @TheGutOncLab has been a great privilege 🔥
Jun 3

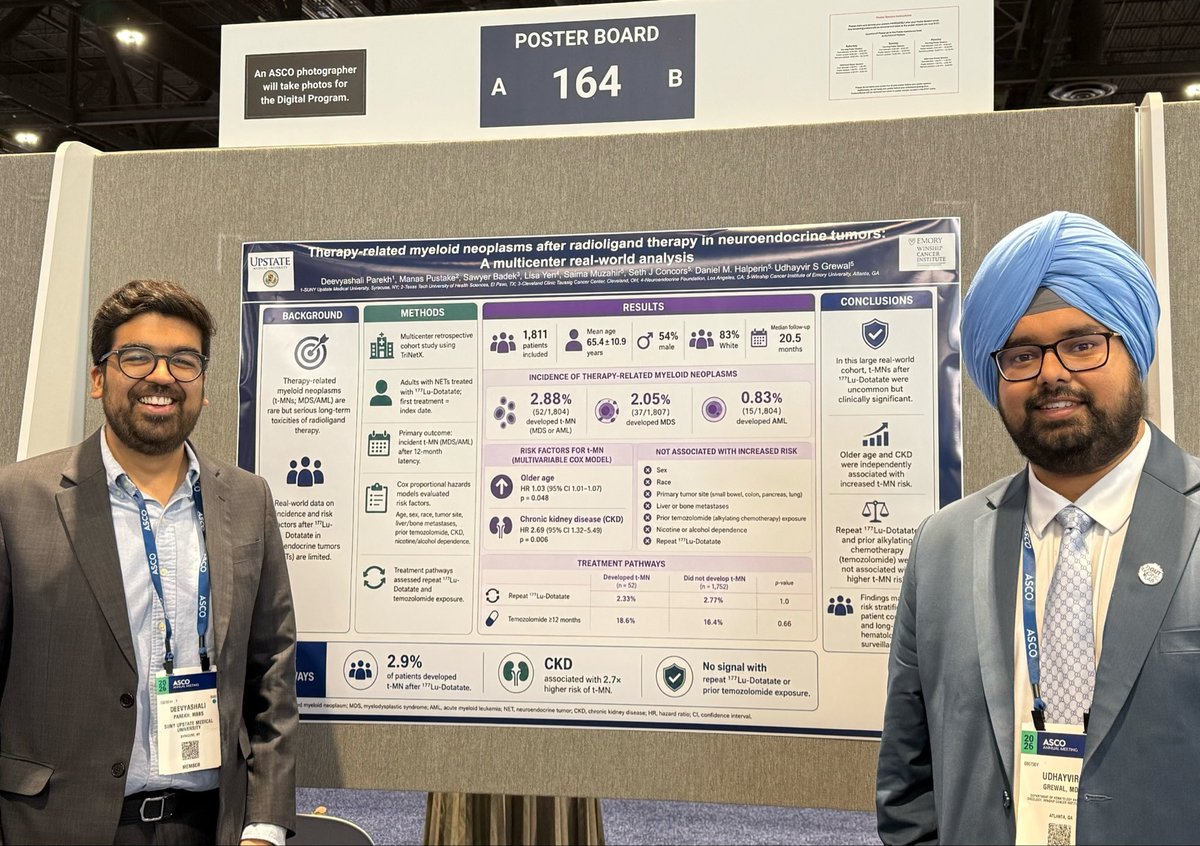
I wanted to take a moment and congratulate @deevyaparekh on his fantastic presentation at #ASCO26
Our study is the largest real world analysis to-date evaluating the risk of therapy-related myeloid neoplasms with Lu177-DOTATATE in patients with Neuroendocrine tumors. Full manuscript in progress.
Deevya will be joining @MontefioreNYC as a hematology/oncology fellow next month and I’m incredibly proud of all of his achievements. @TheGutOncLab
3
5
22
2,307
Gut Onc Lab retweeted
Jun 3
I wanted to take a moment and congratulate @deevyaparekh on his fantastic presentation at #ASCO26
Our study is the largest real world analysis to-date evaluating the risk of therapy-related myeloid neoplasms with Lu177-DOTATATE in patients with Neuroendocrine tumors. Full manuscript in progress.
Deevya will be joining @MontefioreNYC as a hematology/oncology fellow next month and I’m incredibly proud of all of his achievements. @TheGutOncLab
5
6
40
3,946
Gut Onc Lab retweeted
Jun 2
#ASCO26
The future is not just better drugs.
It is earlier molecular detection and targeted intervention.
SERENA-6: Camizestrant CDK4/6i vs AI CDK4/6i after emergent ESR1 mutation before radiographic progression
Such a next-gen trial design.
Here is the question:
If a patient on 1L treatment develops a marker of resistance in their blood, should we target that early with a new therapy?
Do not wait for the scan to get worse. Do not wait for patients to feel worse. Intervene the moment you see a hint of resistance.
Quick hits:
📌 Population
HR /HER2- advanced breast cancer
On 1L AI CDK4/6 inhibitor
Emergent ESR1 mutation detected by ctDNA
No radiographic progression yet
🔁 Intervention
Switch AI to camizestrant
Continue CDK4/6 inhibitor
🆚 Control
Continue AI CDK4/6 inhibitor
📈 PFS improved
16.8 vs 9.2 months
HR 0.45
📊 PFS2 improved
25.7 vs 19.1 months
HR 0.63
That PFS2 piece matters.
After the original 2025 ASCO plenary, this was one of the major questions: are we just moving treatment earlier, or are we actually improving the overall disease course?
This update makes the argument stronger. The model works, liquid biopsy detects resistance before clinical progression.
This is where oncology is going: molecular monitoring, adaptive therapy, and earlier targeted switches before the old clinical milestones show up.
Hopefully the FDA figures out how to evaluate this kind of strategy.
Because if we only accept the old paradigm, we will keep designing trials around waiting for patients to get worse.
That cannot be the future.
@TheGutonclab @UGrewalMD @TimothyJBrownMD @OncoAlert @Onco_Nexus @ASCO
@NazliDizman @LauraAlderMD @DVAraujoMD @DrBarbiOnc @LauraEsfeller @FunchainMD @YGaritaonaindia @DrSAHaddad @jgong15 @iandresmeraz @SakditadMD @RamilaShilpakar @RohitBanwar @lungoncdoc
2
9
28
3,239
Jun 1
Are you a GI med onc or community hematologist/oncologist routinely seeing patients with GI malignancies? we’d love to hear from you.
Please take 1-2 minutes to answer some simple questions for this survey.
redcap.link/5FU
@GIMedOnc @TimothyJBrownMD @UGrewalMD
3
3
716
Gut Onc Lab retweeted
Jun 1
#ASCO26
Personalized cancer vaccines are the next frontier.
Intismeran autogene pembrolizumab vs pembrolizumab in high-risk resected melanoma: 5-year KEYNOTE-942 update
What we are really talking about here is individualized neoantigen therapy: sequence the tumor, identify patient-specific neoantigens, manufacture an mRNA therapy, and train the immune system to recognize the cancer more effectively.
KEYNOTE-942 tested this plus pembrolizumab vs pembrolizumab alone in completely resected high-risk stage IIIB-IV melanoma.
Quick hits:
📌 Randomized phase 2b
157 patients
Intismeran pembrolizumab: n=107
Pembrolizumab alone: n=50
💉 Treatment
9 doses of intismeran Q3W
18 doses of pembrolizumab Q3W
📈 Recurrence-free survival
HR 0.510 (holy smokes)
49% reduction in recurrence or death
⏳ Overall survival
Favorable trend
HR 0.471
🔍 Biology matters
Greater expansion of novel clones was seen in patients without recurrence in the combination arm
⚠️ Safety
Manageable
No new safety signals at 5 years
This is melanoma, not GI.
But the concept matters across oncology.
We have spent decades giving systemic therapy in broad categories: chemotherapy, immunotherapy, targeted therapy.
This is finally something new.
The practical challenges are real: manufacturing, timing, cost, access, tissue quality, sequencing, and whether this works outside highly immunogenic tumors.
But a sustained 5-year signal on top of pembrolizumab is impossible to ignore.
When can we get these products in GI? I know there are studies running now in Pancreatic Cancer, but we’re waiting in Colorectal.
Also, if we could please come up with a different name than “vaccine”? Might help with funding and rollout in the future…
ascopubs.org/doi/10.1200/JCO…
@TheGutonclab @UGrewalMD @TimothyJBrownMD @OncoAlert @Onco_Nexus @ASCO
@NazliDizman @LauraAlderMD @DVAraujoMD @DrBarbiOnc @LauraEsfeller @FunchainMD @YGaritaonaindia @DrSAHaddad @jgong15 @iandresmeraz @SakditadMD @RamilaShilpakar @RohitBanwar @lungoncdoc
7
23
85
15,801
Gut Onc Lab retweeted

We have a pile of good stuff coming soon @TheGutOncLab
Jun 1

@TheGutOncLab 🤝 @Onco_Nexus
Live at #ASCO2026, the team got together to break down all of the exciting data updates from the meeting, key practice changing discussions across pancreatic, CRC, NET, Upper GI, and more. 🔬🎙️
Thank you to our outstanding guests @KReissMD & @adasarimd.
Keep an eye out for these episodes dropping soon 👀🔥
@GIMedOnc
@UGrewalMD
@TimothyJBrownMD
#ASCO




4
16
1,271
Gut Onc Lab retweeted
Jun 1
So glad to have had the opportunity to record live (first time for us) at #ASCO26
Looking forward to sharing these episodes with you all soon.
Jun 1
@TheGutOncLab 🤝 @Onco_Nexus
Live at #ASCO2026, the team got together to break down all of the exciting data updates from the meeting, key practice changing discussions across pancreatic, CRC, NET, Upper GI, and more. 🔬🎙️
Thank you to our outstanding guests @KReissMD & @adasarimd.
Keep an eye out for these episodes dropping soon 👀🔥
@GIMedOnc
@UGrewalMD
@TimothyJBrownMD
#ASCO
6
17
742
Gut Onc Lab retweeted

Jun 1
@TheGutOncLab 🤝 @Onco_Nexus
Live at #ASCO2026, the team got together to break down all of the exciting data updates from the meeting, key practice changing discussions across pancreatic, CRC, NET, Upper GI, and more. 🔬🎙️
Thank you to our outstanding guests @KReissMD & @adasarimd.
Keep an eye out for these episodes dropping soon 👀🔥
@GIMedOnc
@UGrewalMD
@TimothyJBrownMD
#ASCO
2
8
4,309