Gastrointestinal Medical Oncologist @Perlmutter_CC, Associate Program Director @nyulisom_HemOnc. Tweets my own. #Meded
- Tweets 1,433
- Following 238
- Followers 932
- Likes 337















ALT JAMA Oncology: Brief Report on Outcomes of Older Adults with Advanced Cancer preferring Quality of Life vs Prolonging Survival, a secondary analysis of the GAP70 Clinical Trial. Authors: Richardson, Wang, Flannery et al. Published March 5, 2026.

ALT https://academic.oup.com/oncolo/advance-article/doi/10.1093/oncolo/oyag194/8699602








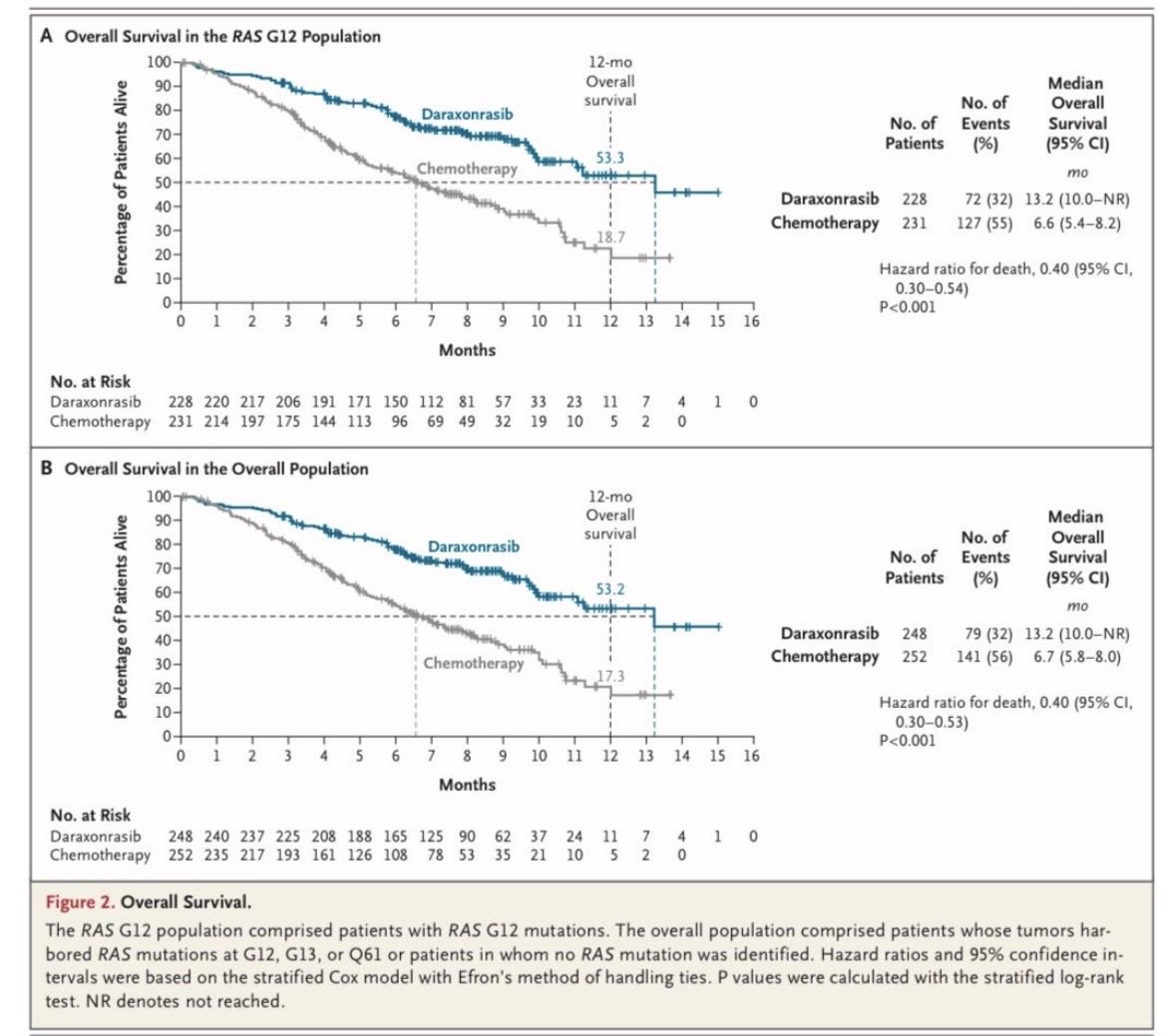





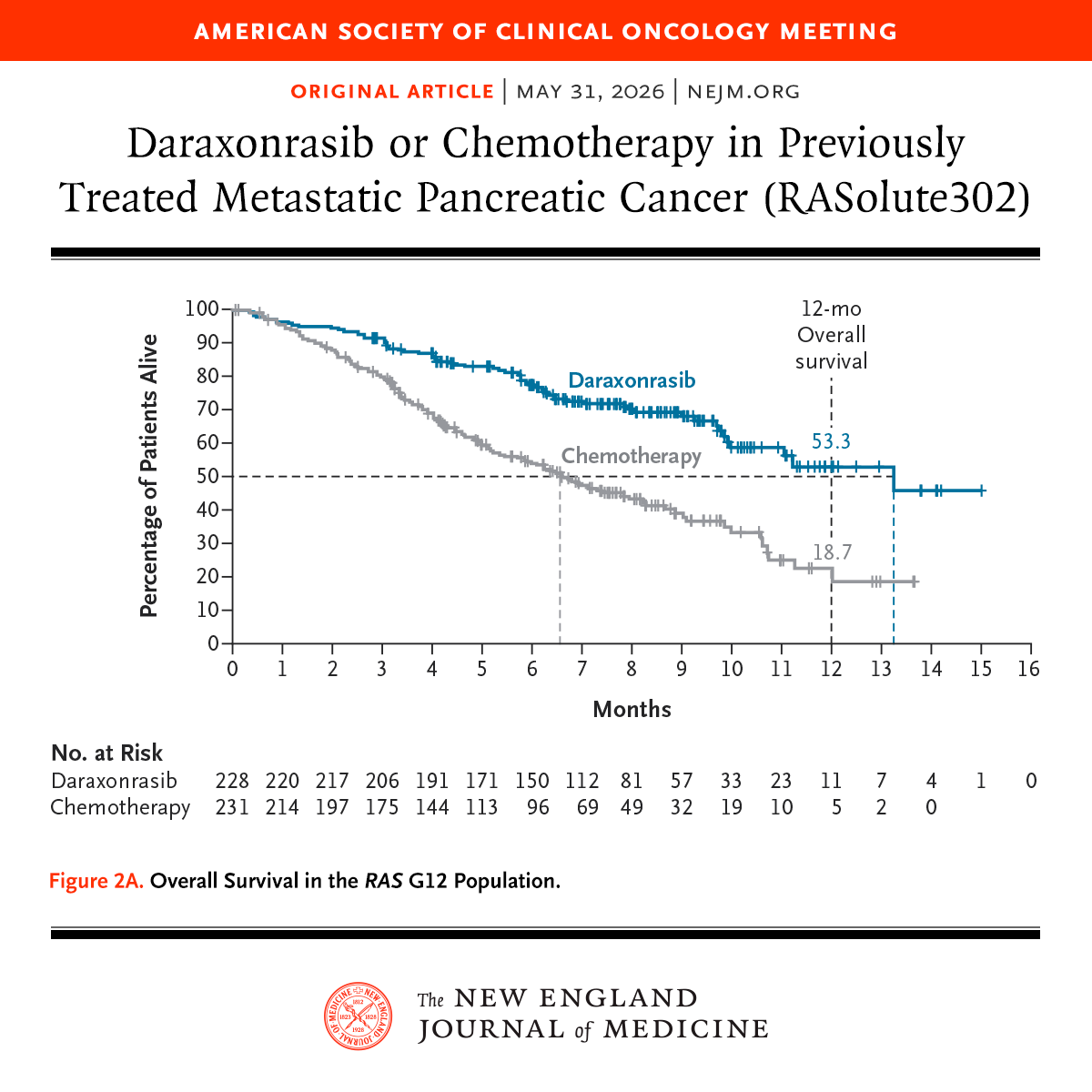
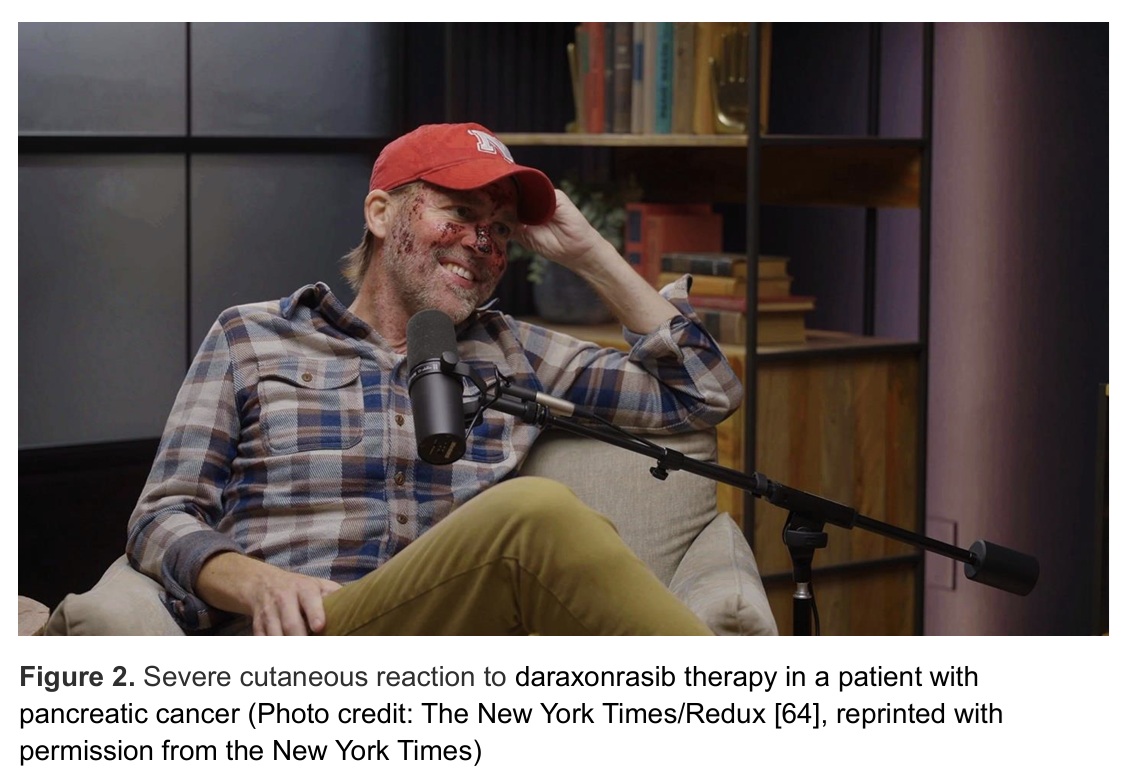
ALT Graph from a study published in the New England Journal of Medicine on daraxonrasib versus chemotherapy for metastatic pancreatic cancer. The x-axis represents months, and the y-axis shows the percentage of patients alive. Two lines indicate survival rates: daraxonrasib (blue) and chemotherapy (gray). The bottom section lists patients at risk over time. Title and journal logo are included.