
Joined April 2017
- Tweets 20,623
- Following 5,607
- Followers 1,316
- Likes 71,370
367 Photos and videos












Pinned Tweet

19 Nov 2020
“If we attend to the needs of the most vulnerable people, which we won't see unless we purposefully look, everyone has what they need.”
- seen on twitter
1
6
29
Health Services Mama🇨🇦🇺🇦 retweeted

Alberta, what do you get out of the $91,000,000, yes, $91 million referendum?
Nothing.
This $91 million could have been spent on building 3 schools, or 4 senior homes, or emergency rooms, hiring doctors or nurses.
Instead, you get nothing.
facebook.com/share/v/1Ayhqhs…
91
595
1,488
18,395
Health Services Mama🇨🇦🇺🇦 retweeted

Jun 11
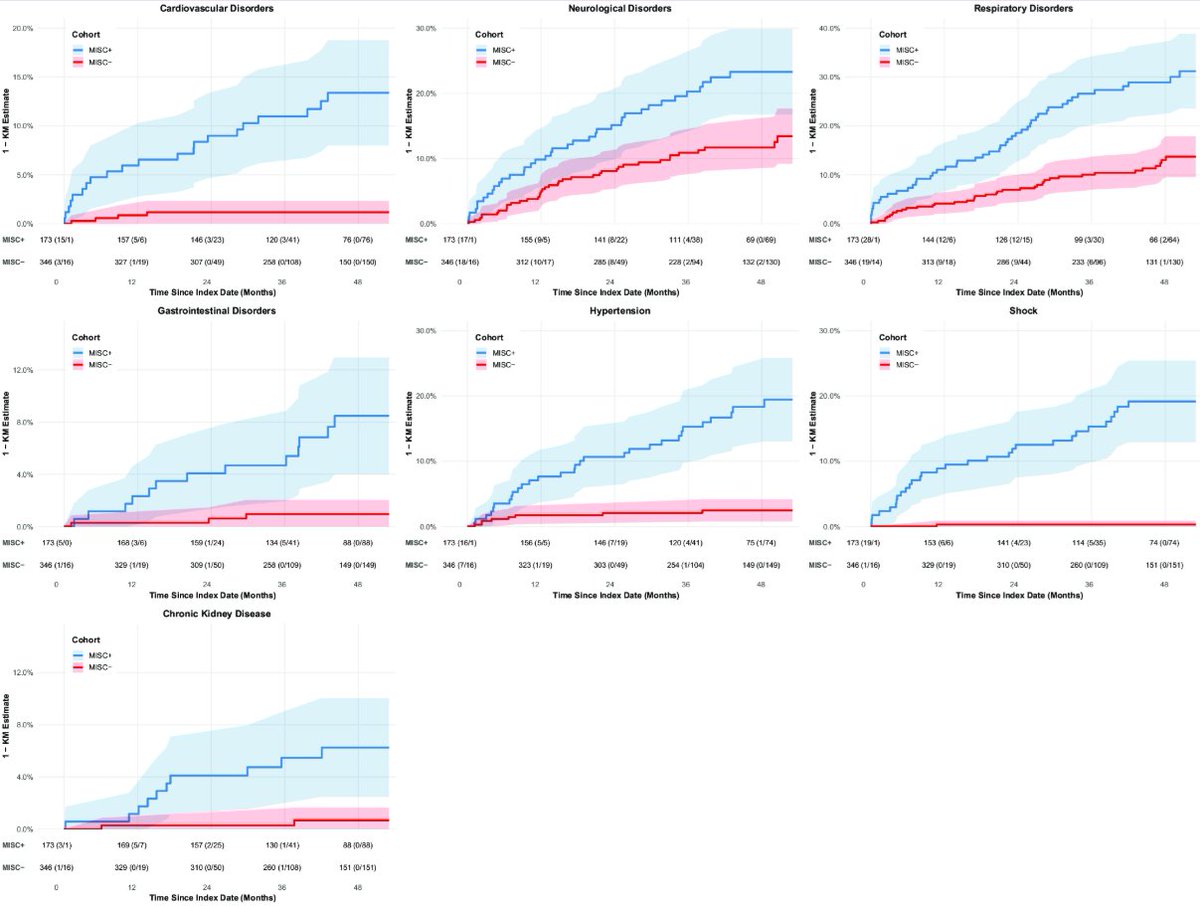
Long-Term Outcomes of Multisystem Inflammatory Syndrome in Children up to 4.5 Years After COVID-19
🚨IMPORTANT new study just dropped: MIS-C in kids is NOT a temporary illness!!
🚨It raises cardiovascular disease risk 14×, hypertension 9×, and gut/lung/brain problems for up to 4.5 years later(=LC)
Earlier “kids recover fine” claims are now officially challenged! Study:👇
➡️ A retrospective cohort study from New York’s Montefiore Health System examined 173 children under 21 with MIS-C versus 346 propensity score-matched controls without MIS-C, all following documented COVID-19 infection.
➡️Follow-up extended up to 4.5 years (March 2020–August 2024) using electronic health records, with MIS-C confirmed by ICD-10 code M35.81 plus CDC/WHO criteria.
➡️Results:
1. MIS-C patients faced markedly elevated risks compared to controls:
- Cardiovascular disorders (aHR 13.88, 95% CI 4.69–41.07),
- Hypertension (aHR 8.86),
- Gastrointestinal disorders (aHR 9.48),
- Respiratory disorders (aHR 3.46), and
- Neurological disorders (aHR 2.02),
- Shock and chronic kidney disease (CKD) occurred almost exclusively in the MIS-C group,
2. Kaplan-Meier analysis showed persistent cumulative incidence in the MIS-C cohort ranging from 6.8% (CKD) to 35.2% (respiratory disorders), with risks diverging and accumulating over years rather than resolving,
3. Preexisting hypertension strongly predicted cardiovascular, neurological, respiratory, and gastrointestinal outcomes,
4. Preexisting diabetes increased CKD risk 49-fold,
5. Older age modestly raised risks of shock and CKD.
6. Sensitivity analyses using stricter MIS-C definitions and alternative respiratory coding confirmed the main results.
7. No mention or data on vaccination and/or reinfection impact.
➡️The study directly challenges earlier reports portraying MIS-C as a transient, self-limited condition with minimal long-term sequelae.
‼️So, MIS-C is not a temporary inflammatory storm that children outgrow. It inflicts severe, lasting multisystem damage that multiplies the lifetime risk of serious cardiovascular disease, hypertension, gastrointestinal, respiratory, and neurological disorders by several-fold to more than ten-fold, while introducing rare but devastating conditions like shock and CKD that almost never occur in peers.
‼️Sadly enough risks continue to accumulate years later.
‼️Earlier short-term “excellent recovery” narratives are contradicted by this longer, rigorous evidence.
‼️Affected children now carry a heavy, potentially permanent burden of chronic illness that will require lifelong medical surveillance and coordinated care or face accelerated morbidity and reduced quality of life!
‼️Of course we need further confirmation, but this does fit the ongoing concerns within the LC science community!
😡So much for paediatric minimalizations!
#AvoidSars2 #AvoidReinfections #ProtectChildren
publications.aap.org/pediatr…
6
204
413
18,721
Health Services Mama🇨🇦🇺🇦 retweeted

Jun 10
When your government tells you; "we're all in the same boat!"
908
51,949
230,725
4,866,443
Health Services Mama🇨🇦🇺🇦 retweeted

Jun 10
You have noticed it. ChatGPT feels dumber than it used to. Your prompts that worked six months ago produce worse results now. The writing sounds flatter. The ideas sound safer. The internet itself feels like it is shrinking. Every article reads the same. Every email sounds the same. Every answer sounds like it was written by the same voice.
You thought it was you. It is not you.
Researchers at Oxford and Cambridge published a paper in Nature proving what is happening. They call it Model Collapse.
Here is the mechanism in one sentence. AI trained on AI-generated data gets dumber every generation until it forgets what real human data looked like.
The internet is filling with AI-generated content. Blog posts. Articles. Reviews. Comments. Social media. AI companies scrape the internet to train the next generation of models. Which means the next generation of AI is being trained on the output of the current generation.
Each cycle loses information. Not randomly. It loses the rarest, most unusual, most creative parts first. The researchers call these the "tails of the distribution." The weird ideas. The unexpected perspectives. The things that made the internet feel human. Those disappear first.
What remains is the average. The safe. The expected. The bland.
Then the next generation trains on that. And loses more. And the next generation trains on that. And loses more. The researchers proved this is not a slow decline. Major degradation happens within just a few iterations. Even when some of the original human data is preserved.
They tested it on large language models. On image generators. On statistical models. The pattern was the same every time. The output converges toward a narrow, flattened version of reality that looks nothing like the original data.
The lead researcher put it plainly. "Large language models are like fire. A useful tool. But one that pollutes the environment."
The pollution is invisible. You cannot see which sentence on the internet was written by a human and which was written by AI. Neither can the AI that is about to train on it. And once the tails are gone, they do not come back. The damage is irreversible.
This is not a prediction anymore. It is a diagnosis.
The internet you grew up on was built by humans writing things no algorithm would have written. Strange, personal, imperfect, alive. That internet is being diluted. One generation of AI at a time. And the models trained on what remains are learning a smaller and smaller version of the world.
Model Collapse is not a technical problem. It is a cultural one. The thing that made the internet worth reading is the thing that disappears first.

1,138
6,387
17,719
2,230,412
Health Services Mama🇨🇦🇺🇦 retweeted

Jun 9
A neuroscientist at UC Irvine spent 60 years proving that your brain has a separate memory system for emotional events, and you can hack it to remember almost anything you want.
His name is James McGaugh.
He founded the Center for the Neurobiology of Learning and Memory at the University of California, Irvine, and he has been running experiments on how the brain decides what to keep and what to throw away since 1959. The finding he spent his entire career building, refining, and defending should change how every person on Earth thinks about learning.
The discovery started with a question almost nobody else was asking in the early 1960s. Why is it that you can read an entire textbook chapter and remember almost nothing three days later, but you can recall in vivid detail what you were doing the moment you heard a piece of devastating news from years ago.
The two memories were stored by the same brain in the same skull, and yet one was almost completely erased while the other was preserved frame by frame. McGaugh was convinced that something specific had to be happening in the brain to explain the gap, and he spent the next six decades chasing it.
The first major piece of evidence came from a simple animal experiment that almost ended his career when he proposed it. He trained rats to perform a task, and then immediately after the training he injected them with a stimulant drug. The rats who received the injection remembered the task far better than the rats who did not, even though both groups had performed identically during the actual learning.
The drug had not made the rats smarter or faster. It had been administered after the learning was over. Something about the chemical state of the brain in the minutes following a learning event was determining whether the memory survived or vanished.
This was the moment the entire field of memory consolidation was born. McGaugh had proven, against decades of consensus, that memories are not formed at the moment of the experience. They are formed in the hours that follow, and the chemical environment of the brain during that consolidation window decides what gets kept.
The next 50 years of his lab's work mapped out exactly which chemicals were doing the work. The answer turned out to be the stress hormones your body releases when something emotionally significant happens. Epinephrine. Cortisol. And most importantly, a neurotransmitter called norepinephrine, which floods a specific part of your brain called the basolateral amygdala the moment you feel anything strongly.
The amygdala is the small almond-shaped structure deep inside your brain that processes emotion.
McGaugh and his colleagues proved that when this region is activated by emotion, it sends a signal to the hippocampus, which is the brain region responsible for forming new memories, and that signal physically strengthens the consolidation of whatever you were experiencing in that moment.
Emotionally charged events get stamped into the brain with a flood of hormones that say keep this. Neutral events get filed without the stamp and are quietly thrown away over the next few days.
The experiment that made the mechanism unmistakable was published in 1994 by McGaugh's collaborator Larry Cahill, who had trained at the same lab. He showed participants a series of slides that told a story. Half of them saw a neutral version of the story where a boy and his mother visited a hospital.
Half of them saw an emotional version where the boy was hit by a car and rushed to the same hospital. The slides were almost identical. The narration was different.
Two weeks later, the participants were brought back and tested on how much they remembered. The emotional group recalled the middle of the story, where the trauma happened, with significantly higher accuracy than the neutral group recalled the same middle slides. The story was the same. The images were the same. The only thing that had changed was whether the brain was emotionally activated while encoding the information.
Then Cahill ran the experiment again. This time he gave half the emotional group a drug called propranolol, which blocks the action of norepinephrine in the amygdala. The drug did not interfere with their thinking. It did not make them sleepy. It just shut down the chemical pathway McGaugh had spent decades mapping. And the emotional memory advantage disappeared completely.
The group on propranolol remembered the emotional story no better than they remembered the neutral one. The hormone was the difference. Block the hormone, and the brain stopped stamping the memory.
This is the framework McGaugh built over 60 years. The brain has a two-track memory system. The default track is for neutral information, and it is leaky on purpose because most of what your brain processes in a given day is not worth keeping.
The emotional track is for information that arrives with a chemical signal that says this matters, and it preserves the experience with stunning detail because evolution decided that anything emotionally significant was probably important for survival.
The implication is the part almost nobody talks about, and it is the reason this research should be on the wall of every classroom and study room.
If you want to remember something, you have to give your brain a reason to flip the emotional switch on while you are learning it. Information delivered in a flat, neutral, low-stakes environment will be processed through the leaky default system regardless of how many times you re-read it. Information delivered with curiosity, surprise, stakes, embarrassment, awe, or even mild stress will be processed through the emotional system, and the same brain will hold onto it for years.
This is why the lecture you were forced to sit through evaporated by the end of the week, while the question you got humiliated by in front of the class is still perfectly preserved 15 years later. The humiliation was the chemical stamp. The lecture had none.
People who remember enormous amounts of what they read are not gifted. They are emotionally engaged with the material in a way most learners never become. They argue with the author in the margins. They feel actual frustration when something does not make sense. They get genuinely excited when a concept clicks. The frustration and the excitement are not side effects of learning.
They are the mechanism of learning. Every emotion you feel while reading is a small dose of norepinephrine being released into the amygdala, telling the hippocampus to stamp this page into long-term storage.
The fix is almost embarrassing in its simplicity.
Stop trying to absorb information neutrally. Pick a question you actually care about answering before you open the book. Argue with the material as you read it. Get angry at the parts that feel wrong. Get curious about the parts that surprise you. Try to explain what you learned to someone who would push back on it. Care about the outcome.
Your brain was never designed to remember neutral information. It was designed to remember anything that made you feel something. McGaugh spent 60 years proving that the rest is almost a rounding error.
The voice in your head that tells you to study harder is wrong.
The one that tells you to study warmer is the one your brain actually listens to.

13
165
545
21,411
Health Services Mama🇨🇦🇺🇦 retweeted

Jun 8
The anatomical proximity and direct connection between the olfactory bulb and the orbital prefrontal cortex (OFC) make it a key neuroinvasion route for #COVID in the brain. In patients with #NeuroCovid, we observe thrombotic events, hypometabolism and atrophy in this region.



21
283
767
29,814
Health Services Mama🇨🇦🇺🇦 retweeted

Jun 8
I know I've said this many times before on this platform, but the moment I learned anosmia was a symptom of Covid-19 was the moment I decided I was going to do everything possible to avoid getting it. I knew anosmia was an early prodromal symptom of Parkinson's Disease.

Could #LongCOVID be leaving behind early fingerprints of Parkinson’s disease?
➡️ In a 16-country study of >11,000 participants, people with LongCOVID showed significantly higher rates of multiple prodromal Parkinson’s-like features—including loss of smell, constipation, daytime sleepiness, dizziness, cognitive problems, urinary symptoms, depression, and dream-enactment behaviors. 1/

32
498
1,652
56,423
Health Services Mama🇨🇦🇺🇦 retweeted

65 Candles 🎂 today for the wonderful & inspirational MICHAEL J. FOX

427
2,224
33,527
286,667
Health Services Mama🇨🇦🇺🇦 retweeted
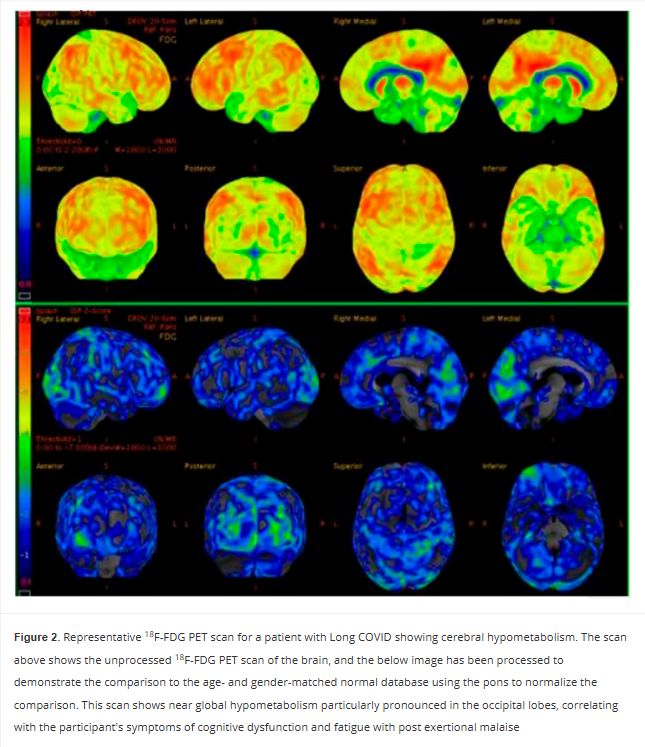
Persistent Cerebral 18-FDG PET Changes in Patients With Long COVID Presenting With Fatigue and Post Exertional Malaise
🚨We already knew Long COVID brain damage could last 6 months.
Now this new PET scan study proves it’s still there at 2 YEARS and counting.
Hypometabolism hits the left sensorimotor cortex (movement body sense), left superior parietal (spatial awareness attention), and bilateral visual cortex (raw sight processing).
This is NOT just “tired.”
This is a broken sensory-motor command center.
Is this the start of a lifelong neurological disease?
➡️Mayo Clinic observational cohort study of 40 Long COVID patients (70% female, median age 53) from a specialized clinic who underwent brain 18F-FDG PET-CT scans 17–149 weeks (median 62 weeks) after SarsCoV2 infection,
➡️73% had predominant fatigue with post-exertional malaise (PEM),
➡️This group showed statistically significant cerebral hypometabolism vs. non-PEM patients in the left sensorimotor cortex (p=0.0253), left superior parietal cortex (p=0.0276), and bilateral primary visual cortex (p=0.0096 and 0.0016),
➡️Abnormalities persisted already up to ~2 years post-infection,
➡️Scans used pons-normalized Z-scores against age/gender-matched controls with common comorbidities included psychiatric, GI, and cardiovascular conditions,
➡️Caveat: No references to vaccination status and/or reinfections,
➡️Authors propose 18F-FDG PET-CT as a potential diagnostic and therapeutic biomarker for the fatigue/PEM phenotype of Long COVID.
‼️So, AGAIN, Long COVID fatigue and PEM have a demonstrable, persistent neurological signature! Cerebral hypometabolism, still detectable on PET scans up to two years later and hits the left sensorimotor cortex (movement body sense), left superior parietal cortex (spatial awareness attention), and bilateral primary visual cortex (raw sight processing).
This isn’t just “tired.”
It’s a broken sensory-motor command center.
😡Study proves LC is biologically real, not psychosomatic or any other stupid FND diagnosis.
Without urgent validation of this biomarker and targeted therapies, patients will continue to be dismissed despite objective brain damage!
#AvoidSars2 #AvoidReinfections #BrainDamage
journals.sagepub.com/doi/10.…
23
276
620
26,370
RT @JoannaTeglund: 1. If you are curious how much COVID—regardless of severity—increases the risk of mental disorders, this study is for yo…
174
Health Services Mama🇨🇦🇺🇦 retweeted

And BTW, I arrived at the Nanaimo Regional General Hospital at 2:30. In X-ray within 15 minutes.
Seen by a doctor at 3:50 with X-ray results.
Cast applied by two other doctors at 5:30.
Prescription for pain relief in my hand at 5:45.
Home by 6:30.
@ABDanielleSmith @UCPCaucus
You should all take a lesson from @Dave_Eby
This is how it’s done.


155
161
933
30,385
Health Services Mama🇨🇦🇺🇦 retweeted

Jun 8
FINALLY:
📌A landmark MRI study published in Heart Rhythm reveals that individuals with Postural Orthostatic Tachycardia Syndrome (#POTS) exhibit structural brain tissue changes, impaired central autonomic network function, and reduced cerebral blood flow during cardiovascular stress. These neurological deficits directly explain symptoms like cognitive "brain fog". [1, 2, 3]
📌Key Findings
•Structural Brain Alterations: MRI scans show clear differences in the central autonomic network (e.g., in regulatory sites like the insula) compared to healthy individuals. [1, 2]
•Cerebral Hypoperfusion: There is a significant reduction in blood flow to critical brain regions during cardiovascular reflex tests, emphasizing that this is a neurological issue, not just a heart rate problem. [1, 2]
•Autonomic Dysfunction: Impaired central neural responses prevent the brain from properly regulating the autonomic nervous system, triggering cardiovascular dysreflexia upon standing. [1]
📌Why This Matters
For years, many patients struggling with POTS have had their symptoms dismissed as anxiety or "all in their heads". This neuroimaging research validates patient experiences by identifying objective, measurable biomarkers in the brain. It establishes that central autonomic control deficits are central to POTS.
STUDY LINKED BELOW🔻
10
232
727
16,249
Health Services Mama🇨🇦🇺🇦 retweeted

#ableg
Alberta’s referendum will cost $90,000,000 of YOUR money!
🦴 7,500 hip surgeries
👨⚕️ 321 family doctors
🏥 15 rural medical centres
♿ $200/mo top-up for 37,500 AISH recipients
Instead…The UCP Alberta clawed back $200/mo from 77,000 disabled citizens
Thanks Danielle!


How much will the referendum on having a referendum, and on 9 questions that can’t be provincially implemented cost?
$90 million tax dollars. 60,000 workers to be hired by Elections Alberta.
You could build 3 schools for that.
That’s your money
#ableg elections.ab.ca/resources/me…
22
303
515
13,409
Health Services Mama🇨🇦🇺🇦 retweeted

I'm a cardiologist. A 42-year-old mother of two came to my office complaining of jaw pain and crushing fatigue. She ran half-marathons. Her EKG was normal. Another doctor had sent her home with anxiety medication.
When I got her into the cath lab, I found severe microvascular disease — plaque choking the tiniest vessels of her heart, the ones standard angiograms routinely miss.
Her heart had been starving in silence while everyone told her she was stressed.
She is alive today. Too many women like her are not.
Heart disease kills more women than every cancer combined. And medicine is still diagnosing it through a male lens.
84% of cardiologists report having patients in the past year whose heart disease was misdiagnosed by another physician. Women with a STEMI heart attack have a 59% greater chance of being misdiagnosed compared to men. Women with an NSTEMI — 41% greater chance.
The reason is structural. For decades, we screened, tested, and treated women using a template built for men.
Men's heart attacks announce themselves — the crushing chest pain, the clutched fist, the Hollywood collapse. Women's hearts whisper. Crushing fatigue that feels like wearing a lead vest. Jaw pain written off as TMJ. Nausea blamed on a stomach bug. An ache between the shoulder blades blamed on a long week. Shortness of breath blamed on being out of shape.
For years, medicine called these "atypical" symptoms. They are not atypical. They are female-typical. Half of humanity is not a variant.
And the biology runs deeper than symptoms.
Women have smaller hearts and narrower coronary arteries. Plaque doesn't only clog the big highway vessels — it hides in the microvasculature, the tiny branches feeding the heart muscle itself. A woman can have a heart attack with a completely "clean" standard angiogram.
SCAD — spontaneous coronary artery dissection — occurs 90% of the time in women. Often young, fit women with zero traditional risk factors. It's the leading cause of heart attack in women under 50, accounting for roughly one quarter of all cases in that age group. Most doctors have never diagnosed one.
And some of the most dangerous cardiac risk factors are hidden in women's medical histories where no one thinks to look:
Preeclampsia or gestational hypertension doubles to quadruples lifetime heart disease and stroke risk. Pregnancy is the body's first cardiac stress test — and these complications are early warning sirens, not closed chapters.
Autoimmune disease — lupus, rheumatoid arthritis, psoriasis — far more common in women, turbocharges inflammation and plaque formation at any age.
Cardiovascular disease in women aged 20-44 is projected to surge nearly 50% by 2050.
The youngest patients in my practice keep getting younger.
What every woman should ask her doctor — and what every doctor should be asking:
"Given my pregnancy history, autoimmune status, and family history — what is my full cardiovascular risk?" If they don't ask about preeclampsia or gestational diabetes, volunteer it.
"Should I have an Lp(a) test and a coronary calcium score?" Standard cholesterol panels miss too much. Lp(a) is genetic, one-time, and most women have never been tested.
"My tests came back normal but my symptoms haven't stopped — what's next?" Normal stress tests and angiograms can miss microvascular disease, spasm, and SCAD. Persistent symptoms warrant coronary CT angiography or cardiac MRI.
And if something feels wrong — say these exact words to your doctor: "I am concerned this could be my heart."
That single sentence changes the workup. Do not soften it. Do not apologize for it.
80% of heart disease is preventable. But the playbook has to be built for female biology.
Two decades ago, I wrote one of the first books warning that heart disease was the number one killer of women and that medicine was diagnosing it through a male lens. It was recognized by First Lady Laura Bush at the White House during the early years of the national conversation about women's heart health.
I'm haunted by how much of that book I could republish today unchanged.
The science has advanced. The awareness has grown. But the gap between what we know and what happens in the exam room is still costing women their lives.
Share this with every woman you love — and every doctor who treats them. READ MORE: open.substack.com/pub/afshin…
179
2,659
6,620
766,913
Health Services Mama🇨🇦🇺🇦 retweeted

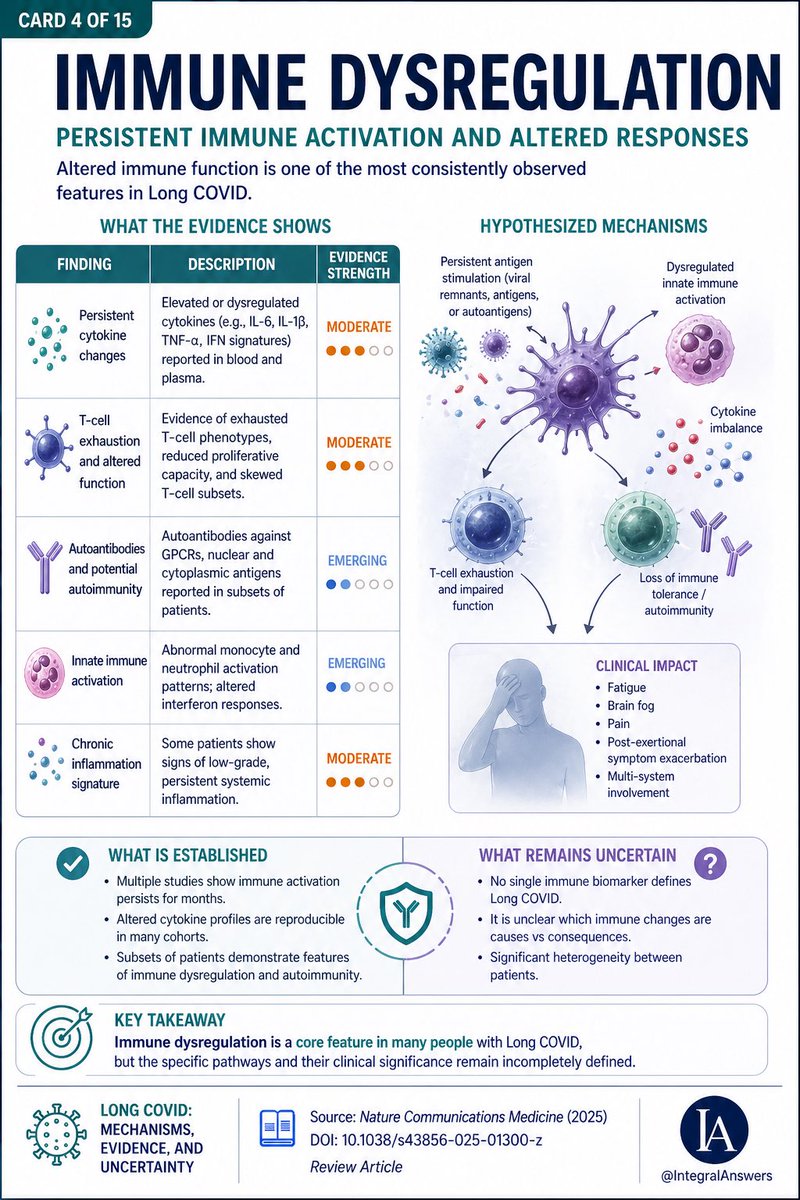
4/ Immune dysfunction is one of the strongest signals.
Findings include:
→ Persistent inflammatory signaling
→ T-cell exhaustion
→ Possible autoimmunity
But:
No single immune signature defines all patients.
2
37
162
3,146
Health Services Mama🇨🇦🇺🇦 retweeted
There are plenty of world-class L0ngC0vid experts far smarter than I am.
But I bring something they don’t: I’m a CV surgeon and endovascular specialist. I’ve had hearts, lungs, arteries, and other organs literally in my hands. I’ve seen their insides, healthy and ravaged, with my own eyes.
That gives me one brutal, irreplaceable edge: I can take the science and translate it straight into the living, bleeding reality of human anatomy.
And what I see coming is ugly.
You, personally and as a society, are in for one hell of a shock.
Read this 🧵👇
If you keep minimising SARSCoV2, refuse to protect yourselves, and keep swallowing the lies of pseudo-experts chasing money or psychiatrists salivating over a fresh FND goldmine… you’re walking straight into disaster.
Tell every last one of them to f.ck off!
Then follow the hard, unfolding science.👇
Your organs don’t care about opinions. They only care about damage. And the damage is already stacking up, be it momentarily maybe still clinically "silent"! #AvoidSars2 #AvoidReinfections

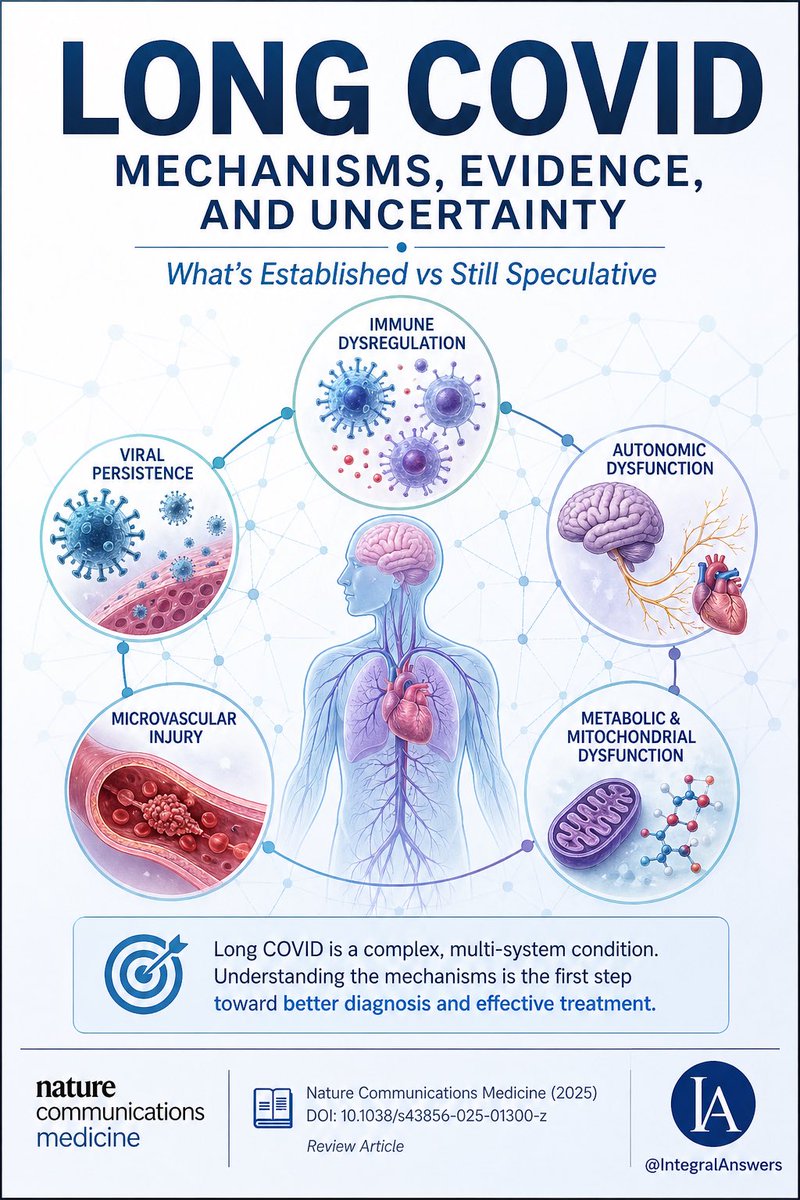
1/ Long COVID is one of the most complex post-infectious syndromes ever studied.
A new review in Nature Communications Medicine attempts to unify the biology.
Here’s what’s established, what’s emerging, and what’s still speculative. 🧵
38
507
1,126
34,769
Health Services Mama🇨🇦🇺🇦 retweeted

Jun 6
i took a 45-minute uber ride home from the airport last night after a brutal, three-day business trip.
i was completely emotionally and physically drained, and my social battery was at absolute zero.
when i got into the car, the driver.. an older guy named kabir.. didn't say the usual "how was your flight?" or turn on the radio.
instead, he just handed me a small, laminated piece of paper attached to the back of his headrest.
it was a literal "ride menu."
it said:
1. *the silent ride* (total quiet, no pressure to talk).
2. *the therapist ride* (if you need to vent about your day, i am listening).
3. *the tourist ride* (i will tell you cool facts about the city).
4. *the radio ride* (we just listen to old jazz and coast).
i smiled, pointed to number 1, and whispered, "silent ride, please. thank you."
he gave me a warm nod in the rearview mirror, adjusted the AC, and drove the entire 45 minutes in absolute, beautiful silence.
it was the most peaceful, therapeutic boundary i’ve experienced all year. i felt my entire nervous system finally reset.
when he dropped me off, i gave him a massive tip and told him, "that menu is a genius business idea. you must get amazing reviews."
He looked back at me and said, "i didn't make the menu to get better tips, dear.
my daughter has severe social anxiety, and she told me that the hardest part of her day is navigating small talk with strangers when her brain is tired.
she told me it feels like running a marathon.
i made the card so that anyone who gets into my car can feel completely safe dropping the mask for a little while."
i walked into my apartment and just sat on my suitcase.
we live in a world that is constantly screaming at us to perform, to network, to be "on," and to over-communicate.
but sometimes, the deepest form of love and respect you can show another human being is just creating a small, safe pocket of silence for them to rest in.
pay attention to the people who give you permission to be quiet. they are rare.
148
2,339
12,298
262,745
Health Services Mama🇨🇦🇺🇦 retweeted

May 25
A friend passed this to me, saying it might be helpful - it's about getting help on Long Covid from your GP, it's for a UK setting, but some of it will be applicable anywhere - read the note at the end for more too.
"I work in AI. I used it to research and write my mum a letter about her Long COVID. Her GP called her the next day after 3 years of being dismissed!
*Reposting here as myself since it blew up in another support group and people really want help with this… feel free to add/DM me.*
So I work in AI, specifically in healthcare tech. So when my mum had been fobbed off by her GP for the third year in a row about her Long COVID, I figured I should actually do something useful with what I know.
This isn't about gaming the system or bending rules. Everything I'm sharing here is publicly available on NHS and government websites. I just used AI to find it, understand it, and turn it into something a GP couldn't easily brush off.
Here's what most people don't know. The NHS publishes detailed guidelines that GPs are expected to follow. NICE published a specific Long COVID guideline called NG188 that sets out exactly what a GP has to do when a patient comes to them with ongoing post-Covid symptoms. Most patients have never heard of it. Most GPs don't follow it unless someone pushes them on it.
The other thing most people don't know: verbal dismissal is easy to ignore. A formal written letter that references specific guidelines creates a paper trail. The GP now has a documented duty of care they're expected to respond to. It genuinely changes everything.
My mum is 61. Not remotely tech savvy. She would never have found any of this herself. I spent about 20 minutes using AI to pull the relevant guidelines, match them to her situation, and draft a letter. She sent it to her GP by email on a Tuesday. Her GP called her on Wednesday afternoon. First time in three years a GP had called her. She now has a referral to a Long Covid clinic and a written management plan, after years of being told it was probably anxiety or just her age.
Posting her letter below with her details redacted. Copy it, adapt it to your situation, send it by email not in person. You need a timestamp. You need a record. That's what actually forces a response.
───
[Her letter, personal details redacted]
████████████████
████████████████
████████, ██████
██ ██████ 2025
Dr ████████████
████████████ Surgery
████████████████
████████, ██████
Re: Formal written request for Long COVID assessment and personalised management plan
Dear Dr ████████,
I am writing to formally request appropriate assessment and management for post-COVID-19 syndrome (Long COVID), and to create a written record of this request for my medical file.
I contracted COVID-19 in ████████ 2022 and have experienced the following ongoing symptoms for over three years:
• Severe fatigue and post-exertional malaise, symptoms worsen significantly following any physical or cognitive exertion
• Cognitive dysfunction, difficulty with memory, concentration, and word retrieval
• Breathlessness disproportionate to exertion
• Heart palpitations and episodes of tachycardia
• Disrupted sleep despite significant fatigue
• Generalised pain and joint discomfort
These symptoms have substantially impaired my ability to work, maintain daily activities, and quality of life.
CLINICAL BASIS FOR THIS REQUEST
NICE guideline NG188, COVID-19 rapid guideline: managing the long-term effects of COVID-19, was developed jointly by NICE, SIGN and the Royal College of General Practitioners. It applies to any patient with new or ongoing symptoms four or more weeks after acute COVID-19.
Under NG188 section 5.2.1, GPs are expected to use a multidisciplinary approach to guide rehabilitation, including physical, psychological and psychiatric aspects of management.
Under NG188 section 5.2.2, GPs must work with the patient to develop a personalised rehabilitation and management plan, which must be recorded in writing. NICE states explicitly that healthcare professionals are expected to take this guideline fully into account. This is not optional guidance.
Under GMC Good Medical Practice (2024), where a GP cannot adequately manage a patient's condition, they are required to refer to a specialist with the relevant expertise.
Under the NHS Constitution, I have the right to be referred to an appropriate specialist where my GP is unable to provide the required clinical management.
I have not received a personalised management plan or specialist referral in three years of presenting with these symptoms.
WHAT I AM FORMALLY REQUESTING
1. A holistic clinical assessment consistent with NICE NG188, including physical, psychological and functional domains
2. A personalised rehabilitation and management plan recorded in writing, as required under NICE NG188 section 5.2.2
3. Referral to the Long COVID clinic or appropriate multidisciplinary rehabilitation service
4. A written response to this letter within 14 days
I would like this letter to be added to my medical record. I am not requesting anything outside published NHS guidelines. I am asking for what those guidelines state I am entitled to receive.
Yours sincerely,
████████████████
Date of birth: ██/██/████
NHS number: ███ ███ ████
Based on: NICE NG188 (January 2024) | GMC Good Medical Practice (2024) | NHS Constitution (2023)
*Verify current guidelines at nice.org.uk before sending.*
───
Same approach works for basically any condition where you're being dismissed. MCAS (I am currently writing myself a letter to escalate my own issues with this), fibromyalgia, EDS, POTS, chronic fatigue. The escalation pathways exist for all of them, most people just don't know how to use them.
If it’s useful I could build a tool that does this automatically for you. You answer a few questions about your condition, it finds the relevant guidelines and drafts the letter for you. If that sounds useful, DM me or comment. Happy to write one manually for anyone in the meantime.
Not medical advice! Keep seeing your GP. Call 111 if anything gets worse."
27
182
475
11,906
Health Services Mama🇨🇦🇺🇦 retweeted
May 25
L0NG C0VID IS QUIETLY WRECKING HEARTS.
Maybe time for a recap based on 2026 science.
Here’s the comparison for MACE, Stroke, Deadly Clots & overall CV risks:
➡️MACE (heart attack, stroke, heart failure)
• Non-COVID: HR 1.0
• COVID-19: 1.8–3.9x
• Long COVID: ~4.5x
➡️Stroke (ischemic):
• Non-COVID: HR 1.0
• COVID-19: ~2–3x
• Long COVID: ~3.5x
➡️Deadly clots (PE / VTE):
• Non-COVID: HR 1.0
• COVID-19: ~2–4x
• Long COVID: 3.2–4.4x
➡️Overall CV risks:
• Non-COVID: baseline
• COVID-19: ↑1.5–2.5x (arrhythmias, CAD, HF)
• Long COVID: 2–4.5x higher
Long COVID adds extra danger beyond regular post-COVID.
Risks hit even non-hospitalized patients and last for years.
Vax may reduce risks but certainly doesn’t erase it.
Absolute risks lower in young/healthy, but serious if older/comorbid.
‼️Today’s evidence shows that while any COVID-19 infection elevates cardiovascular risks, long COVID dramatically amplifies them, making proactive heart monitoring essential for affected patients.
Bottom line: Get your heart checked post-Covid19/ LongC0vid and #AvoidSars2 #AvoidReinfections!
🚨C0VID-19/L0NG C0VID are serious CV RISK FACTORS!
11
247
551
24,297
Health Services Mama🇨🇦🇺🇦 retweeted

May 21
Bruce Springsteen appeared on Stephen Colbert’s show tonight and COOKED Trump and his goons
“I’m here in support tonight for Stephen, because you are the first guy in America who lost his show because we got a president who can't take a joke…. and because Larry and David Ellison feel they need to kiss his ass to get what they want. Stephen, these are small minded people. They got no idea what the freedoms of this beautiful country are supposed to be about”
3,710
15,025
75,349
2,368,979