
Medical Director Urologic Oncology/GU Cancers. Mary Bird Perkins Cancer Center. Metairie, Louisiana. Bladder and Prostate Cancer subspecialty.
Joined April 2014
- Tweets 2,413
- Following 991
- Followers 1,894
- Likes 10,916
293 Photos and videos










Pinned Tweet

Radical Cystectomy shouldn't be the only conversation after EV-Pembro.
3
8
45
4,132
Scott E Delacroix Jr M.D. retweeted

Here is a look at @USAPrimeBSB_HTX 16U Elite's Ben Chapin (@benchapin2028) on the mound this morning. The RHP was efficient, throwing 3 innings, striking out 3 batters, and allowing no hits or runs.
St. John's (TX) 2028 #uncommitted
Profile: fivetool.org/players/7831a9d…
3
8
1,122
Scott E Delacroix Jr M.D. retweeted

Was great to chat with @l_ballas, who had many interesting questions beyond what we had time for @APCCC_Lugano. Loved the meeting. Loved the interview discussion @urotoday. Love working with smart people to make care better for our patients!
#APCCC26
May 26

Debating prostate radiotherapy for metastatic hormone-sensitive #ProstateCancer. @TylerSbrt7 @UCSanDiego joins @l_ballas @CedarsSinai outlining his approach to radiation therapy for the primary tumor in metastatic hormone-sensitive prostate cancer. He summarizes three randomized trials that consistently show a progression-free survival benefit, particularly in patients with low-volume metastatic disease. #WatchNow on UroToday > bit.ly/4t9XGaq @APCCC_Lugano #APCCC26
4
13
1,827
Scott E Delacroix Jr M.D. retweeted

People have been DM and asking me: with an HR of 0.68 for durvalumab BCG in POTOMAC, why isn’t this for every high-risk NMIBC patient?
Here’s how hazard ratios work – and why they can mislead you if you stop there. 🧵 #ASCO26
@tompowles1 @WesKassouf @shilpaonc @DrFelixGuerrero

The approval answers one question, but leaves another unanswered: which patients truly derive enough benefit to justify escalation beyond optimized BCG?
The FDA approval of durvalumab plus BCG in high-risk NMIBC was driven by a meaningful improvement in disease-free survival (HR 0.68), mainly recurrence free survival. Checkpoint inhibitors are not benign therapies, carrying ~ 15% risk of serious treatment-related adverse events.
At the same time, this trial also demonstrated that patients with BCG-naïve high-risk NMIBC have low rates of progression and bladder cancer mortality, when treated with BCG appropriately.
For many patients, the balance between reducing recurrence and exposing them to potentially significant toxicity is not straightforward.
That raises a practical question: who should actually receive treatment intensification?
5
16
38
8,371
Scott E Delacroix Jr M.D. retweeted

May 20
36 years of loyal service and more cold beers than we could count.
RIP to a garage legend 🍻
32
42
1,336
431,411
Scott E Delacroix Jr M.D. retweeted

May 20
Today on Clinical Trials Day, we honor patients, researchers & professionals advancing cancer care. Every study brings new hope. Thanks to all for helping to move oncology research forward. #ClinicalTrialsDay #CTD2026 #ResearchRising

5
10
386
Scott E Delacroix Jr M.D. retweeted
May 19
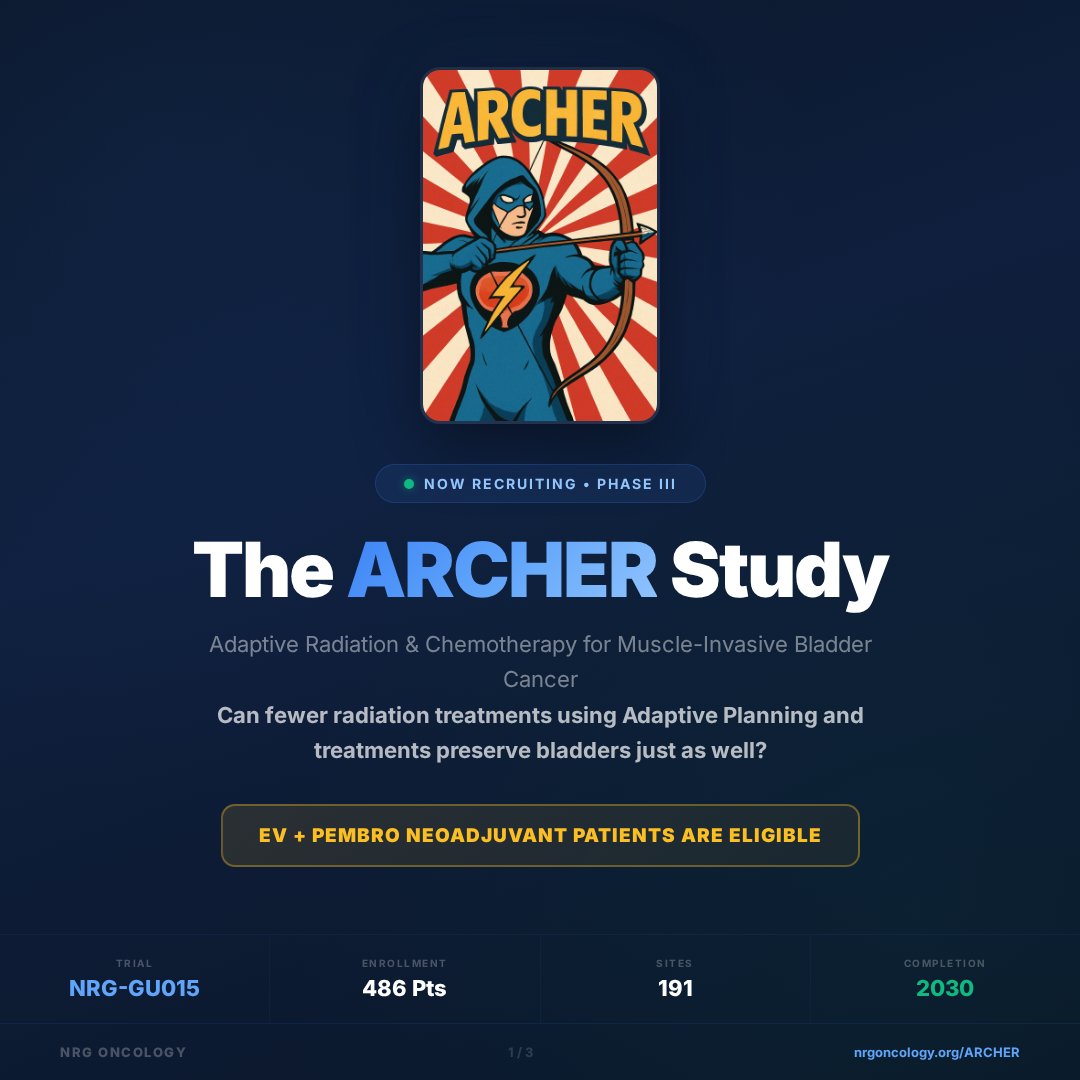
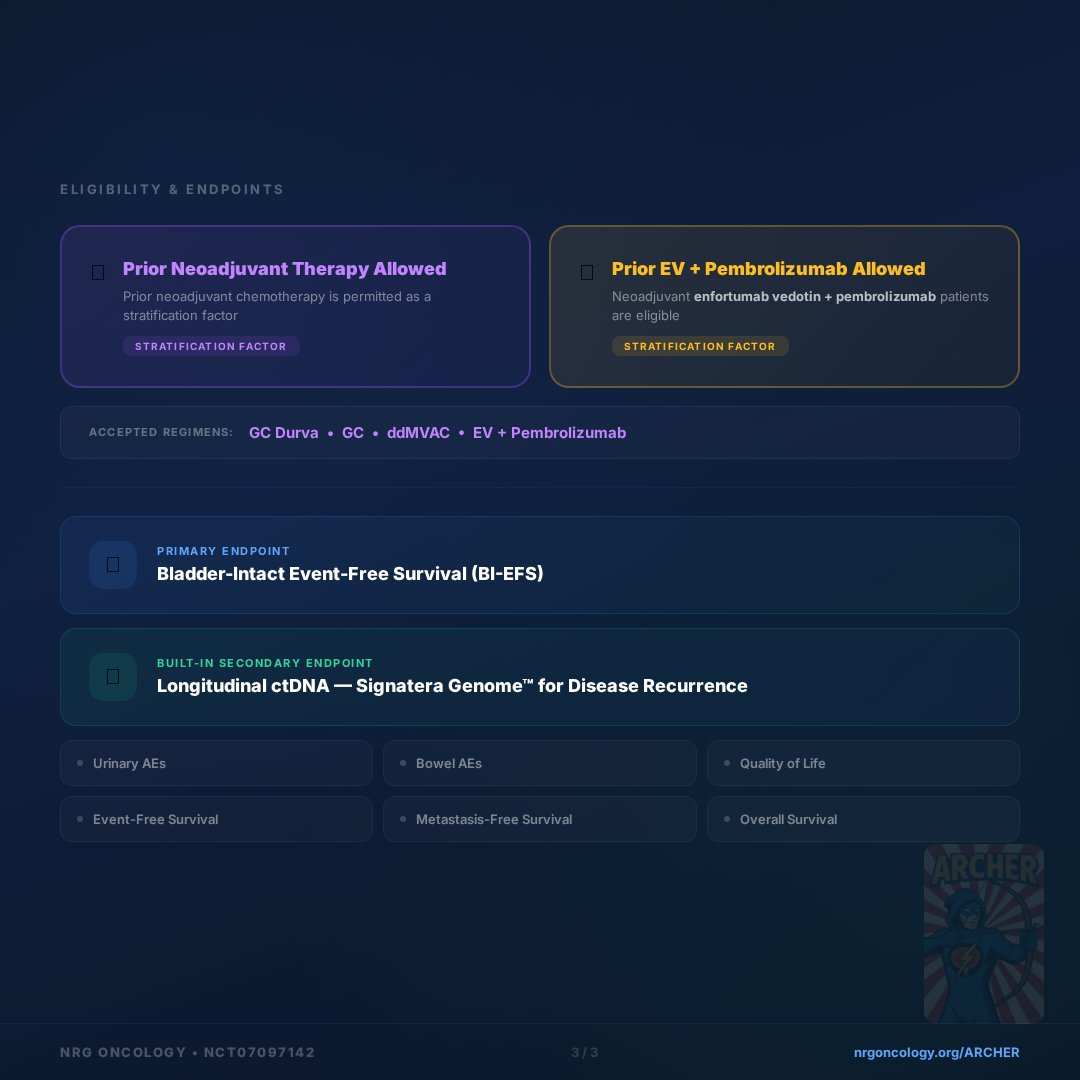
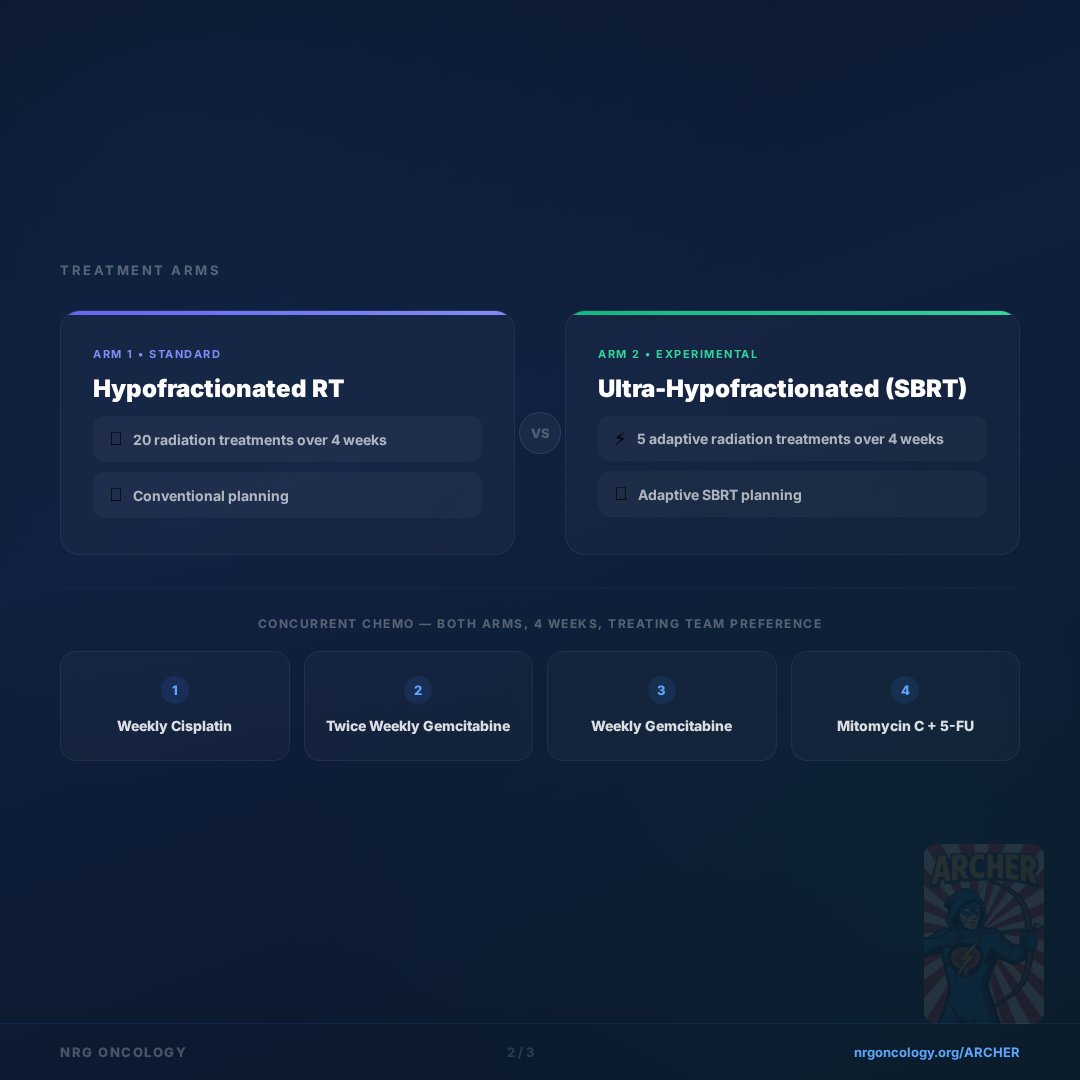
May is #BladderCancerAwarenessMonth. We're highlighting studies in our GU portfolio. NRG-GU015 The ARCHER Study is enrolling patients with cT2-cT3 MIBC that is clinically node negative. Learn more ➡️ ow.ly/RqQm50YZJ59 @UroCancer @HimanshuNagarMD

1
7
7
706
Scott E Delacroix Jr M.D. retweeted

May 18
After 10 years as @UroOnc PD at @UTMDAnderson, Happy to announce @KKBree will assume the role
As APD, she has shown an unique ability 2 connect w/fellows while maintaining the rigor needed to train today’s Uro Oncs
Proud of her leadership excited for the future #oncsurgery

8
5
125
5,106
Scott E Delacroix Jr M.D. retweeted
May 15
For #BladderCancerAwarenessMonth, we're highlighting NRG studies in our GU portfolio that are currently enrolling patients - NRG-GU014, The PARRC Trial is enrolling patients with high-grade T1 #bladdercancer. Learn more ➡️ow.ly/fJe950YZI4N @BrianBaumannMD @UroCancer
2
2
234
Scott E Delacroix Jr M.D. retweeted
Debate resulted in consensus: support clinical trials! We don’t know unless we investigate.
What an honor to discuss management of PSMA-only M1a #ProstateCancer with Jeff Karnes @CaPsurvivorship @UroCancer @DrSpratticus
#AUA26 @urogeek
May 15

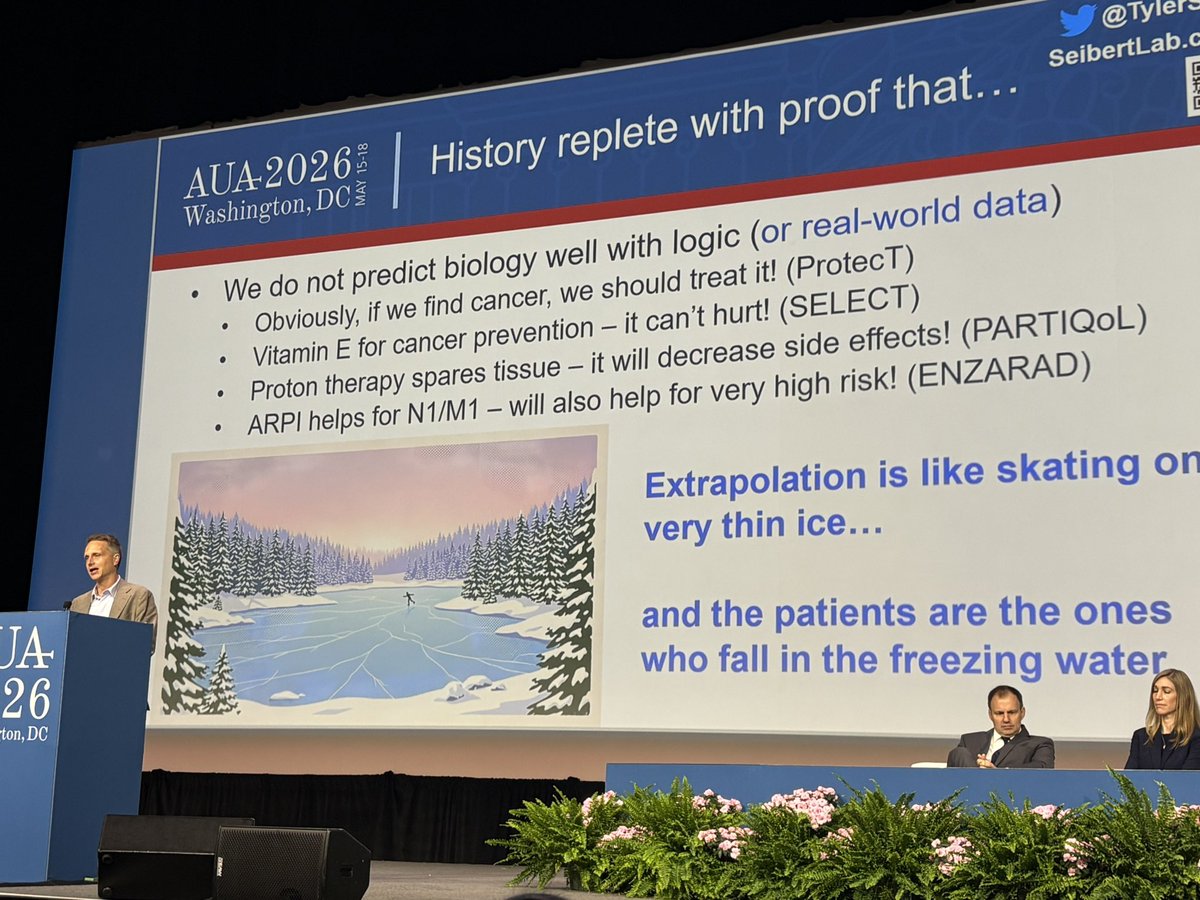
My favorite slide from exciting #AUA26 crossfire discussion so far by @TylerSbrt on M1a PCA. Beware of indirect evidence. We have been burnt before.
4
27
1,848
Scott E Delacroix Jr M.D. retweeted

May 15
My favorite slide from exciting #AUA26 crossfire discussion so far by @TylerSbrt on M1a PCA. Beware of indirect evidence. We have been burnt before.
2
14
50
9,393
3
6
596
77
Scott E Delacroix Jr M.D. retweeted

May 9
Q: Is there a reason why the chemoRT arm does not allow neoadj EVP? With 302/303 showing clear benefit of addition to local tx, the control arm of chemoRT alone feels handicapped. NRG GU15 and S2427 both allow EVP as SOC leading into CRT/IO-RT as example.
4
4
30
2,814
Scott E Delacroix Jr M.D. retweeted

May 10
That’s not true. Most people are reasonable when their concerns are acknowledged in a polite and reasonable manner.
1
3
21
1,652
Scott E Delacroix Jr M.D. retweeted

May 10
Struggle to see consenting physician not offering EVP. Trial only makes sense in places that don’t have EVP access. “We have a drug combination that is a sea change in bladder cancer but there’s a 50% chance you will not get it if you enroll on this trial.”
Just because you decline RC (as this trial allows) shouldn’t deny access to EVP.
3
16
1,060
Scott E Delacroix Jr M.D. retweeted

Dogma, Doubts, and Debunking Myths: Which Are Next? Outstanding presentation by @uroegg challenging long-held medical beliefs that persist despite little to no supporting evidence. @USC_Urology @UclaUrology

1
8
52
2,572
Scott E Delacroix Jr M.D. retweeted

"Where do all my healthcare dollars go?"
May 4

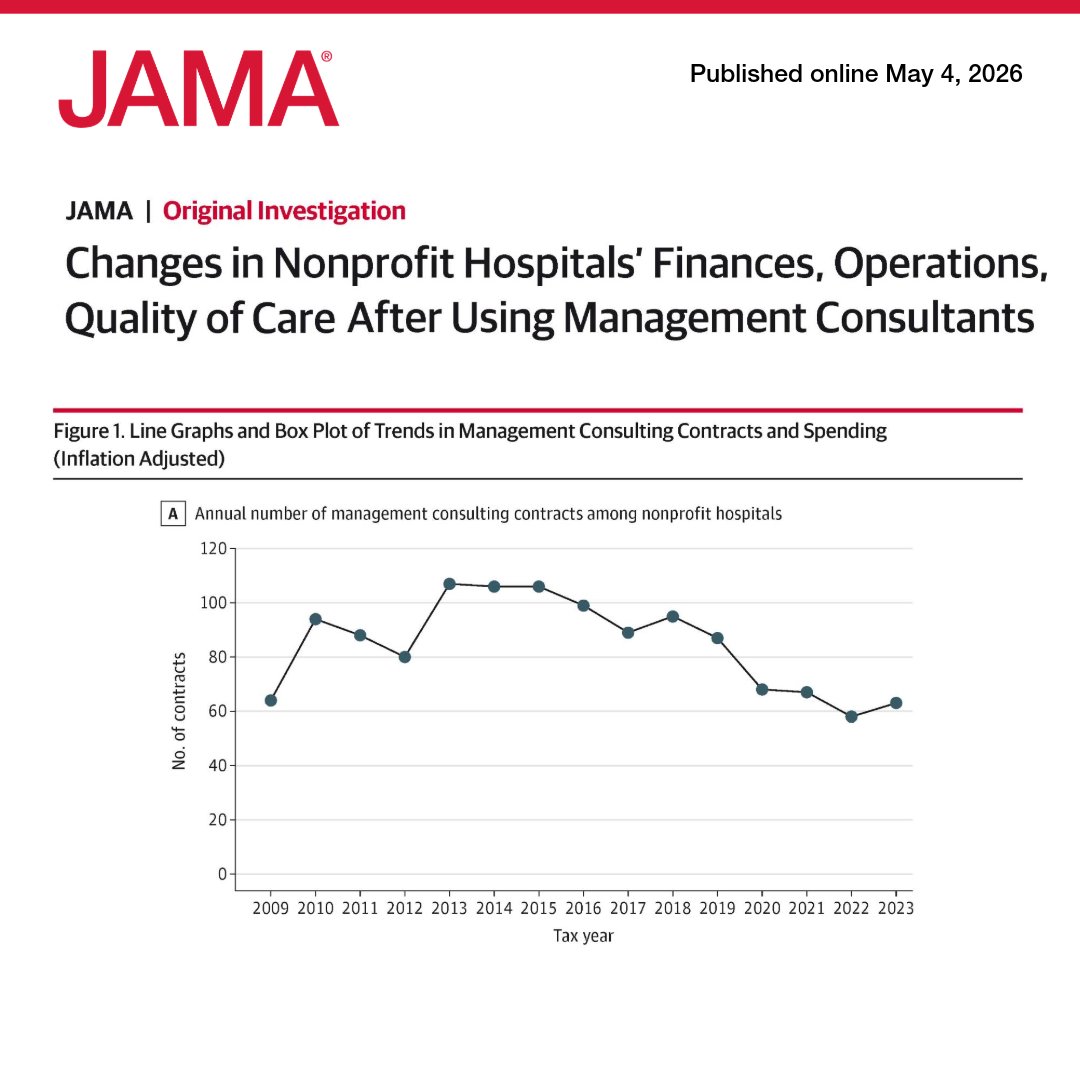
US nonprofit hospitals spent $7.8 billion on management consultants from 2009 to 2023, but contracts were not associated with meaningful changes in finance, operations, or quality of care. 🧵
ja.ma/4d46zfq
5
3
23
1,634
Scott E Delacroix Jr M.D. retweeted

May 4
US nonprofit hospitals spent $7.8 billion on management consultants from 2009 to 2023, but contracts were not associated with meaningful changes in finance, operations, or quality of care. 🧵
ja.ma/4d46zfq
82
614
1,532
623,078