
Endowed Professor, Surgeon, Former Fellowship Director @UTMDAnderson | President @IBCG_BladderCa | Assoc Editor @EurUrolOncol | Views my own
Joined March 2010
- Tweets 10,246
- Following 829
- Followers 12,594
- Likes 22,528
1,084 Photos and videos







Pinned Tweet

Deeply honored to receive The Tagore Medal from the Urological Society of India (USI)
“The Tagore Medal is a prestigious lifetime achievement award in Uro-Oncology, presented to recognize pioneering national and global contributions, groundbreaking advances, and leadership in the field.
Presented under the aegis of the USI Uro Onco Section, the award reflects a shared commitment to advancing research, education, innovation, and patient care across prostate, kidney, and bladder cancers.”
Truly humbled by this recognition.
@usioffice @UTMDAnderson #OncSurgery
32
15
128
38,816
General-purpose LLMs outperform specialized clinical AI tools on medical benchmarks
@NatureMedicine
Frontier models beat OpenEvidence and UpToDate Expert AI across every evaluation, including real physician queries rated by blinded clinicians.
Not unexpected, but surprising nonetheless!
nature.com/articles/s41591-0…
1
3
10
943
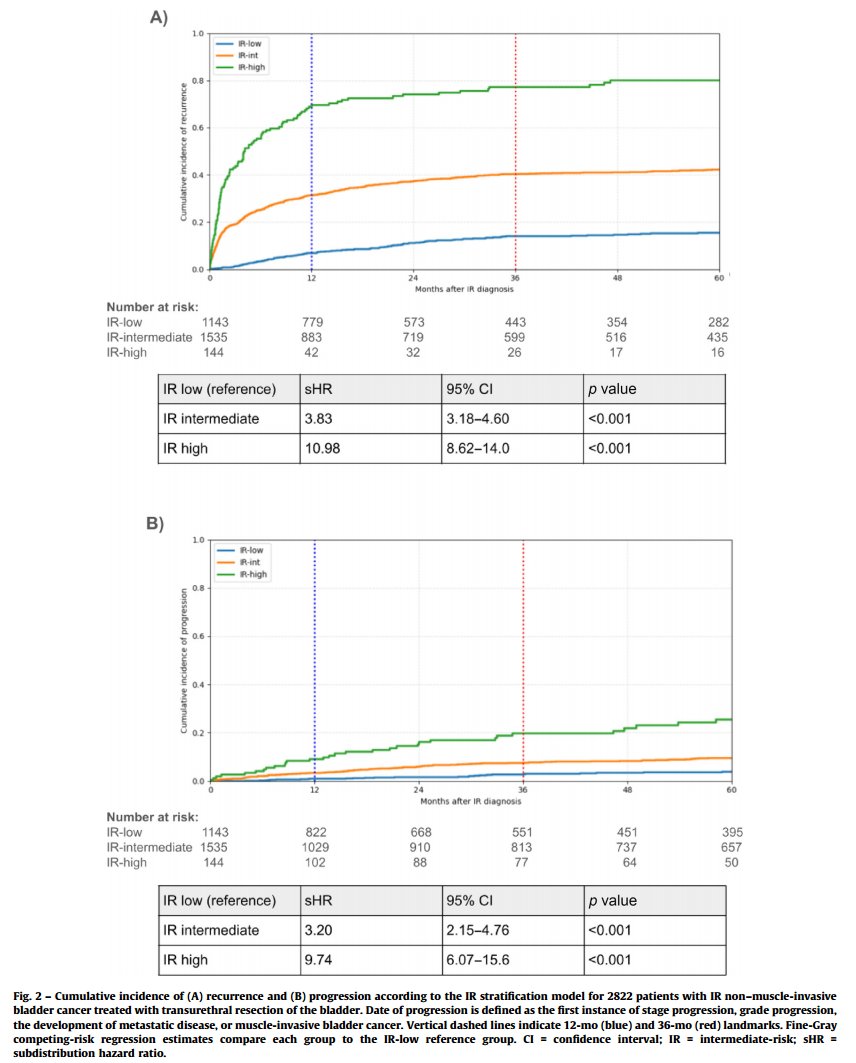
Congratulations to @LauraBukavinaMD @jaymsiva @drjkaouk and @ClevelandClinic team on largest external validation of the IBCG IR NMIBC substratification model
📊 2822 patients | 20 years | 3-year recurrence by subgroup:
🟢 IR-low: 12%
🟡 IR-intermediate: 38%
🔴 IR-high: 77%
Progression followed the same stepwise pattern. Fine-Gray competing-risk models confirmed significance (p<0.001) - separation held on 12-month landmark analysis, ruling out early-event bias.
Yet more evidence that trials enrolling IR NMIBC should stratify by IBCG subgroup at enrollment to be clinically meaningful.
Conflating patients with 12% and 77% recurrence risk in the same trial arm is a fundamental problem.
Full text:
authors.elsevier.com/sd/arti… @IBCG_BladderCA
2
12
44
6,534
This builds on the body of evidence supporting our @IBCG_BladderCA IR NMIBC Risk Scoring system eg 👇
20 Jan 2025

Clinical Validation of the Intermediate-risk Non–muscle-invasive Bladder Cancer Scoring System and Substratification Model Proposed by the International Bladder Cancer Group by @frasor86 et al
buff.ly/3Bg84Zj
#UroSoMe #MedTwitter #EUO

2
1
7
2,415
And further enhances rationale for its inclusion in the March 2026 @NCCN Guidelines

Pleased to share that the 2026 @NCCN Bladder Cancer Guidelines now incorporate the @IBCG_BladderCa risk stratification framework for intermediate-risk NMIBC.
A milestone reflecting more than a decade of collaborative work by colleagues worldwide
einpresswire.com/article/901…
@UrogerliMD @drtanws @shilpaonc @pjhensley11 @mouwlab @AndreaNecchi @LAUrology_NL @AmirHorowitz @karima_oualla @PGrivasMDPhD @paolo_gontero @pcvblack @MaxKates @SpiessPhilippe @RobertoContieri @KKBree @LauraBukavinaMD @MRoupret @joanfundi @UroToday @BladderCancerUS @WorldBladderCan
1
2
1,395
Ashish M. Kamat, MD, MBBS retweeted

Jun 11
Individual patient data analysis explores the benefit of adding immunotherapy to BCG in #BladderCancer. @UroDocAsh @UTMDAnderson joins @zklaassen_md @GACancerCenter to discuss a commentary analyzing BCG plus checkpoint inhibitor trials in #NMIBC. #WatchNow on UroToday > bit.ly/4sKNlC4 @JCO_ASCO
9
14
1,853
Ashish M. Kamat, MD, MBBS retweeted
Jun 10
Bladder Burden Survey findings on patient trust, unspoken struggles, and mental health in #BladderCancer. @UroDocAsh @UTMDAnderson joins @zklaassen_md @GACancerCenter to discuss the survey findings, covering data collected from approximately 800 patients across six countries and a matched cohort of urologists. #WatchNow > bit.ly/49JzaWM @BladderCancerUS @WorldBladderCan

5
11
732
New data in @Annals_Oncology: A target trial emulation of >229K obese, nondiabetic adults shows GLP-1RA use is associated with a 41% reduction in obesity-associated cancers compared to lifestyle modifications alone (HR 0.59). - Congratulations to Aparna Kamat, Arthur Hsu, @pedroramirezMD & entire @MethodistHosp team
annalsofoncology.org/article…
@SGO_org
3
17
48
9,755
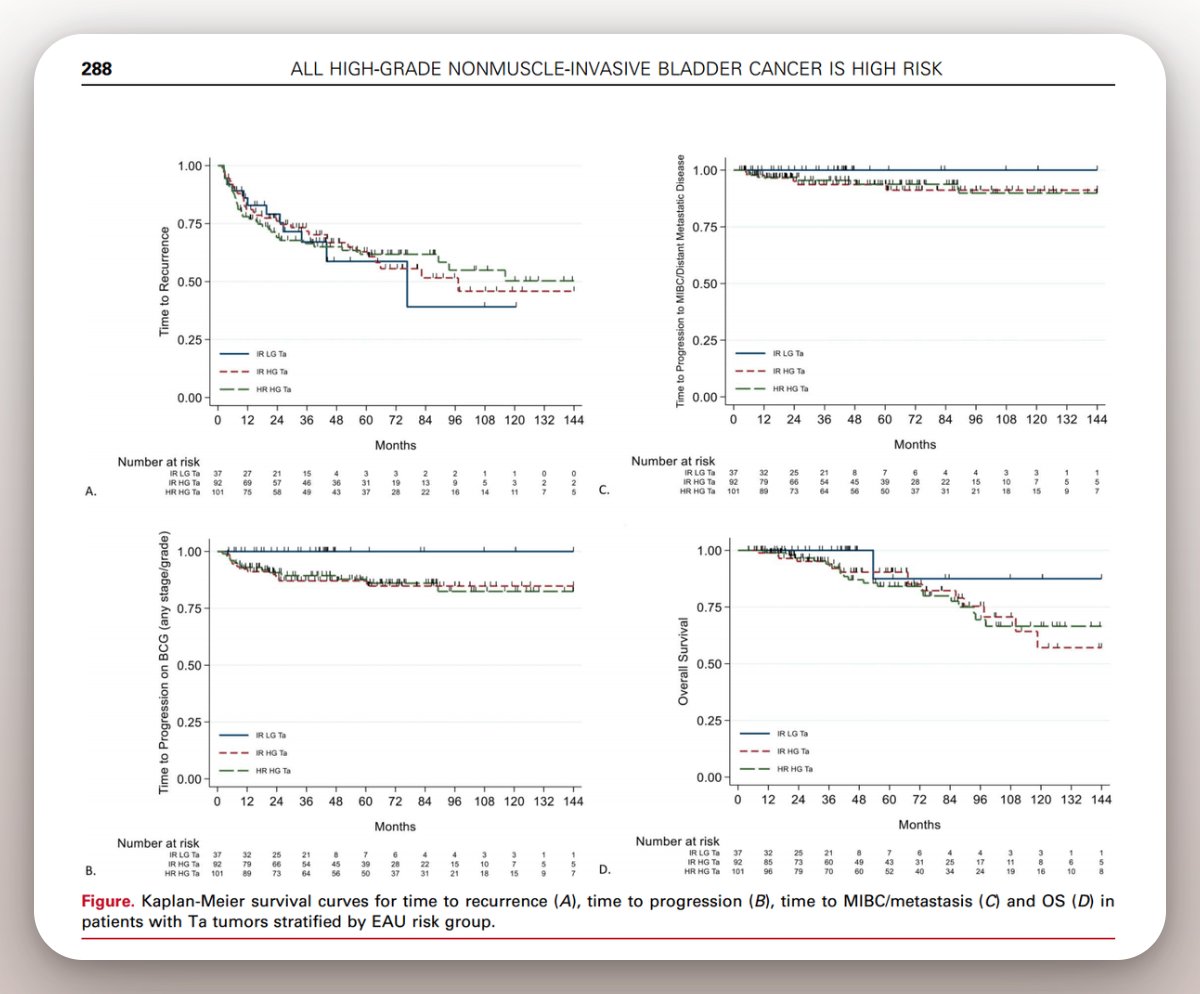
This paper by @drtanws @heerlab @emmahall71 provides supporting evidence removing TaHG NMIBC from the IR NMIBC risk category
When we properly define IR-NMIBC the way @IBCG_BladderCA recommends - LG disease only - and look at what happens to those patients across four RCTs (578 patients, contemporary treatment):
Stage progression: 2%
MIBC or metastasis: 2%
Cancer-specific mortality: <1%
New paper just out in @EurUrolOncol - outcomes of patients with intermediate-risk NMIBC when treated with contemporary protocols?
We analyzed 578 patients across 4 RCTs. IR NMIBC defined as per @IBCG_BladderCA and 2019 EAU Guidelines - only LG tumors.
Real-world relevant data. Here is what we found. 🧵
Ohttps://euoncology.europeanurology.com/article/S2588-9311(26)00127-6/fulltext
1
6
18
5,148
Now look at our paper on TaHG patients treated with adequate BCG @KKBree et al., J Urol 2022 @pjhensley11 @niyatilobo
Stage progression: 13%
MIBC or metastasis: 6%
BCG unresponsive: 13-14%
Stage progression is 6x higher in TaHG than LG
MIBC/metastasis risk is 3x higher than LG
Make your own conclusions
@MaxKates @LauraBukavinaMD @djmcconkey @joanfundi @drtanws @paolo_gontero @LAUrology_NL @ParamMariappan
Our @JUrology paper looked at 251 patients with TaHG tumors. All treated with adequate BCG. We stratified them by risk groups - "intermediate-risk" vs "high-risk" - based on clinical factors like tumor size, age, multifocality.
All TaHG tumors behaved the same: BCG unresponsiveness: 14% vs 13%
Stage progression: 13% in both groups.
MIBC or metastasis: 6.5% vs 5.9%.
Multicenter cohorts and AI-based pathology studies have since shown the same thing: the clinical factors used to downgrade TaHG to intermediate risk do not meaningfully discriminate outcomes.
Once a Ta tumor is high grade, the biology drives the behavior. #BladderCancer #ASCO26 #OncSurgery @KKBree
4
5
1,770
New paper just out in @EurUrolOncol - outcomes of patients with intermediate-risk NMIBC when treated with contemporary protocols?
We analyzed 578 patients across 4 RCTs. IR NMIBC defined as per @IBCG_BladderCA and 2019 EAU Guidelines - only LG tumors.
Real-world relevant data. Here is what we found. 🧵
Ohttps://euoncology.europeanurology.com/article/S2588-9311(26)00127-6/fulltext
1
15
55
9,361
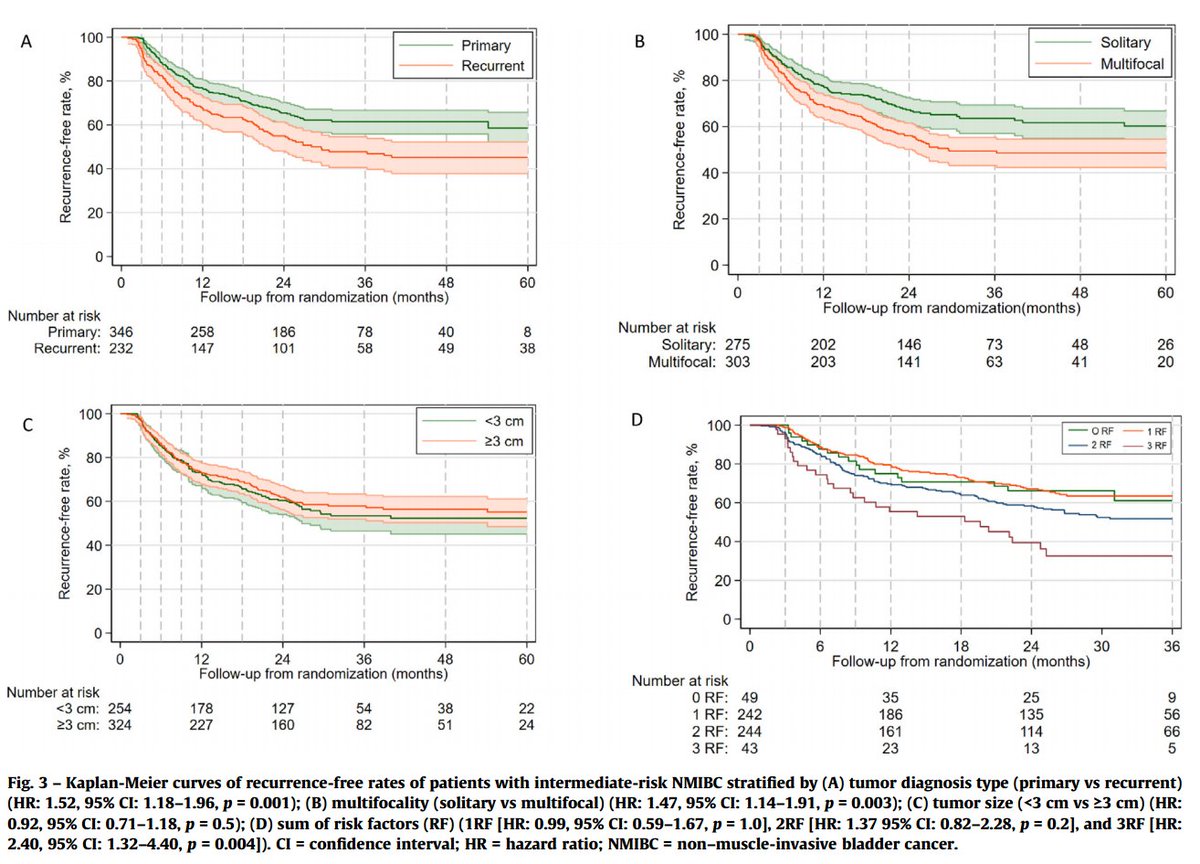
On multivariable analysis, three factors independently predicted recurrence:
-- Prior recurrence: HR 1.75 (p=0.008)
-- Multifocality: HR 1.49 (p=0.004)
-- Grade G2 vs G1: HR 1.57 (p=0.018)
One factor that did NOT predict recurrence:
-- Tumor size: HR 1.08 (p=0.6)
1
2
13
1,176
The reassuring part:
Grade progression (LG to HG): 5%.
Stage progression (Ta to T1 or higher): 2%.
MIBC or distant metastasis: 2%.
Cancer-specific mortality: < 1%.
This suggests that IR-NMIBC - properly defined as low-grade disease - has a high recurrence burden but a benign long-term trajectory.
De-intensification of both treatment AND surveillance is appropriate for selected patients.
2
9
430
Ashish M. Kamat, MD, MBBS retweeted
Jun 4
CORE-008 CX early efficacy and tolerability data. Aaron Berger, MD joins @UroDocAsh to discuss CORE-008 CX arm data, cretostimogene combined with intravesical gemcitabine in approximately 55 BCG-exposed and BCG-unresponsive patients with CIS and high-grade papillary disease. #WatchNow > bit.ly/4o8WWkF

3
4
650
Ashish M. Kamat, MD, MBBS retweeted
Jun 3
BOND-003 Cohort C: Durability of responses examined with cretostimogene in BCG-unresponsive #BladderCancer. Shreyas Joshi, MD, MPH @winship_cancer joins @UroDocAsh @UTMDAnderson reviewing 24-month durability data from BOND-003 Cohort C, a study of cretostimogene grenadenorepvec in BCG-unresponsive CIS patients. #WatchNow on UroToday > bit.ly/4dnjevQ @cgoncology
1
5
8
1,298
Ashish M. Kamat, MD, MBBS retweeted
Jun 3
DRIFT: A floating device for intravesical gemcitabine-docetaxel delivery. James Byrne, MD, PhD @uiowa joins @UroDocAsh @UTMDAnderson to discuss the DRIFT - Drug-Releasing Intravesical Floating Technology for sequential gemcitabine-docetaxel delivery. #WatchNow > bit.ly/3PDEYdd
6
10
1,535
Ashish M. Kamat, MD, MBBS retweeted
Jun 3
Systematic review of cure definitions in early #BladderCancer. @DrFelixGuerrero @Urologia12, and @UroDocAsh @UTMDAnderson discuss a systematic review of 110 real-world studies defining cure in early bladder cancer. Dr. Guerrero-Ramos emphasizes that counseling should be tailored to what matters most to each patient. #WatchNow > bit.ly/4viQUBo
10
21
1,867