
National advocate for patients, clinicians, research & scientists… all who are involved in living with, treating, or researching chronic/persistent pain.
Joined March 2012
- Tweets 47,932
- Following 4,549
- Followers 6,893
- Likes 133,085
1,157 Photos and videos



Pinned Tweet

2 Sep 2021
1. My #RealPainStory: in 2006, I jumped down a mountainside to stop a child from going over a cliff. I herniated a few discs. 6 months later, a neurosurgeon confused me with a different patient, & cut out the back of my lumbar spine. That plunged me into my first 15 years of pain
55
84
255
Andrea Anderson retweeted

It’s deja vu all over again!
pubmed.ncbi.nlm.nih.gov/4173…
7 May 2025

CAUGHT LYING AGAIN: Author Jane C. Ballantyne, professor, once again asserts she has no conflicts of interest when publishing an editorial in a top-5 international medical journal.
In her BMJ editorial, “Spinal interventions for chronic back pain: Do negative findings demand action?”
BMJ 2025;388:r179
doi.org/10.1136/bmj.r179
Published: 19 February 2025
Let’s examine her claim:
***Financial Conflicts of Interest for Jane Ballantyne***
1. Paid Consultant for Law Firms
Ballantyne has worked as a highly-paid consultant for Motley Rice, a law firm involved in opioid litigation, with potential to earn millions in consulting expert fees.
She eventually disclosed this, years after she should have, in a revised statement to Annals of Internal Medicine in 2019, long after she had been working with them as early as 2012.
Ballantyne previously served as a paid consultant for Cohen Milstein Sellers & Toll, another law firm engaged in opioid litigation, only disclosed to the CDC during the 2016 opioid guideline development.
2. Expert Witness in Opioid Litigation:
She acted as a paid expert witness in opioid litigation lawsuits, a lucrative sideline for PROP members, with some earning up to $850/hour. Specific cases or total compensation not detailed in disclosures.
3. Non-Disclosure Issues plaguing Jane Ballantyne:
Ballantyne has failed to report conflicts of interest in 84% of qualifying publications, despite being a section editor for a medical journal highly aware of ethical disclosure standards, standards she enforces for authors who seek to publish in the journal for which she is an editor.
Co-authored articles (e.g., with Mark Sullivan) where litigation-related conflicts were not disclosed, requiring corrections.
She did not disclose Motley Rice consultancy due to a confidentiality agreement; later revised disclosure after scrutiny. Here is her falsified form that she was later forced to correct:
static1.squarespace.com/stat…
Explaining away her failure to disclose, the journal said, “in a recent Ideas and Opinions commentary, Dr. Ballantyne did not disclose that she has received personal fees for the multidistrict opioid litigation because her consultancy in the litigation was under a confidentiality agreement. Dr. Ballantyne has now updated her disclosure because her role in the multidistrict litigation has since become public knowledge,” acpjournals.org/doi/10.7326/…
**The ethical standard for disclosing conflicts of interest is not that “your role was made public.”
In the next post, I will detail what are the ethical requirements for disclosing conflict of interest is the ethical standard for disclosing complex of interest in academics::
4. Recent X posts (2025) suggest Ballantyne may still be on retainer with Cohen Milstein, though this is unconfirmed by primary sources.
5. Ballantyne’s conflicts stem from her consultancy and expert witness roles in opioid litigation, compounded by inconsistent disclosure practices and her leadership in PROP, an advocacy group with aligned interests.
Why do journals allow the PROP cartel to exert outside influence in legal, administrative, publishing, committee memberships, and media outlets, when they have been caught in repeated lies, failures to disclose relevant COIS (which continues to this day) as they manipulate and deceive journal readers, stakeholders, affected persons, and the journals themselves?
Surely the @bmj_latest is better than this.
@bmj_latest please investigate this issue.
2
9
20
750
Andrea Anderson retweeted

Jun 10
⭐️VERY INFORMATIVE POST!⭐️
You may not be aware of companies like OwnYourLabs.com that will order your lab results whenever you want them, without a doctor's visit. Here is a sample of what they charge. This list is not complete. You go to the site, request the labs you want, and then have them drawn a Quest, Labcorp, etc. Your results will be available online. Then, put your results into CHATGPT for a detailed summary. This is great if your insurance deductible isn't met or you don't have insurance.
• CMP — $10.00
• Hemoglobin A1c — $8.80
• Lipid Panel — $10.00
• CBC w/Differential & Platelets — $8.40
• Insulin — $14.40
• hs-CRP (Cardiac) — $26.40
• TSH — $13.20
• ApoB — $17.20
• Vitamin D (25-OH) — $44.60
• Ferritin — $15.00
• Free T4 — $17.00
• NMR LipoProfile IR Markers — $78.60
• Lipoprotein(a) [Lp(a)] — $35.20
• Free T3 — $43.20
• Iron & TIBC — $17.20
• Vitamin B12 & Folate — $34.40
• Cortisol — $19.80
I did some research on places similar to OwnYourLabs for anyone that would like to save $$$ on lab tests that do not require a doctor's order. Not all are available in every state. Here's the list:
OwnYourLabs — ownyourlabs.com
Ulta Lab Tests — ultalabtests.com
Walk-In Lab — walkinlab.com
DirectLabs — directlabs.com
Request A Test — requestatest.com
Private MD Labs — privatemdlabs.com
Life Extension Lab Testing — lifeextension.com/lab-testin…
True Health Labs — truehealthlabs.com
HealthLabs — healthlabs.com
QuestDirect — questhealth.com
Labcorp OnDemand — ondemand.labcorp.com
140
688
1,927
73,342
Jun 10
Phenomenal news from @AmerMedicalAssn regarding pharmacy denials of analgesic medications, the rates of denials, and the reasons for them.
Thank you, the champion of the cause of caring for and protecting those who suffer so greatly: @ChadDKollas

BREAKING: The @AmerMedicalAssn has adopted the following policies at its 2026 #AMAmtg:
"The AMA [will] convene a meeting with the National Association of Boards of Pharmacy and other national pharmacy organizations to identify ways to improve communications between physicians and pharmacists about physicians’ and pharmacists’ corresponding responsibility and related areas" about physicians' plenary prescriptive authority (including controlled medications), providing a report in June 2027....
The "AMA [will] work with pharmacies subject to the national opioid litigation settlements to provide data on refusals to fill and dispense medications, including the reasons for such refusals."
2
1
1
101
Andrea Anderson retweeted
Actually, what the authors (several of whom have financial connections to lawsuits against opioid manufacturers) conclude is exactly this:
"Opioid analgesics are efficacious in reducing pain in some acute conditions."
All pain care must be individualized. For some acutely painful conditions (musculoskeletal pain, for example), anti-inflammatory medications may be better choices (depending on patients' comorbidities, such as renal impairment).
Several of these authors were involved in the deeply flawed @OPALstudy. There are underlying financial conflicts at issue. #DontDrinkTheKoolaid
Jun 9

“World's largest opioid review finds they often don't work”
6/9/26
sciencedaily.com/releases/20…
“Efficacy and Harms of Opioid Analgesics for Acute Pain: Overview of Systematic Reviews and Meta-analyses.”
Drugs, 2026; 86 (4)
link.springer.com/article/10…
@ibdgirl76
@ChadDKollas
4
21
54
1,608
Jun 9
These people have #Opal connections? well then this is utterly predictable. Of course opioids are very important for acute conditions like kidney stones.
Actually, what the authors (several of whom have financial connections to lawsuits against opioid manufacturers) conclude is exactly this:
"Opioid analgesics are efficacious in reducing pain in some acute conditions."
All pain care must be individualized. For some acutely painful conditions (musculoskeletal pain, for example), anti-inflammatory medications may be better choices (depending on patients' comorbidities, such as renal impairment).
Several of these authors were involved in the deeply flawed @OPALstudy. There are underlying financial conflicts at issue. #DontDrinkTheKoolaid
1
3
216
Jun 9
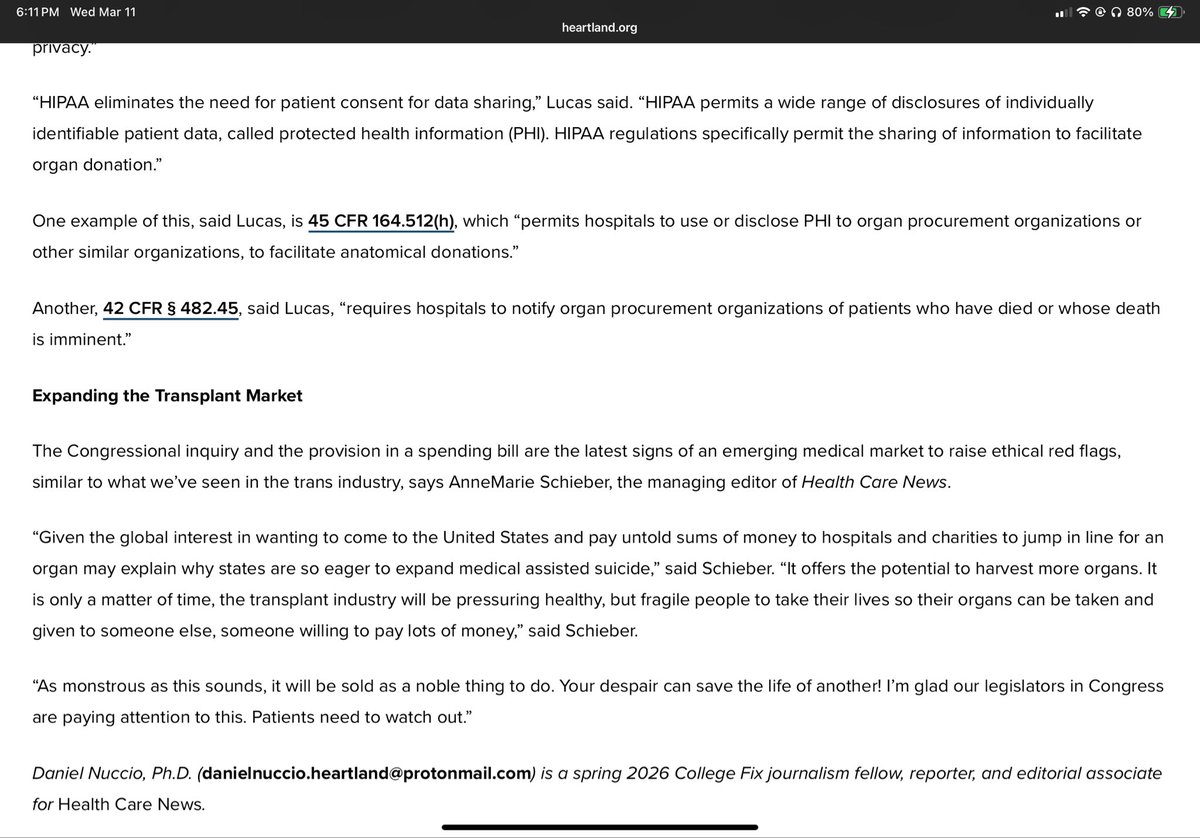
Fantastic news. This is how it should be everywhere.

Kentucky just passed a law allowing whistleblowers to pause organ harvesting when there are any signs of life: lifesitenews.com/analysis/ne…
54
Andrea Anderson retweeted
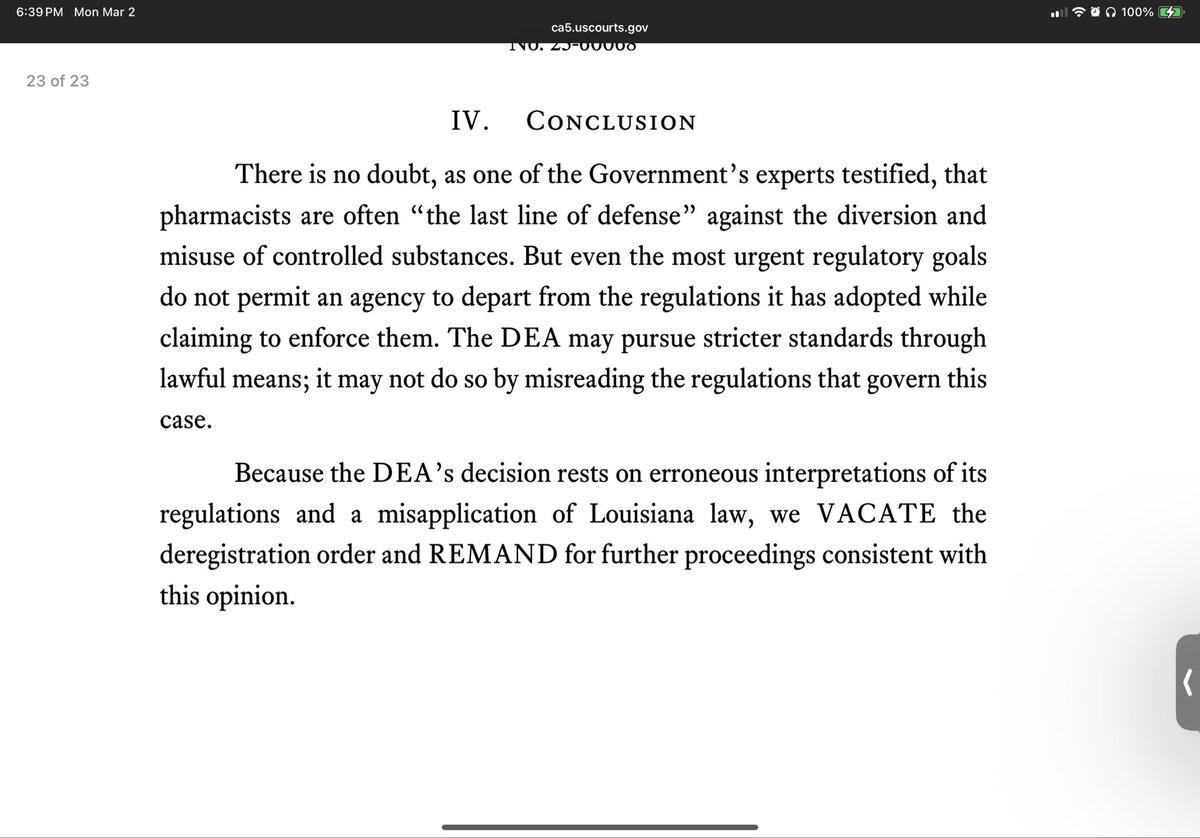
Dear @DEAHQ,
Please stop conflating prescription fentanyl and illicit fentanyl (fentalogues). You risk stigmatizing patients with severe illness who require prescription fentanyl to treat severe pain. #WordsMatter
dea.gov/press-releases/2026/…
10
40
128
2,089
Andrea Anderson retweeted

Jun 9
Thank you for your insights!! Here is the full interview, starting about 15 minutes in:
afr.net/podcasts/jenna-ellis…
1
3
13
2,713
Andrea Anderson retweeted
It’s that time of year again. Honored to represent @AAHPM at the @AmerMedicalAssn 2026 Annual Meeting!! #AMAmtg #hpm #hapc
2
9
32
791
Andrea Anderson retweeted
Jun 5
.@elonmusk have you considered demonetizing the killer dad who is still trying to benefit from the murder of his child for possibly having Down syndrome?
He shouldn’t profit off murdering his child.
76
216
2,526
45,931
Jun 5
H/T to @ibdgirl76 girl for sharing this article about “Medical Exceptionalism.”
It is excellent - and the link is at the end of this post.
An excerpt: “"Prudence is not a virtue when it becomes a pretext forabandonment and unnecessary suffering."
More from the article:
Jun 4
One of the most striking features of this new framework is that pain is often described as a disorder of the brain when institutions wish to emphasize neuroplasticity, central sensitization, and the role of cognition and behavior in modulating suffering. In those moments, pain is supposedly treated as fully real, fully biological, and deeply embedded in the nervous system. However, when patients seek pharmacologic relief, the philosophy becomes entirely different, and the condition is suddenly approached as uniquely dangerous to treat through medication, as though the mere fact of pain’s subjectivity has rendered it less scientifically legitimate than other disorders of the same organ system. This is not a coherent scientific standard. It is a shaky epistemology and, perhaps even worse, a morally selective one. It therefore raises a profound question: why is pain treated as biologically real enough to psychologize and even moralize, but not biologically legitimate enough to medicate?
1
2
125
Jun 4
One of the most striking features of this new framework is that pain is often described as a disorder of the brain when institutions wish to emphasize neuroplasticity, central sensitization, and the role of cognition and behavior in modulating suffering. In those moments, pain is supposedly treated as fully real, fully biological, and deeply embedded in the nervous system. However, when patients seek pharmacologic relief, the philosophy becomes entirely different, and the condition is suddenly approached as uniquely dangerous to treat through medication, as though the mere fact of pain’s subjectivity has rendered it less scientifically legitimate than other disorders of the same organ system. This is not a coherent scientific standard. It is a shaky epistemology and, perhaps even worse, a morally selective one. It therefore raises a profound question: why is pain treated as biologically real enough to psychologize and even moralize, but not biologically legitimate enough to medicate?
5
21
61
2,067
Jun 4
2
6
198
Andrea Anderson retweeted

Good that some Canadian media starts questioning myth of #MAID being inherently 'beautiful' and more dignifying than natural death. Good and horrible deaths happen, including with MAID... W MAID, unknowns remain. comments @rljcoelho nationalpost.com/news/maid-c… via @nationalpost
2
12
25
996
Andrea Anderson retweeted

Public trust in organ donation rests on the dead donor rule. This ethical principle states that donors must not be killed by the removal of their organs.
The dead donor rule is being violated every day.
Viable organs can only come from people who are still biologically alive. Living people have been redefined as being LEGALLY dead using the “brain death” rubric to allow organ donation.
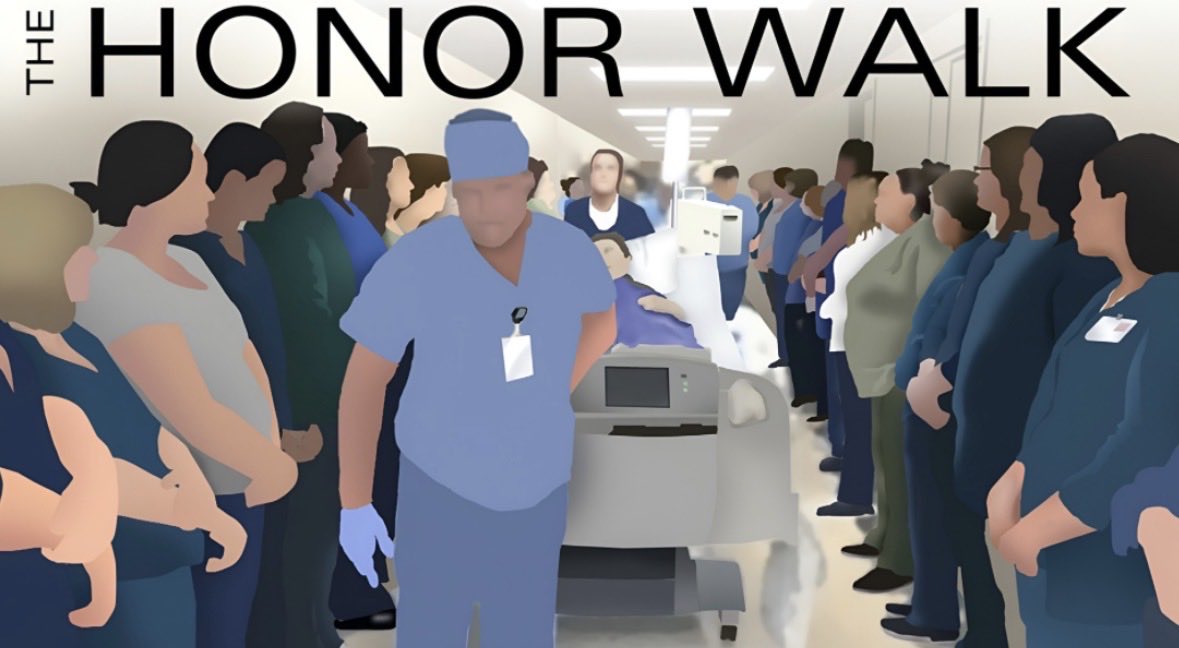
And we all know this: think about an honor walk, in which a warm, heartbeating person receiving oxygen via ambubag is walked to the operating room to become an organ donor.
Would we as easily escort this same person into a cremation chamber? Would we lower them with their beeping monitor (showing their vital signs) into a grave?
Stop accepting the doublethink. “Brain dead” people are neurologically injured, but they are not dead. Removing their organs is a concealed form of euthanasia.
14
120
261
15,686
May 30
This would be insurance companies astroturfing as crusaders to stop personal injury verdicts.
While I agree nuclear verdicts can be out of control, and the LOP system is outrageous, don’t be fooled by this nonsense.

Many accident victims say they felt pressured, misled, or financially trapped after hiring a personal injury lawyer.
PACT launched YourInjuryStory.com to share victim stories — and expose how the personal injury system really works.
Share your story:
1
2
59
May 26
Re: NIH submission:
I could not get mine to submit, either on my iPad or on my laptop. The submission button is just not working.
So I sent it to the email on their page and told them that the SUBMIT button is not working, but that I wanted this to be counted towards the official total.
mailto:nihstrategicplan@od.nih.gov
My comment:
Recommendations for NIH Funding Priorities in Chronic Pain Research
Submitted in Response to NIH Request for Input on Pain Research Funding Allocation
1. Comprehensive Research on the Causes, Sequelae, and Long-Term Outcomes of Chronic Pain Across All Sources of Injury and Disease
Invest in large-scale, longitudinal studies that map the biological, psychological, and social mechanisms underlying chronic pain from all etiologies.
2. Evaluation of Current Trending Pharmacological Treatments, Including Gabapentinoids and Antidepressants
Conduct rigorous comparative effectiveness and safety studies on widely prescribed non-opioid agents. For gabapentinoids, research should specifically examine the documented association between increased prescribing for chronic pain (particularly low back pain) and elevated risks of dementia and mild cognitive impairment, including dose-response relationships and age-stratified effects in middle-aged adults.
E.g., SNRIs and TCAs) for pain management—now endorsed in clinical guidelines—focusing on real-world efficacy, long-term outcomes, and challenges associated with deprescribing, including withdrawal symptoms, relapse of pain or mood disorders, and barriers to safe discontinuation.
3. Assessment of the Actual Benefits of Long-Term Opioid Therapy
Despite decades of clinical use, high-quality evidence on the sustained benefits of opioids for chronic non-cancer pain remains limited. NIH-funded randomized controlled trials and long-term observational studies (beyond 1 year) are urgently needed to evaluate pain relief, functional improvement, quality of life, and patient-reported outcomes.
4. Outcomes Following Opioid Deprescribing Driven by Policy and Regulatory Changes
Research should systematically track the health outcomes of these patients, including pain control, mental health, overdose risk, suicide, illicit substance use, and overall mortality.
5. Longitudinal Follow-Up of Patients Subjected to Opioid Deprescribing Over the Past Decade
Dedicated cohort studies should prospectively or retrospectively follow patients tapered or discontinued from long-term opioids since approximately 2016.
6. Investigation into Harms Associated with Implanted Neuromodulation Devices, Particularly Spinal Cord Stimulators
Despite widespread adoption, spinal cord stimulators have generated over 100,000 adverse event reports to the FDA since 2016 (including tens of thousands of injuries and hundreds of deaths), with complications such as lead migration, infection, device failure, shocks/burns, nerve damage, and need for revision or removal occurring in up to 20–40% of cases in real-world data.
7. Development of Evidence-Based Protocols to Support Safe Opioid Prescribing for Patients Who Clearly Benefit
Create and validate multidisciplinary clinical protocols and decision-support tools to assist physicians in identifying, monitoring, and managing patients for whom long-term opioid therapy provides clear, sustained benefit.
1
4
6
208
Andrea Anderson retweeted
May 25
FYI: The National Institutes of Health (NIH) currently has a Request for Information up in which they are receiving public comments (until May 26th) to help shape the research priorities and strategy for NIH for 2027-2031: Request For Information
4
4
6
276