
Husband | Father | GI Radiation Oncologist at @BIDMChealth | @Harvardmed | Gastrointestinal Oncology Program | #MedEd | #RadOnc | Tweets my own
Joined February 2020
- Tweets 177
- Following 96
- Followers 186
- Likes 340
Photos and videos
Pinned Tweet

26 Jan 2022
Rad onc radiology like peas and carrots 🟢 🥕
25 Jan 2022

special guest at our abdominal imaging & intervention fellowship morning conference today...@abrams_md!!!
#radiology #radiationoncology go together like peanut butter jelly! one of my favorite parts of my job is working with our rad onc colleagues.
5
Matthew Abrams, MD retweeted
You don’t sound incredibly humbled
2
7
236
20,581
Matthew Abrams, MD retweeted

May 11
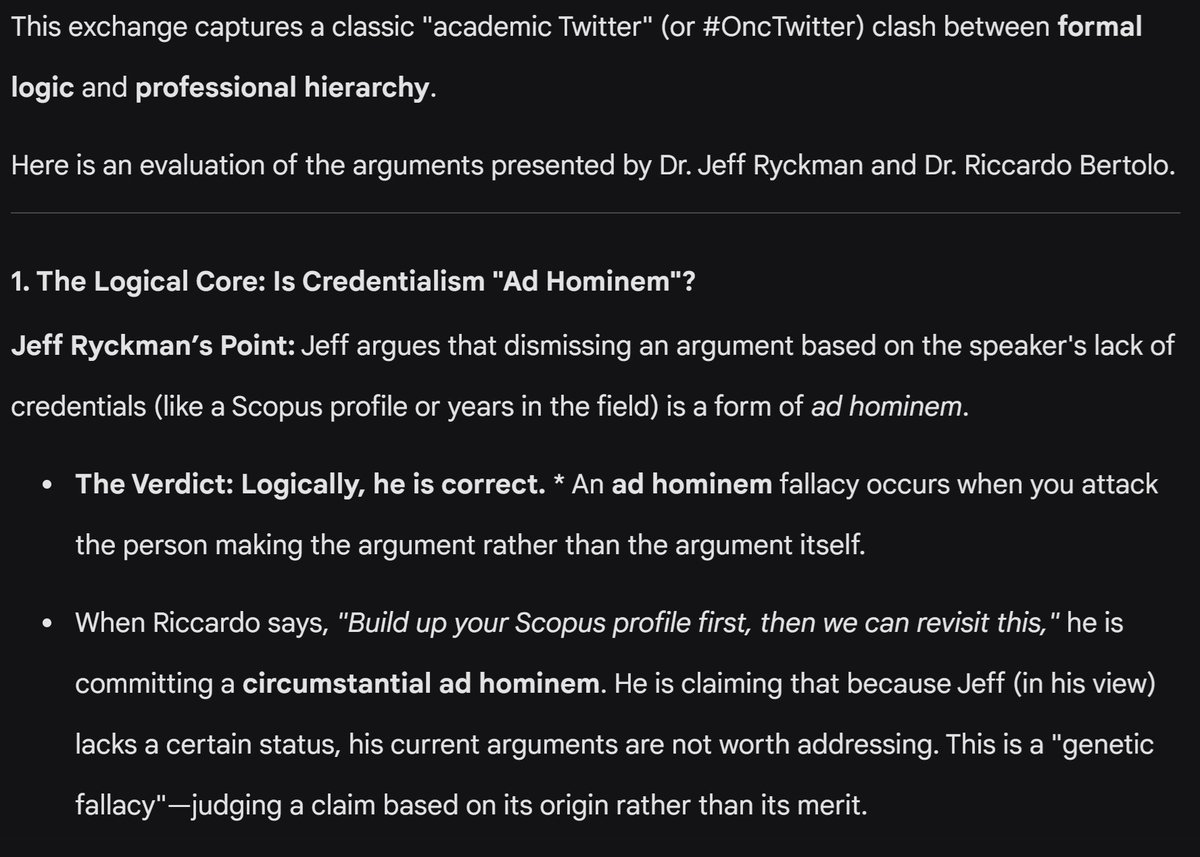
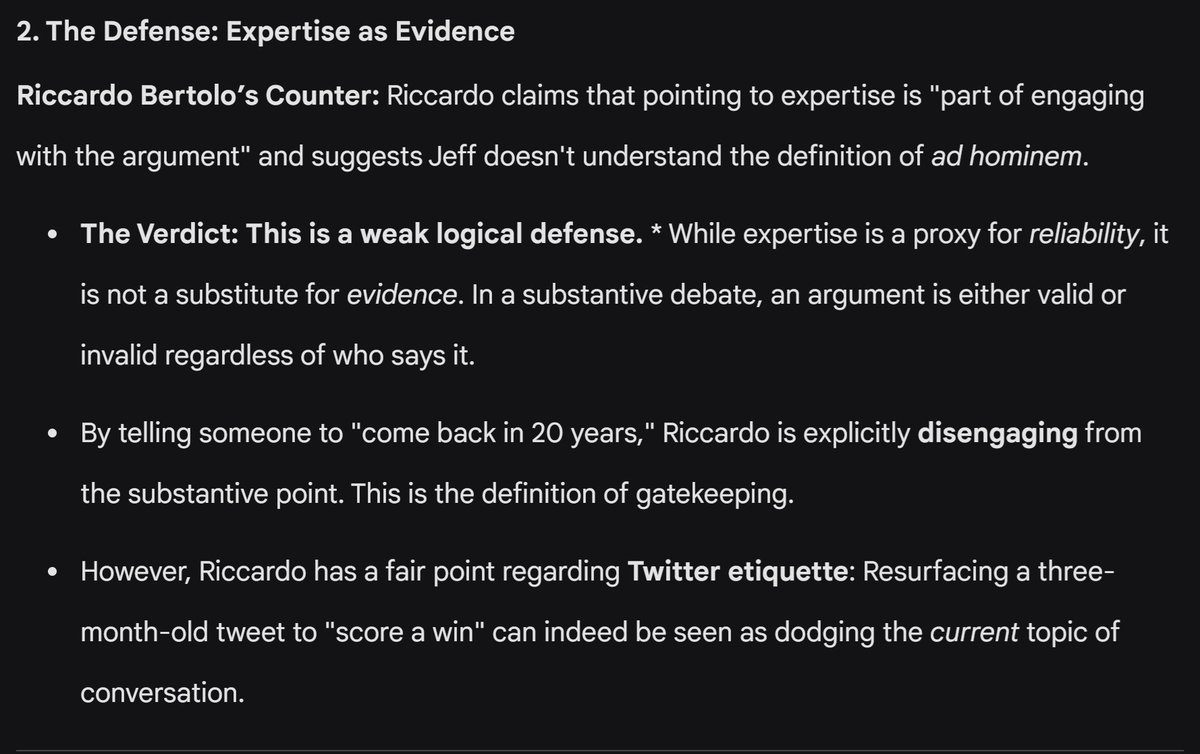
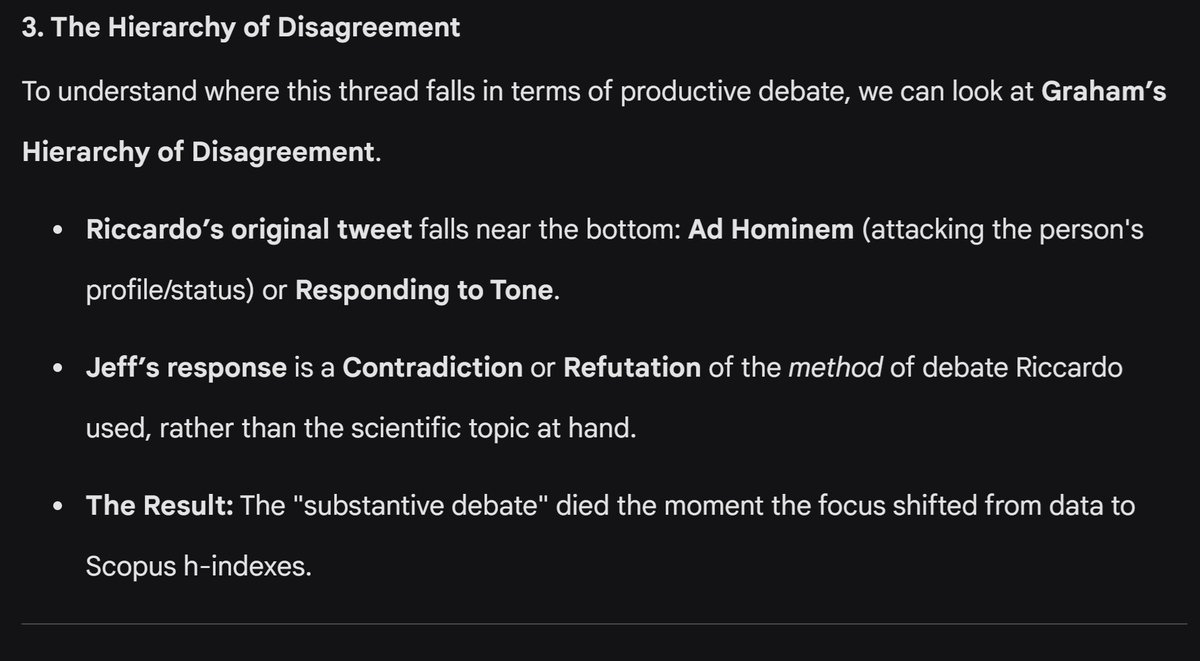
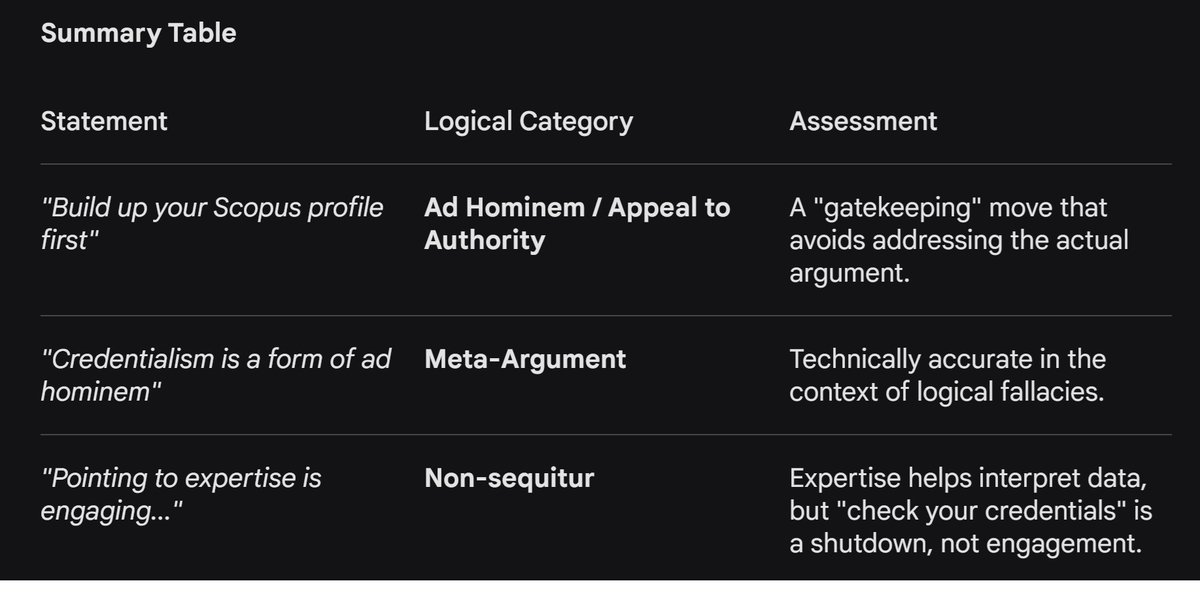
Credentialism / focus on someone's SCOPUS profile is textbook definition of ad hominem. Only here for the meta-debate, carry on with the science debate 😀
2
4
493
Matthew Abrams, MD retweeted

May 11
Claude's conclusion on the subject /end
2
6
32
2,644
Matthew Abrams, MD retweeted

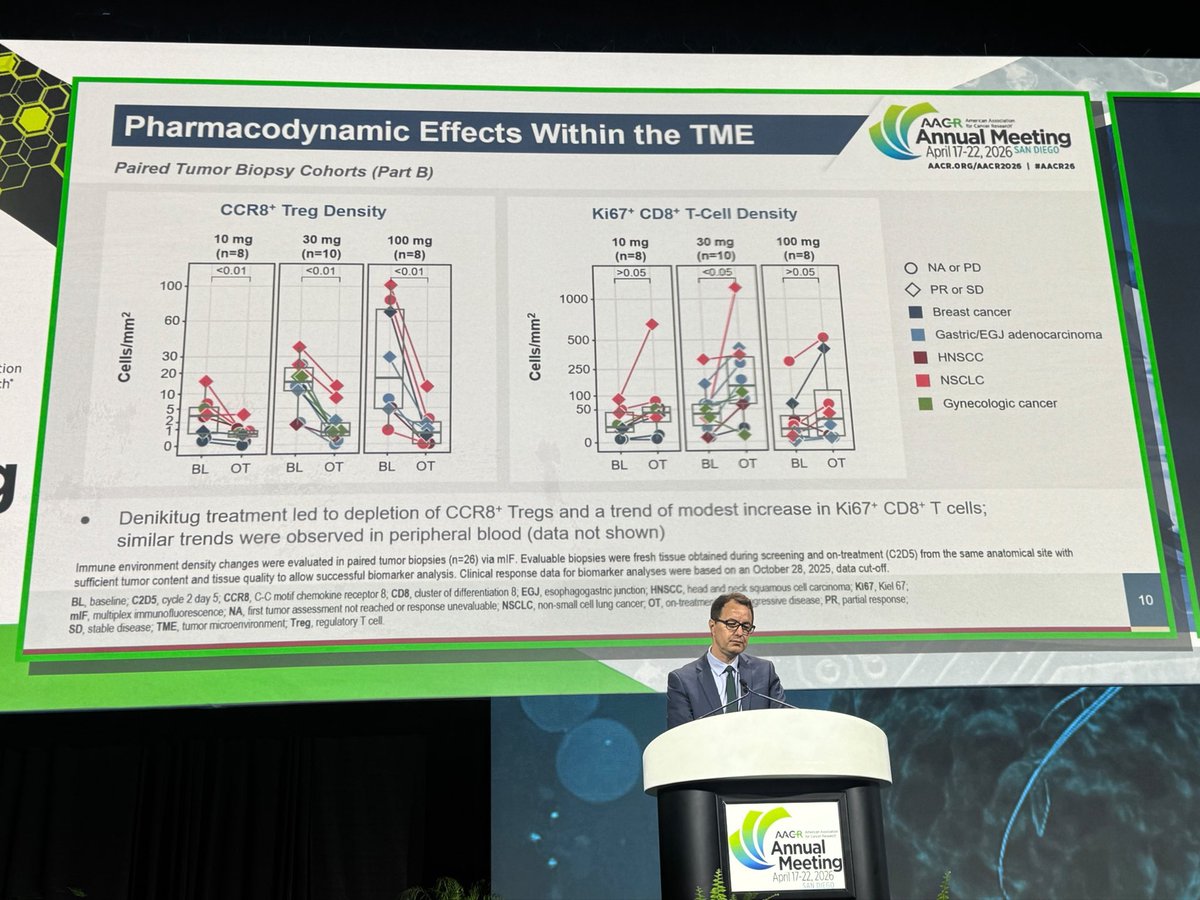
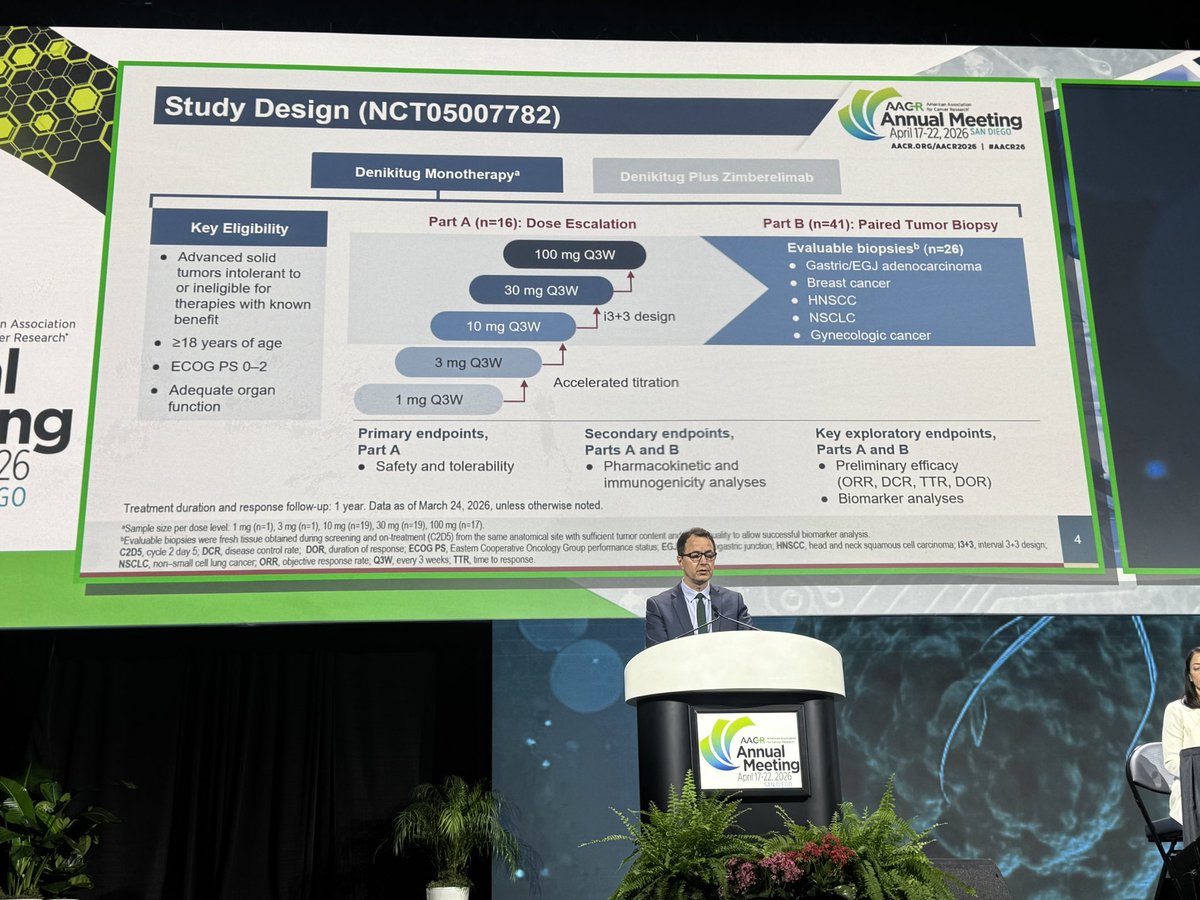
Presented Phase 1 denikitug at #AACR26. Anti-CCR8 mAb is pharmacologically active at ≥10 mg: CCR8 intratumoral Treg depletion and Teff activation on paired biopsies. Antitumor responses in heavily pretreated pts, including anti-PD-(L)1 refractory. Manageable safety. Supports mono and combo development. @BIDMC_CancerCtr @DanaFarber

3
3
17
1,531
Matthew Abrams, MD retweeted

Apr 25
"Began ~2.5 months ago"
"Recently completed"
79.2Gy in 44 fractions: BASED.
His RadOnc clearly understands how to choose wisely.
3
4
20
6,509
Matthew Abrams, MD retweeted

1 Jun 2025
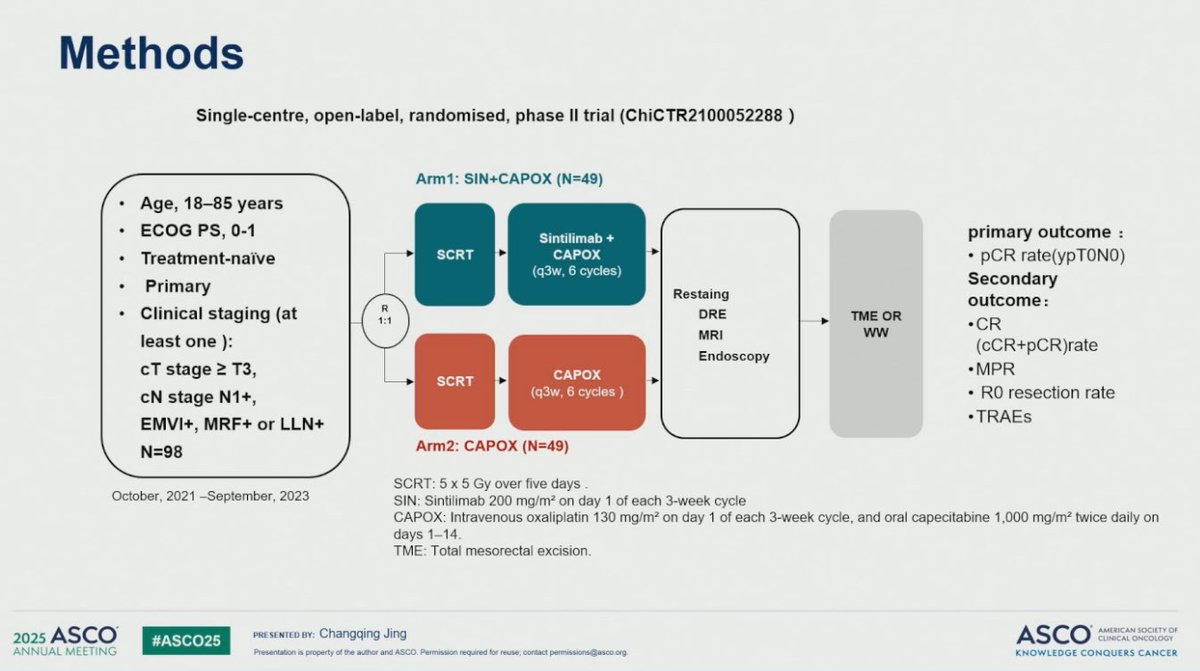
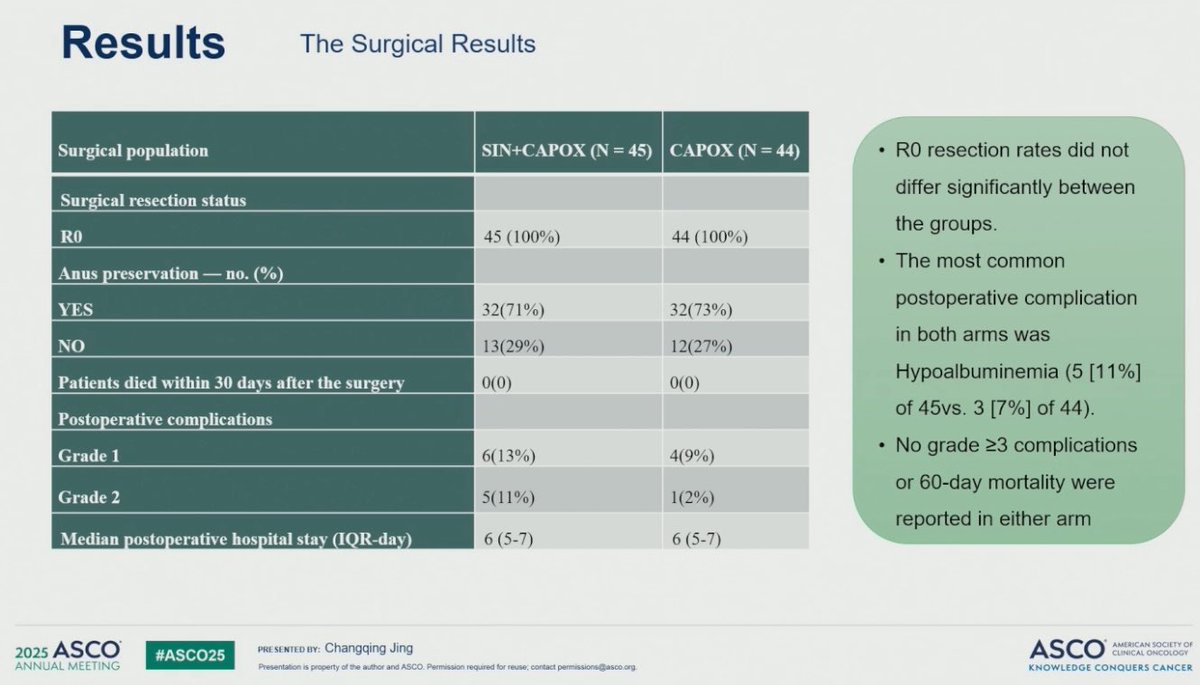
🚨SPRING-01🚨
🔍Locally Advanced Rectal Cancer
RCT:
25 Gy x 5 ➡️ CAPOX - Sintilimab
🔥 Sintilimab demonstrated:
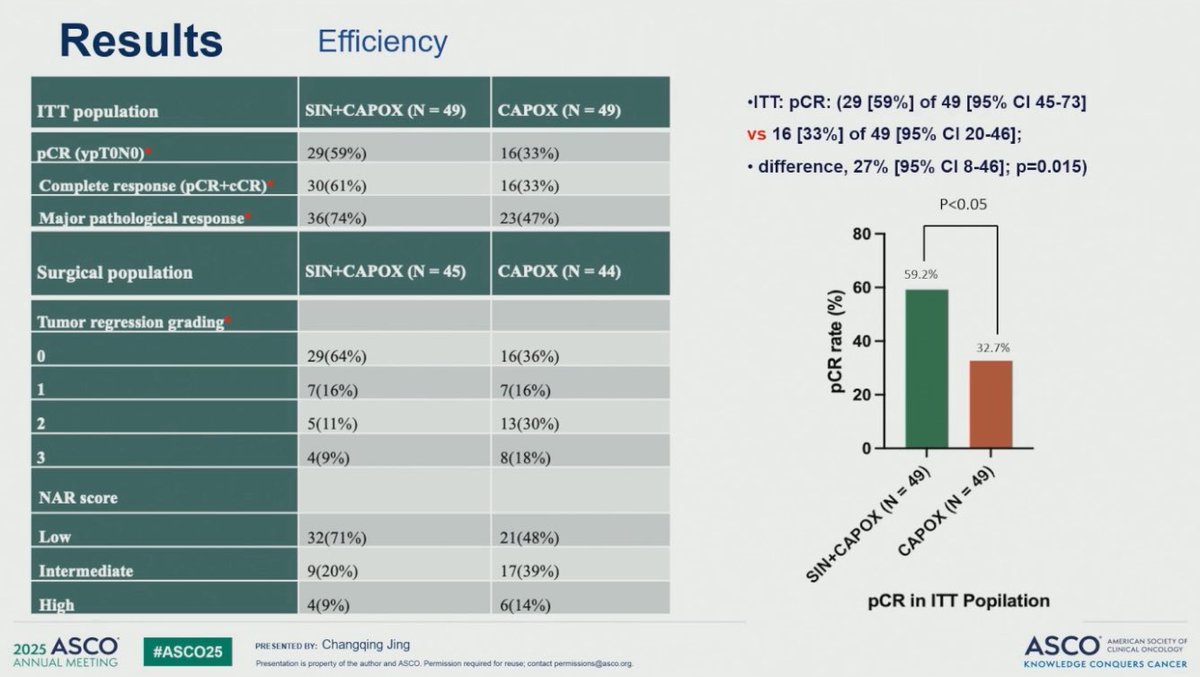
✅⬆️pCR 59% vs 33%
✅No significant adverse surgical or safety signals
Time to explore with organ preserving approaches⁉️
#ASCO25
2
33
70
8,484
Matthew Abrams, MD retweeted

23 May 2025
X-torial: Cleaning up the misinformation about @JoeBiden and #ProstateCancer that I am reading everywhere.
The purpose of this is to provide education from someone who treats and studies PCa for a living, lead the USA @NCCN PCa guidelines, hold leadership in @NRGonc @theNCI @US_FDA and dedicated my career to help men and their families suffering from PCa
@nytimes @WSJ @FoxNews @CNN @NBCNews @Reuters @ASCO @PCFnews @DeptofDefense
26
147
362
89,942
Matthew Abrams, MD retweeted

22 May 2025
✨ Practice-changing for gallbladder cancer?
A randomized phase 3 trial from 🇮🇳 evaluated NACTRT vs NACT in locally advanced GBC (T3/T4, N1, liver infiltration).
Results:
✂️ R0 resection: 51.6% (NACTRT) vs 29.7% (NACT) p=0.01
⏳ Median OS: 21.8 vs 10.1 mo
HR: 0.56 (95% CI 0.37–0.84), p=0.006
⏱ EFS: 10.6 vs 4.9 mo
HR: 0.58 (95% CI 0.39–0.85), p=0.006
5-year OS: 27% vs 18%
Grade 3 post-op morbidity: similar (~18–28%)
Conclusion: NACTRT significantly improves resectability & long-term survival in unresectable LAGBC.
#GIonc #GallbladderCancer #ASCO25 #OncoTwitter @NiuSanford @5_utr @ASCO
4
40
105
9,744
Matthew Abrams, MD retweeted

17 May 2025
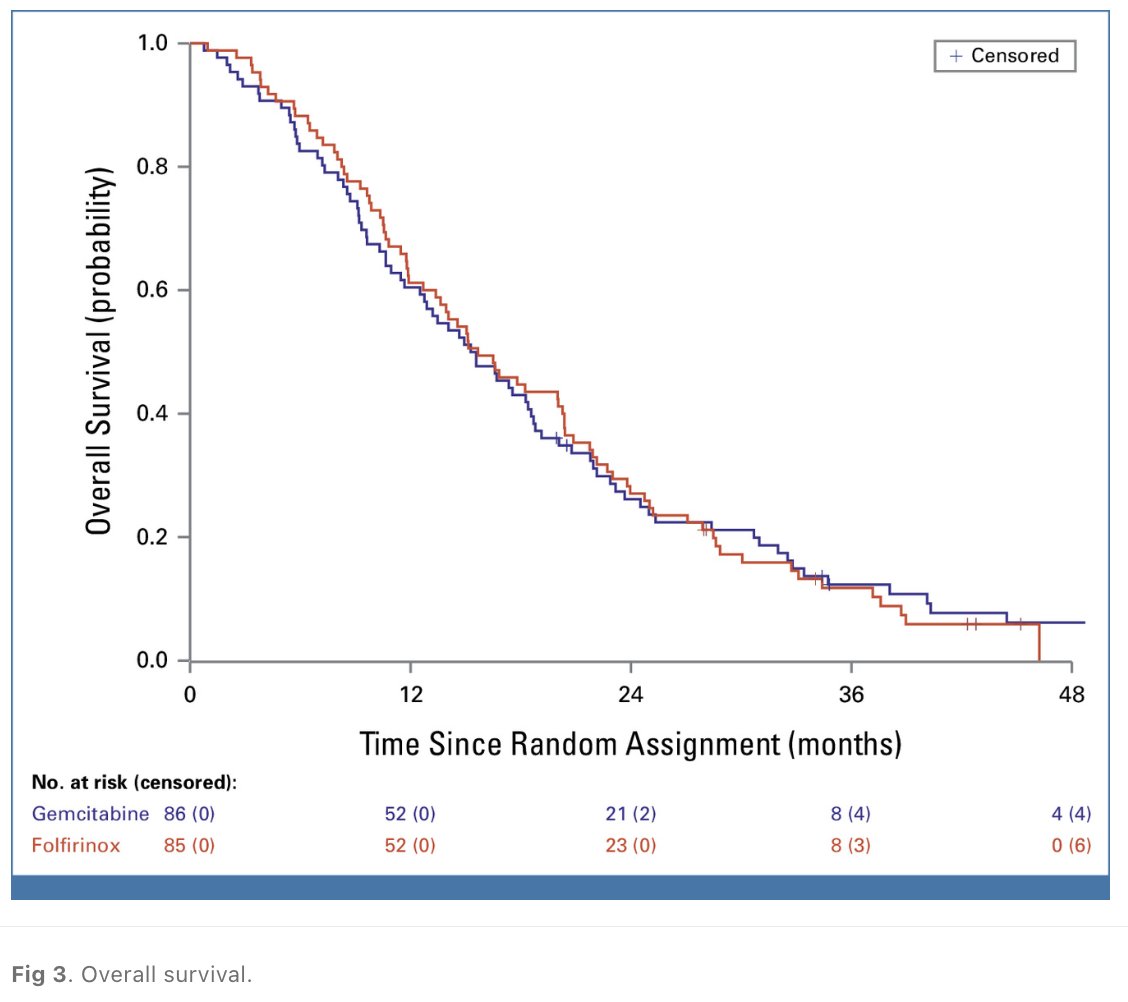
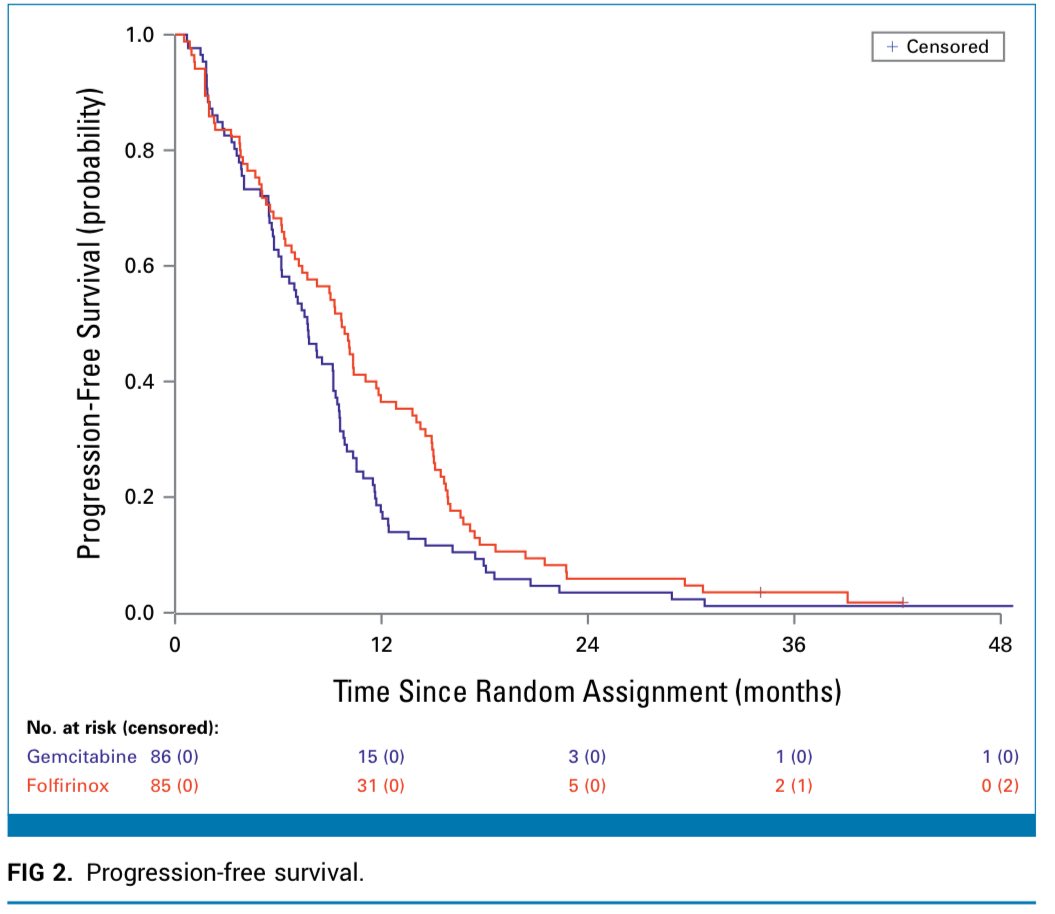
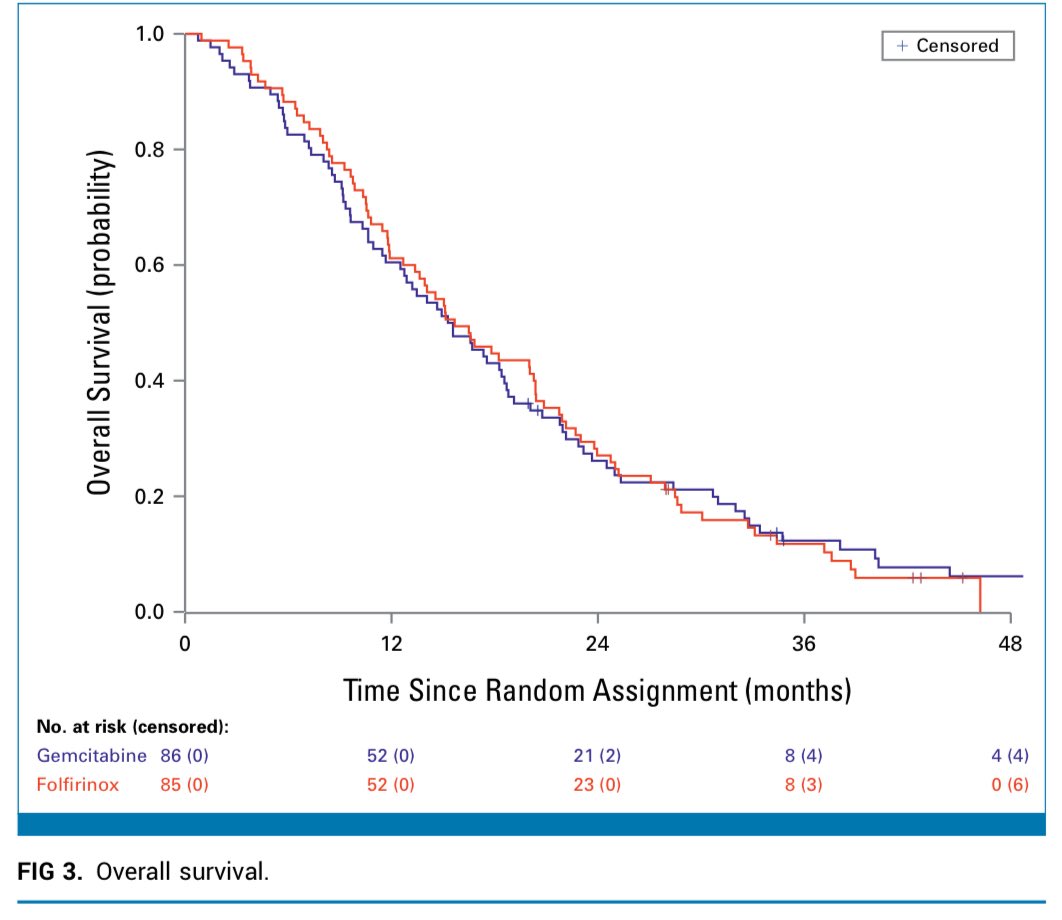
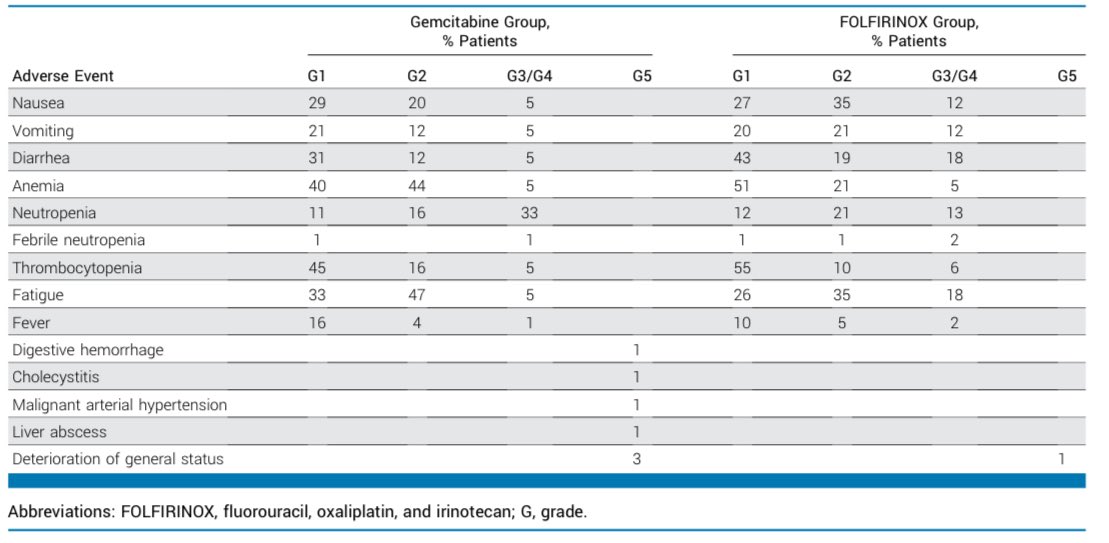
Wow, this trial showed no OS benefit to FOLFIRINOX vs. single agent gemcitabine in locally advanced pancreas cancer (different than adjuvant & metastatic trials - both w OS improvement!)
PFS increased by 2 mo, but this came at cost of increased toxicity, $, treatment burden.
17 May 2025

🚨 NEOPAN - Pancreatic Cancer Update 🚨
In LAPC (locally advanced pancreatic cancer) 🧬:
📊 Trial compared FOLFIRINOX vs Gemcitabine
👥 171 patients, PS ≤1, unresectable cases
📌 Primary endpoint: PFS
📌 Secondary endpoints: OS, QoL, safety
🧪 Results:
🕒 Median PFS:
➡️ FOLFIRINOX: 9.7 months
➡️ Gemcitabine: 7.7 months
📉 HR = 0.7, P = .04 ✅
🕒 Median OS:
➡️ FOLFIRINOX: 15.7 months
➡️ Gemcitabine: 15.4 months
⚖️ HR = 1.02, P = .95 ❌
✅ Better PFS with FOLFIRINOX
🤷♂️ No OS benefit
💊 Well tolerated
doi.org/10.1200/JCO-24-02210
8
53
169
27,964
Matthew Abrams, MD retweeted
4 May 2025
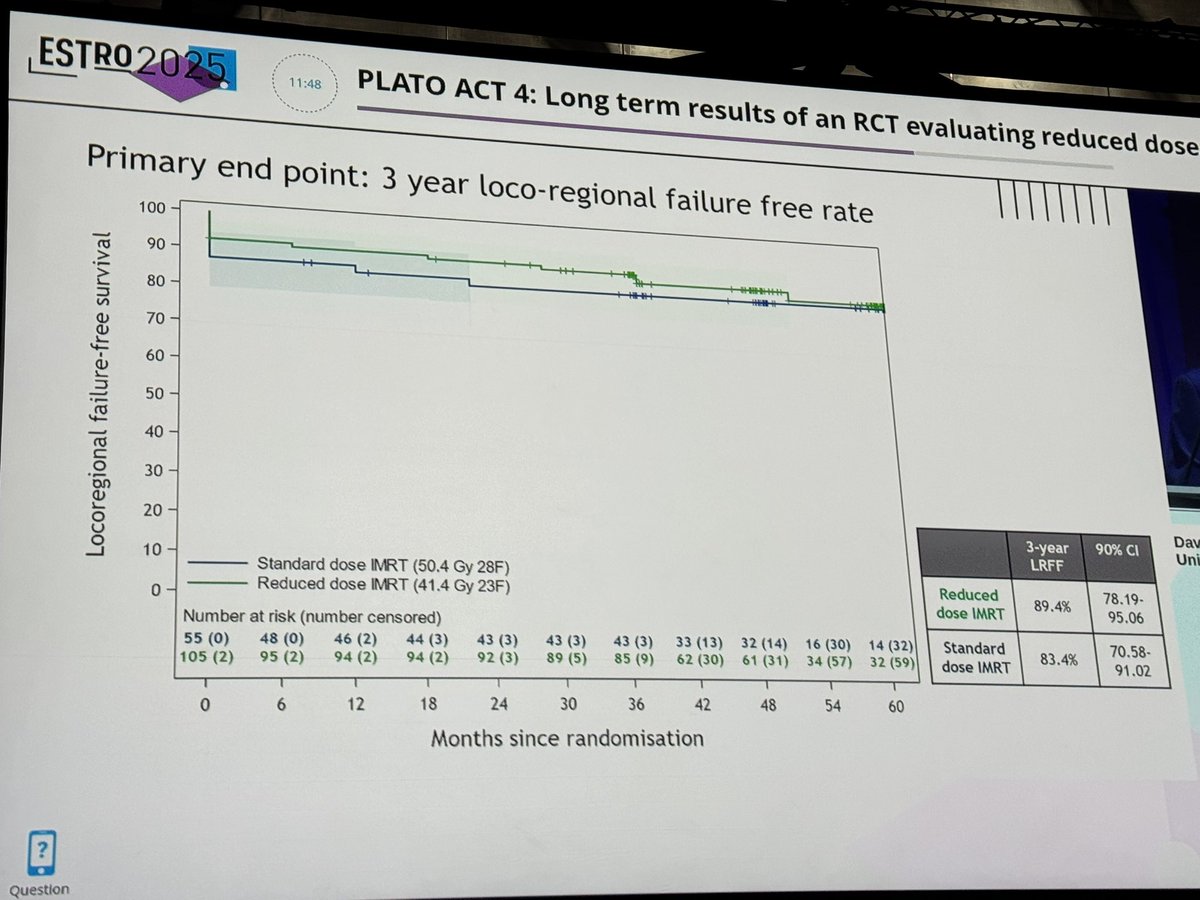
PLATO ACT 4: Ph II RCT of 50.4 vs. 41.4 Gy for T1-2 (<4 cm) N0 anal SCC.
No difference in 3-year local recurrence (primary endpoint) or OS, & better toxicity/QOL with dose-reduction.
Should 41.4 Gy be a SOC option (ahead of Ph III DECREASE trial reporting)?
#ESTRO25
4 May 2025

PLATO ACT 4 results for dose de-escalation in early-stage anal cancer are out! Prof Sebag-Montefiore presents on the plenary stage at #ESTRO24
3-year locoregional failure 16.4% for standard dose IMRT vs 12.4% reduced dose IMRT
Reduced dose IMRT is safe & effective!
#radonc



4
29
63
10,388
Matthew Abrams, MD retweeted

4 Apr 2025
⚡️⚡️NEW STUDY - presented today at #ARS2025 in an oral talk by MS2 Yarelis Roque-Reyes from UCC School of Medicine, PR
🧠💥 Does whole brain RT (WBRT) help patients hospitalized with symptomatic leptomeningeal disease (LMD)?
Our @MountSinaiRO study suggests: rarely — and in reality, it may be more harmful to patients’ quality of life and end-of-life care.
🧵👇 #radonc #neuroonc #endoflifecare #ARS2025
LMD is a devastating CNS complication with 3–6 mo survival. WBRT is often used for palliation — but for patients sick enough to need hospital admission, we asked:
👉 Does it actually help?
We reviewed 58 such patients (2014–2023). Here’s what we found ⬇️
📊 Symptom response after WBRT:
❌ 74% worsened
➖ 21% no change
✅ Only 5% improved
💀 Short-term mortality:
40% at 30 days
60% at 60 days
76% at 90 days
📉 ECOG declined in 79%
⏳ 30% spent >⅓ of their remaining lifespan on treatment — often in the hospital
🎯 Our takeaways
➡️ In hospitalized patients with symptomatic LMD, WBRT provides little to no clinical benefit
➡️ with few exceptions, best supportive care — not burdensome WBRT — should be the priority
➡️time to rethink WBRT in hospitalized pts with LMD?
👏 Congrats to Yarelis Roque-Reyes on her #ARS2025 oral talk!
@sindhu_kunal @MountSinaiRO @QuadShotNews
7
45
85
12,363
Matthew Abrams, MD retweeted

30 Mar 2025
When I was a resident, Harvard took money from Krupp I naïvely thought this has to be a different company/family than the one that funded the third Reich. This was in the early 70s. I was wrong should’ve known.
1
7
704
Matthew Abrams, MD retweeted

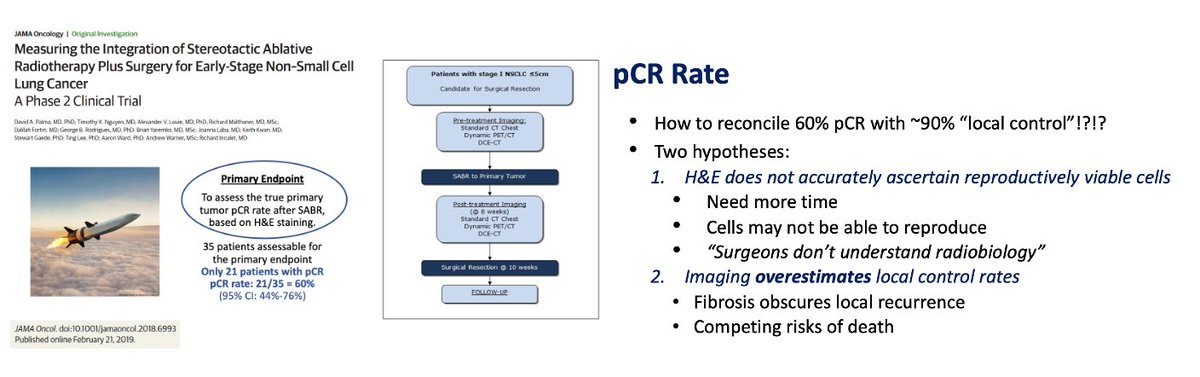
10 Mar 2025
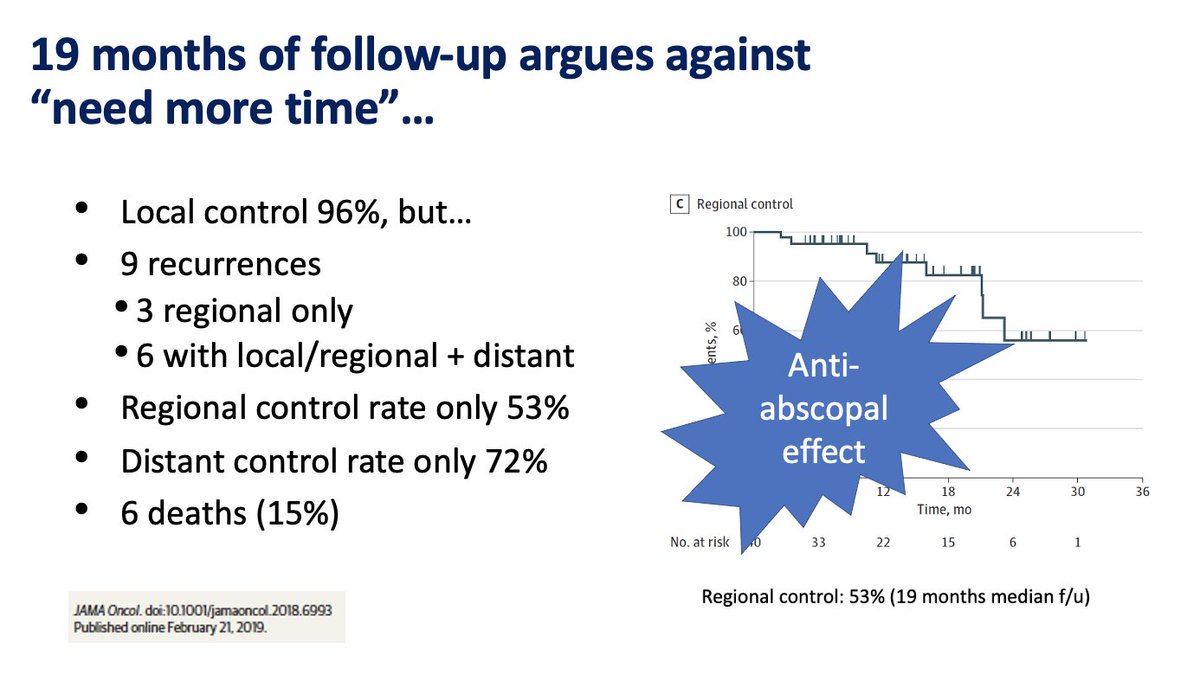
All due respect, but it is relatively common knowledge that radiotherapy works for many months after it has been delivered. One must not conflate pCR, especially short term pCR, after radiotherapy as a surrogate for LC or residual tumor. This has been well demonstrated across many disease sites.
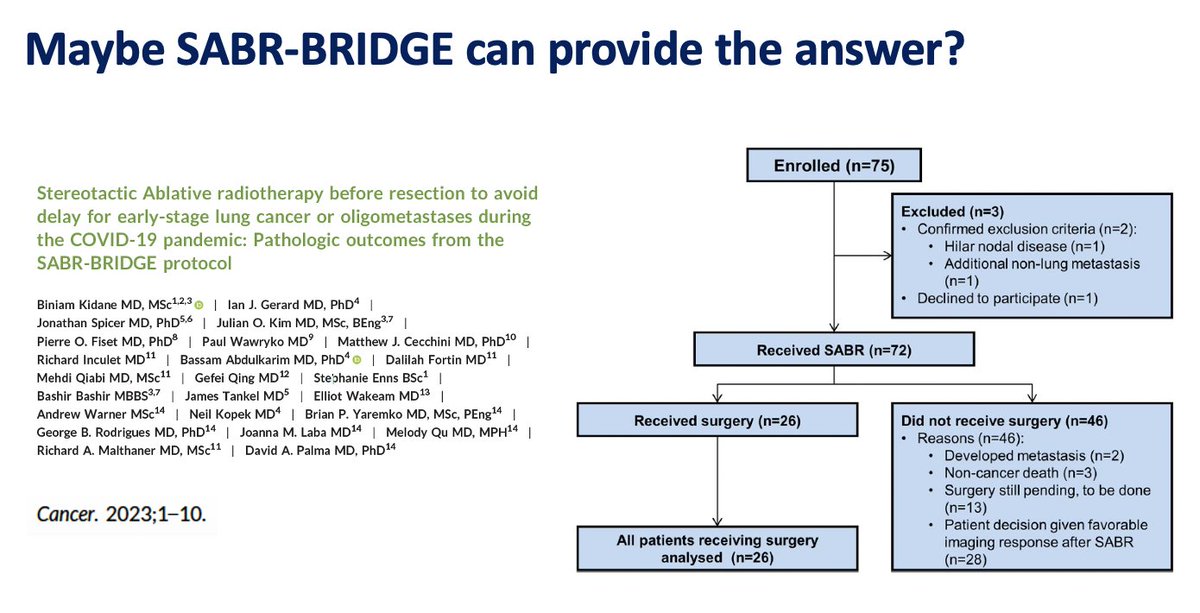
For reference, MISSILE cut at 10 weeks s/p RT while SABR-BRIDGE cut at 4.5 mo post-SBRT (range 2-17.5 mo).
Take anal cancer, for example. When biopsied at 3 months, if positive, 3/4 of patients with positive biopsy converted to negative biopsy by 6 months. Of course, the whole specimen was not removed, so there is a potential there could be "residual," but robust data supports very high cure rates in the long term (~85%, generally speaking) with CCRT alone for anal SqCC.
Receipt here:
pmc.ncbi.nlm.nih.gov/article…
Take prostate cancer, for example. Post treatment biopsies are essentially not recommended until two years after radiotherapy.
Receipt here:
pubmed.ncbi.nlm.nih.gov/3355…
Take RCC, for example, where routine post-treatment biopsy is not recommended as it is not predictive of patient outcome.
Receipt here:
pubmed.ncbi.nlm.nih.gov/3818…
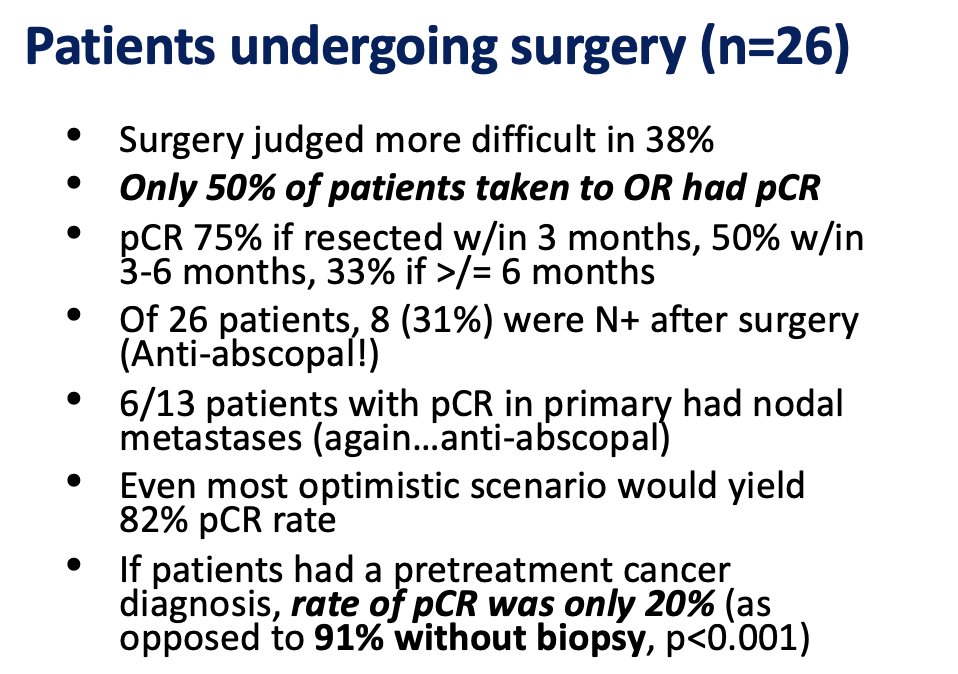
So, why should lung cancer be any different? Similarly to RCC, if post-treatment biopsies after lung RT do not predict outcomes, is this meaningful to patients or multidisciplinary discussion? Radiotherapy can also induce cellular senescence, where the cell will no longer divide but can still make proteins at low levels. We must not perpetuate misinformation suggesting short-term pCR is predictive of patient outcomes after RT, as it harms existing biases against radiotherapy.
I have seen this fallacy posted repeatedly on X, so I felt it was time to address this head-on.
9 Mar 2025

Unfortunately, MISSILE and SABR-BRIDGE didn't show the same w/ full pathology...clearly we need more research and effects may be tumor/site specific!
3
16
73
9,303

🎙 Randomized Trial 🚨: SBRT vs. RFA for Recurrent Small HCC—Is It Time to Rethink Local Treatment? @OncoAlert
🔬 Study Highlights:
📌 Phase III trial, 166 👥 with recurrent HCC (≤5 cm, single lesion).
📌 Randomized to RFA (n=83) or SBRT (n=83)
Key Outcomes:
✅ Local progression-free survival (LPFS):
•2-year LPFS: 92.7% (SBRT)🏆 vs. 75.8% (RFA) (HR: 0.45, p=0.014).
✅ Progression-free survival (PFS):
•Median PFS: 37.6 months (SBRT) vs. 27.6 months (RFA) (p=0.19).👌
✅ Overall survival (OS):
•2-year OS: 97.6% (SBRT) vs. 93.9% (RFA) (p=0.83).👌
✅ Safety: Comparable acute and late adverse events.👍
📣 Implications for Practice:
SBRT demonstrated ⬆️ local control while maintaining similar safety and OS compared to RFA.
5
80
184
18,796
Matthew Abrams, MD retweeted
5 Dec 2024
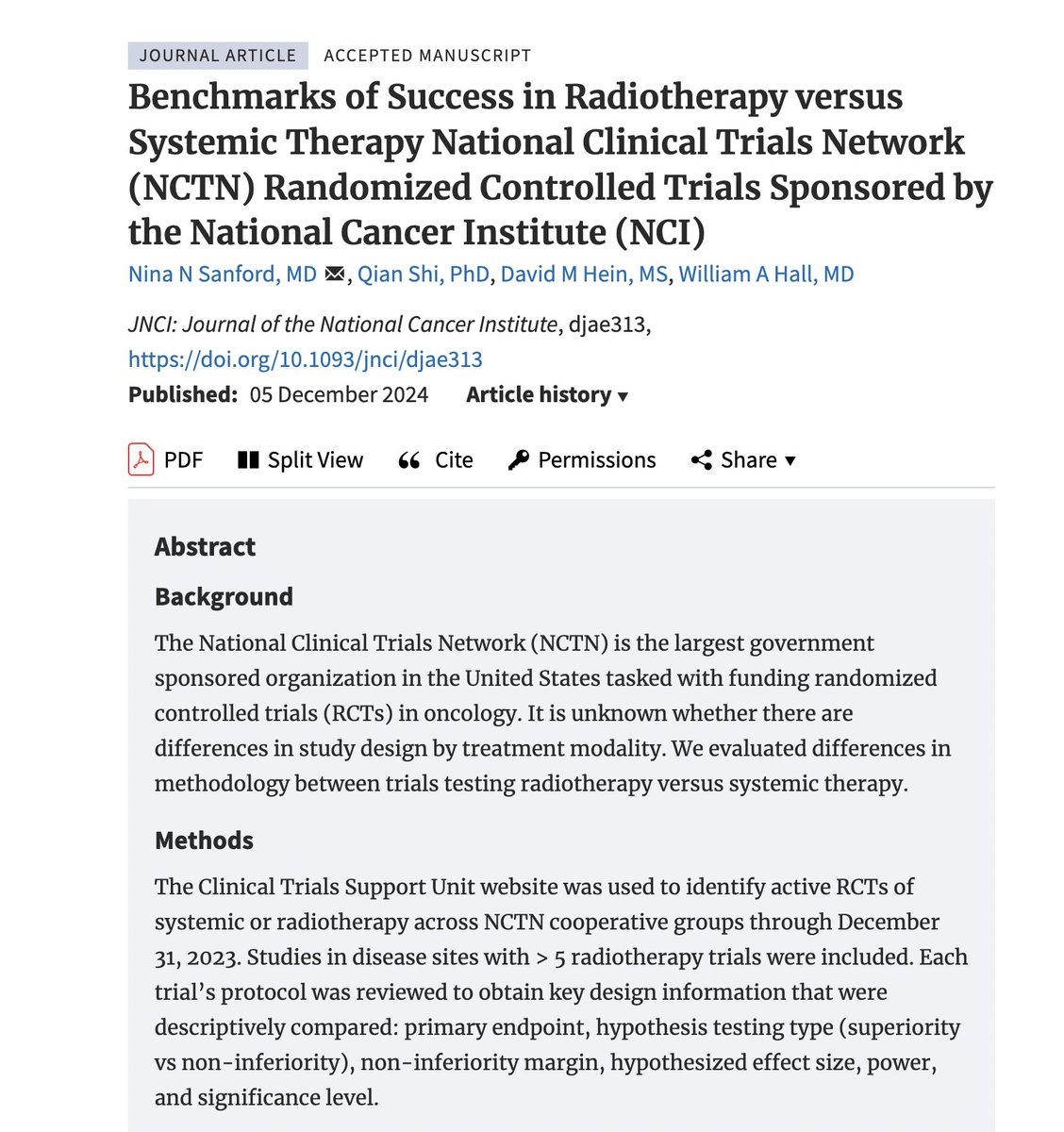
Our comprehensive assessment of NCI cooperative group trials is out in @JNCI_Now!
If you are involved or enrolling in coop trials, please consider reading.
A 🧵of our major findings. 1/12
academic.oup.com/jnci/advanc…
4
58
111
22,803
Matthew Abrams, MD retweeted

23 Oct 2024
BIDMC’s Rectal Cancer Program has achieved accredited status, the first program in Massachusetts to reach this milestone.
#BIDMC #BILH #rectalcancer
1
20
2,541
Matthew Abrams, MD retweeted

30 Sep 2024
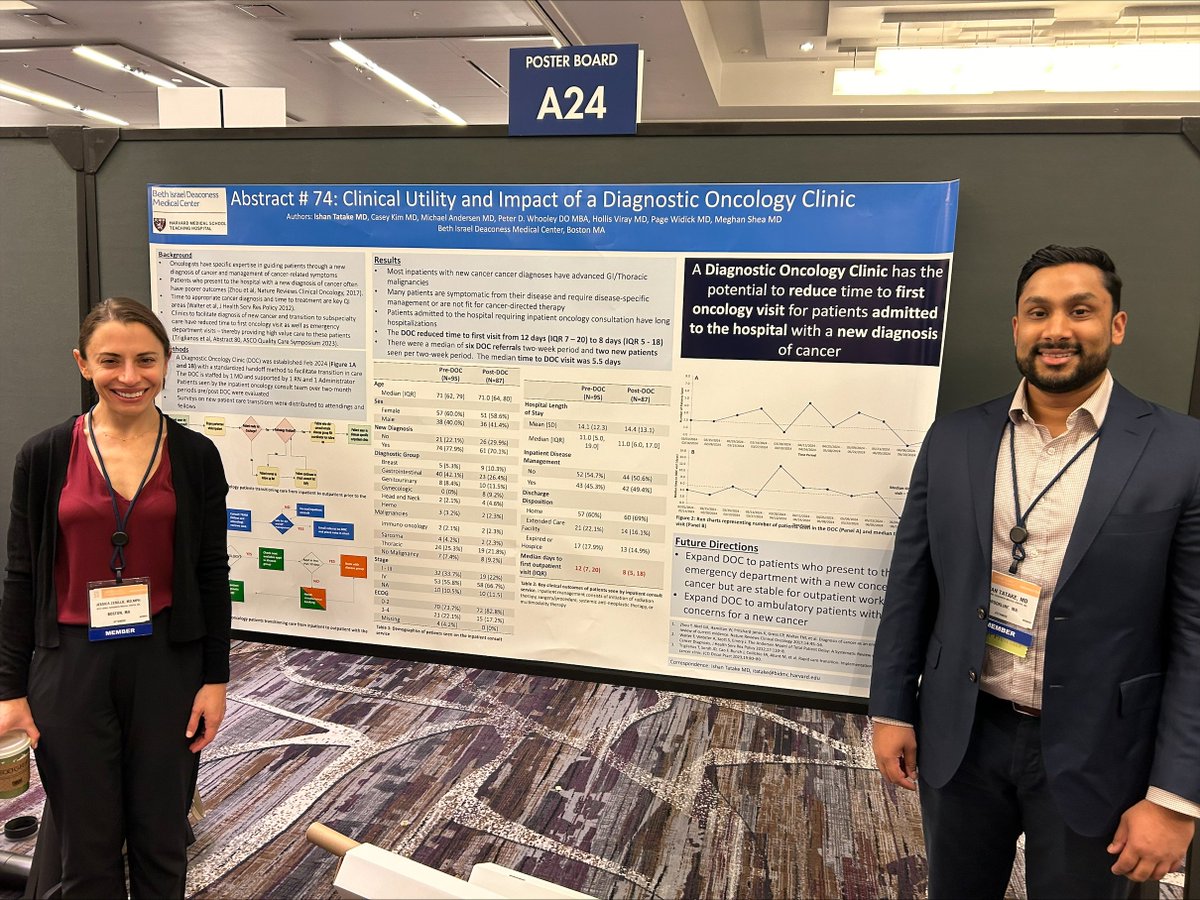
⭐️@ishtatMD @BIDMC_HOFellows shares findings on how a diagnostic oncology clinic improves patient outcomes, including the potential for faster handoffs to a first oncology visit for patients admitted to the hospital with a new cancer diagnosis. #ASCOQLTY24
4
12
1,249
Matthew Abrams, MD retweeted
26 Sep 2024
Unresectable HCC (median tumor diameter 10cm, 60% MVI) treated w IO SBRT (N=63):
-46% achieved complete response, much higher than prior trials of IO alone: atezo/bev (CR 5.5% IMBRAVE150) & STRIDE (3.3% CR)
-CR associated w better OS (3yr 76% vs. 28%)!
jamanetwork.com/journals/jam…
6
55
129
17,770
Matthew Abrams, MD retweeted
23 Sep 2024
Some trial caveats (small N, no MMR status, chemo could be longer than XELOX x 4)…
But this RCT is a good reminder that for rare case of unresectable colon cancer, chemoRT should be considered for downstaging to facilitate R0 resection.
It is even in 2024 NCCN guidelines 🙏!
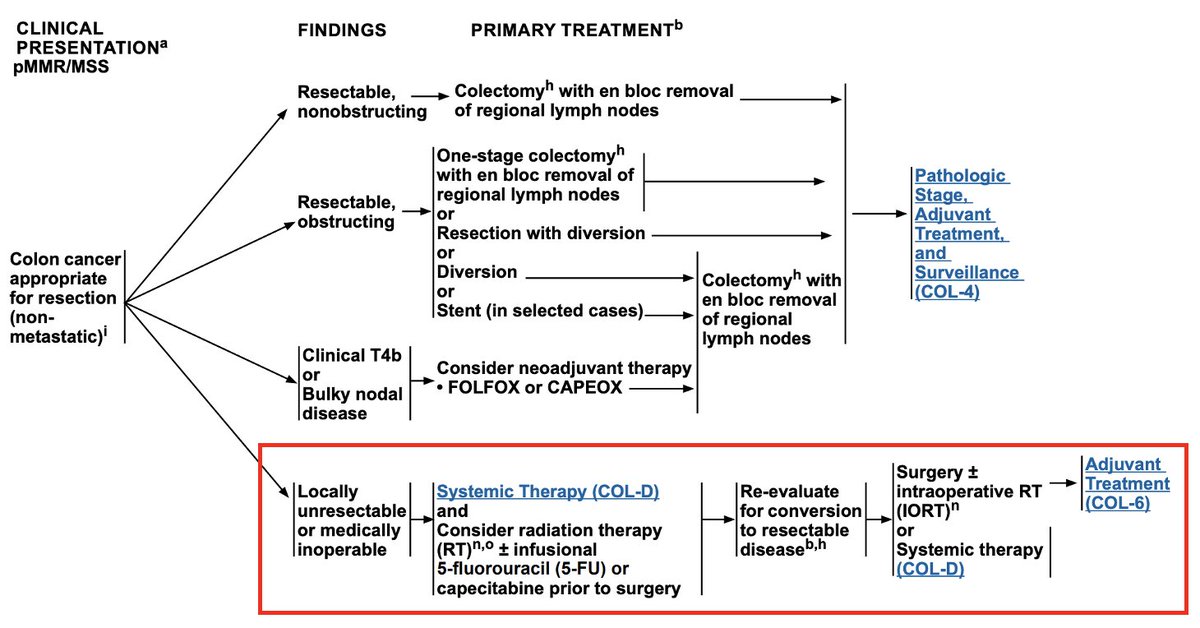
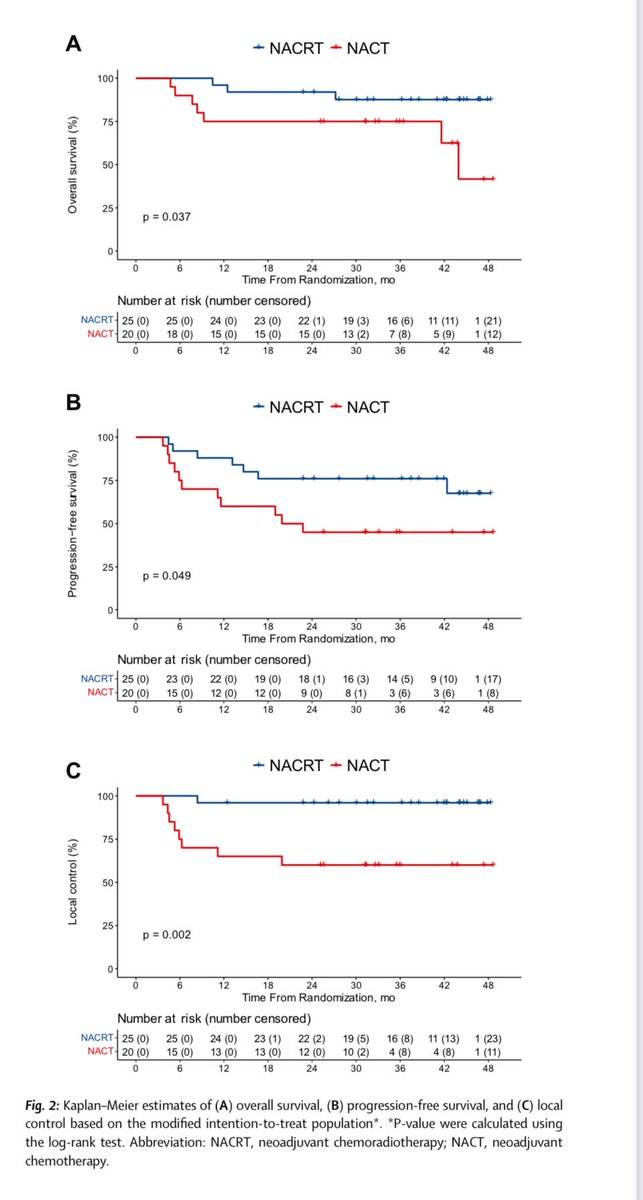
23 Sep 2024

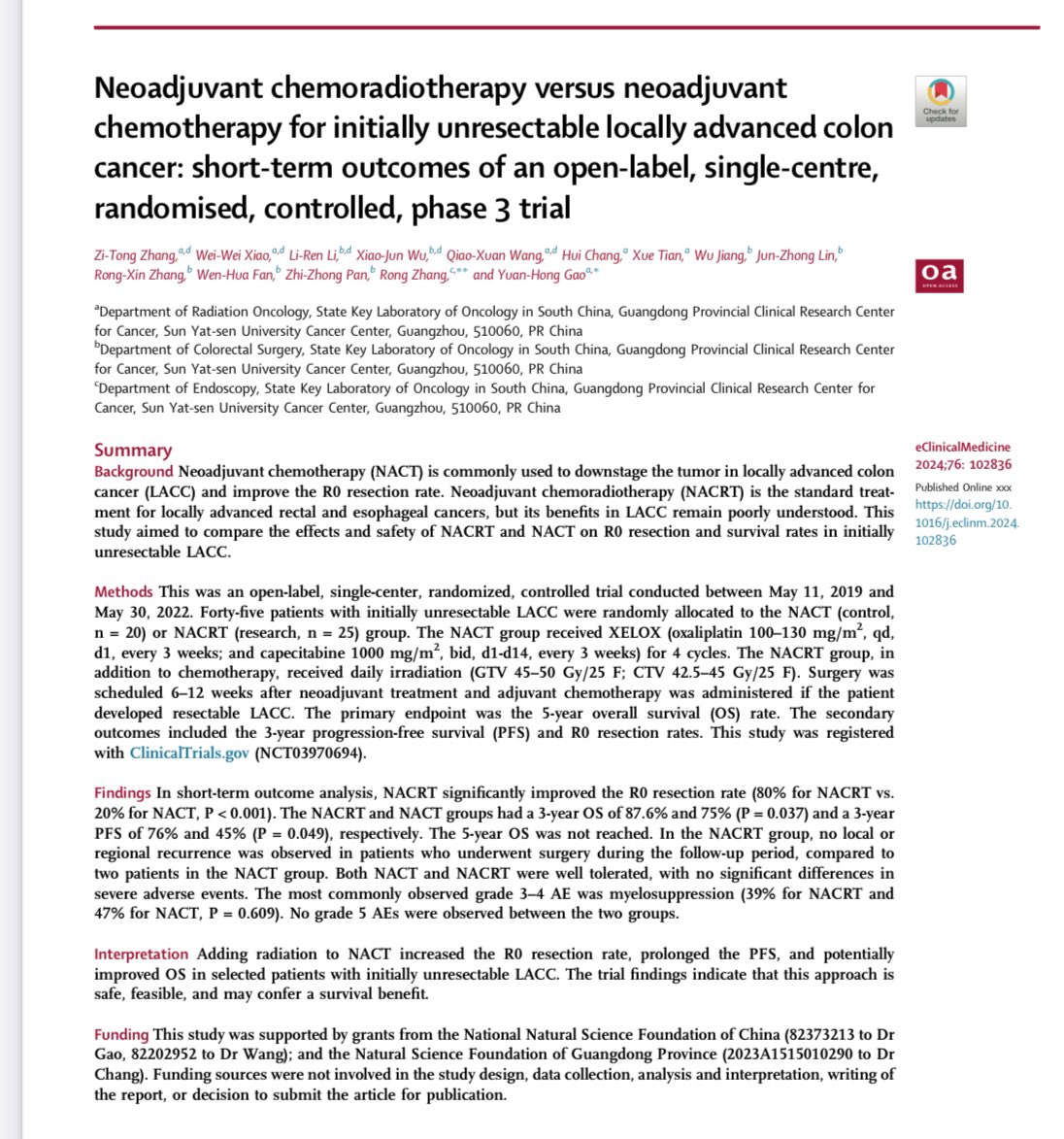
☢️Neoadjuvant CRT vs. ChT for initially unresectable locally advanced "Colon" cancer
@eClinicalMed
➡️45 patients
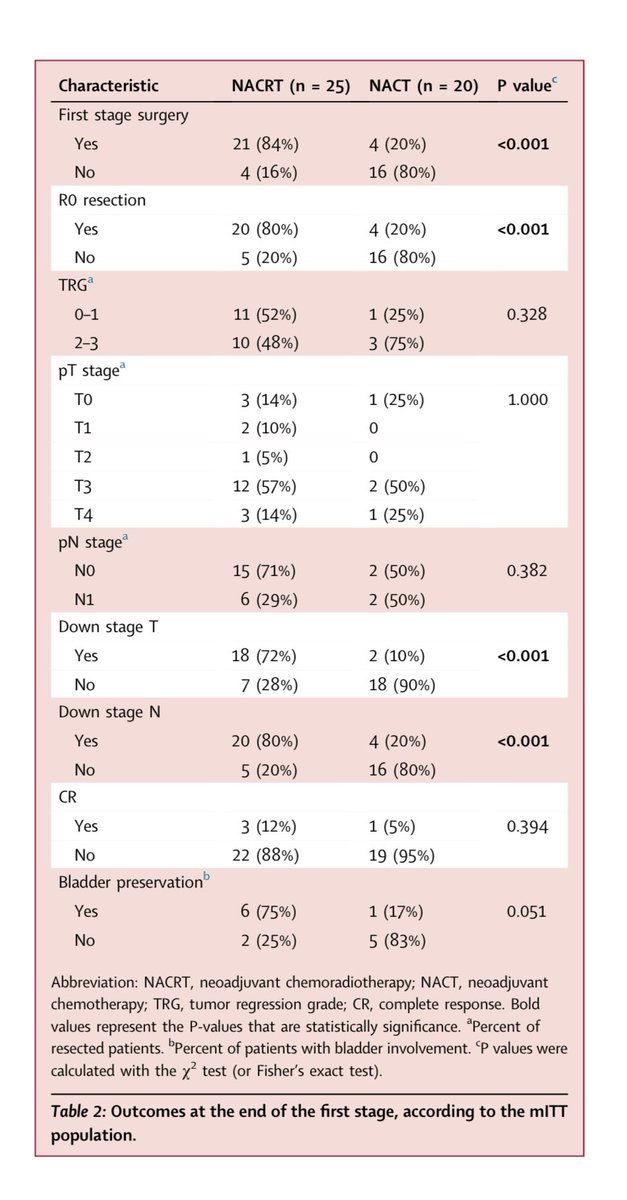
✅R0 resection: 80% vs. 20%, P < 0.001
✅3-year PFS: 76% vs. 45% , P = 0.049
✅3-year OS: 87.6% vs. 75% , P = 0.037
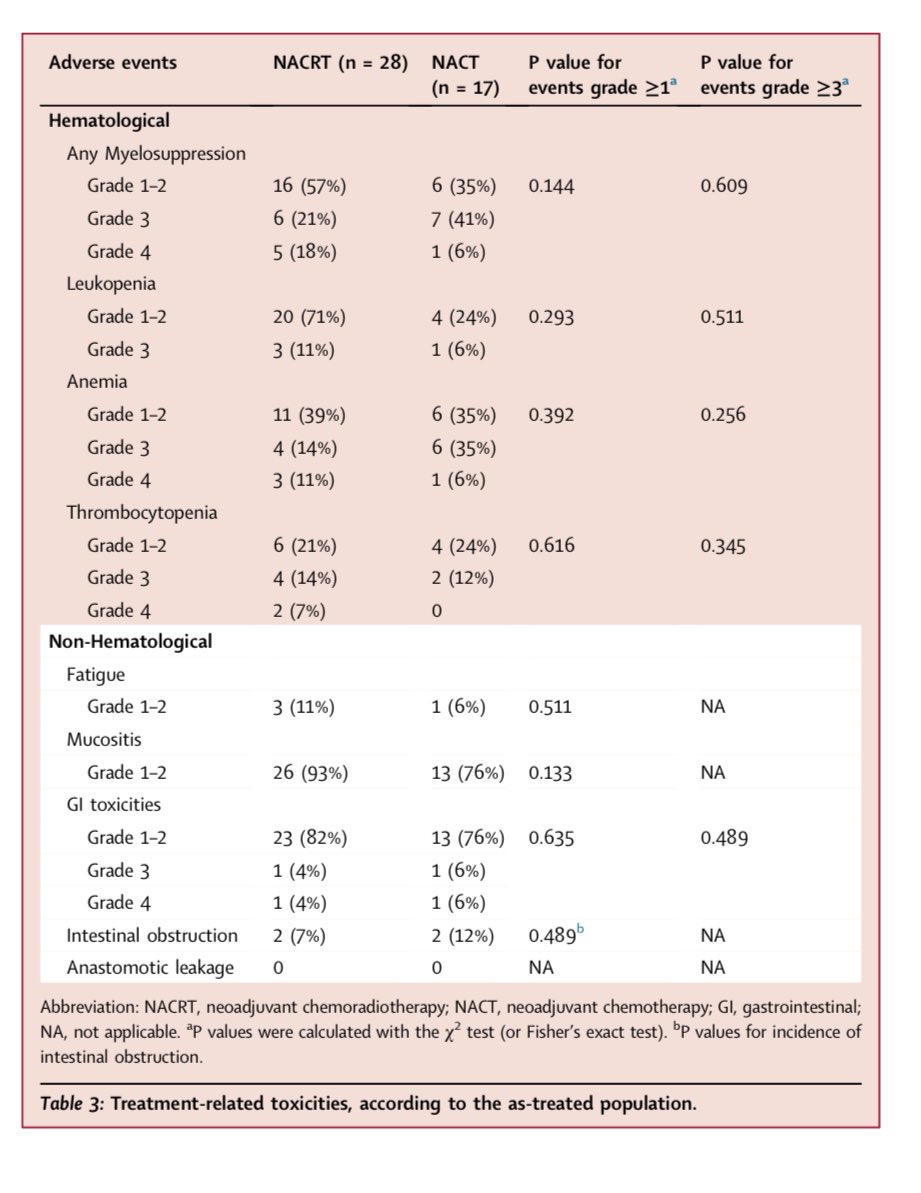
✅No differences in severe AEs
❗️Study was terminated prematurely because of R0 resection benefit of CRT
👉doi.org/10.1016/j.eclinm.202…
@TheLancetOncol @TheLancet @LancetGastroHep @myESMO @OncoAlert #cancer #oncology #MedX
22
75
14,915
Matthew Abrams, MD retweeted
14 Sep 2024
We should not be excited about #LEAP012. TACE has the worst local control among all LC modalities of any disease site, with a ~50-60% LF rate.
In 2024, TACE should be reserved for special cases (e.g., caudate lobe tumors where radiotherapy risks complicate liver transplant), but otherwise, it should be phased out entirely. #ESMO24
Anyone with cancer being considered for TACE should consult their local radiation oncologist to discuss the data and explore all available options. #radonc
2
16
52
11,618