
Radiation Oncologist | MSc Physics | PhD AI & Quantum Computing / Oncologic Imaging | Views are my own
Joined January 2012
- Tweets 1,277
- Following 581
- Followers 439
- Likes 2,581
49 Photos and videos



Tony Felefly retweeted

Jun 10
RTOG 0848 forest plot (Fig 3): RT*chemo interaction p=0.414. Gem alone, gem combos, gem erlotinib — all consistent. Zero evidence RT benefit varies by chemotherapy backbone. Calling for a new FOLFIRINOX trial before using RT in pN0 patients inverts the burden of proof.
1
6
3,302
Tony Felefly retweeted

Jun 10
RTOG 0848: neg overall, but benefit in pN0 (adj chemoRT improved OS 5yr 48% v 29%).
Caveats: small N0 subgroup (N=91), gem chemo, pre neoadj era.
My main takeaway: RT has role in (select) resectable PDAC & future trials need to focus on biologically favorable subset. @OncoAlert
Jun 10

Adjuvant Chemotherapy /- Chemoradiotherapy for Adenocarcinoma of The Pancreatic Head: Results of The Radiotherapy Randomization of NRG Oncology/RTOG 0848 | Journal of Clinical Oncology ascopubs.org/doi/10.1200/JCO…
3
25
68
13,288
Tony Felefly retweeted

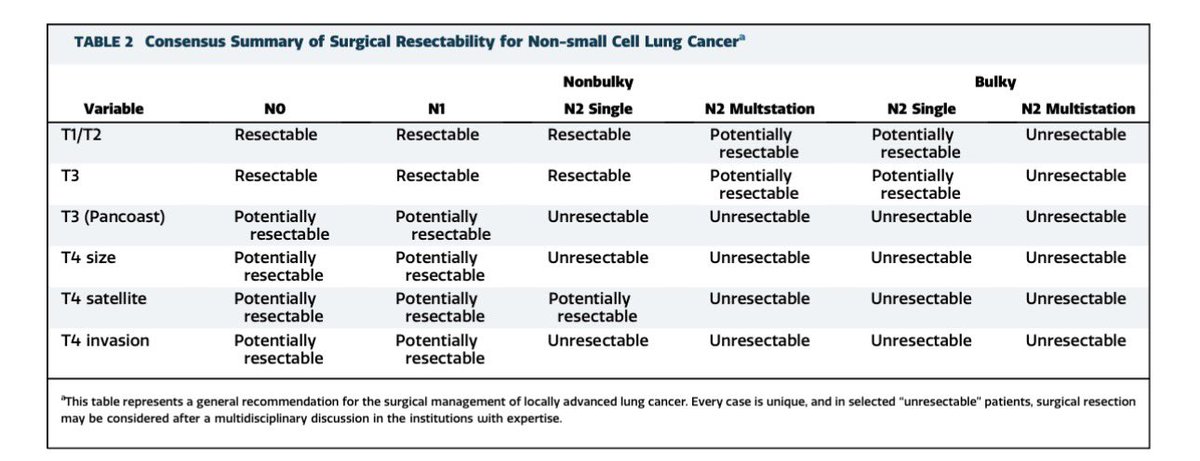
Definitive Radiotherapy to the Primary Tumor in Stage IV NSCLC: A Consensus Statement From the International Association for the Study of Lung Cancer Advanced Radiation Technology Subcommittee - Journal of Thoracic Oncology jto.org/article/S1556-0864(2…
31
66
8,655
Tony Felefly retweeted

Also, the use of Dotatate PET scan in addition to MRI is really useful in meningiomas. I’ve been taking some of these “bad actor” meningiomas to 66-70 Gy.
Jun 8

FIRESTORM: improved PFS with dose-escalated postop RT >= 66Gy/33fr for high-risk meningiomas
redjournal.org/article/S0360…
@Raj_Singh_MD @joshuapalmermd @PDBrownOnc
1
3
442

Jun 8
FIRESTORM: improved PFS with dose-escalated postop RT >= 66Gy/33fr for high-risk meningiomas
redjournal.org/article/S0360…
@Raj_Singh_MD @joshuapalmermd @PDBrownOnc
2
15
1,203
Tony Felefly retweeted

Jun 7
No, 30/5 is the default unless we can’t meet brain minus CTV V30<10.5 cc then consider dropping the 27.5 or rarely 25/5. If 25/5 with residual tumor then boost on GK with an additional ~5/1
1
1
6
287
Tony Felefly retweeted
Jun 7
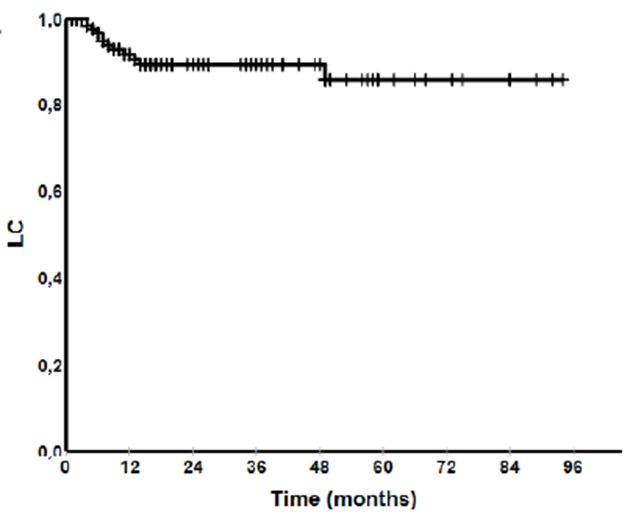
This is our approach at Sunnybrook with excellent LC
1
1
2
223
Tony Felefly retweeted

At @DukeRadOnc we did 27.5 Gy in 5 fx to PTV. 2mm margins from cavity to PTV.
1
4
201
Tony Felefly retweeted

Jun 7
I typically use 27 in three. For large lesions I’ll use either 30 in five or 32.5. I was impressed with their results with such a relatively lower dose. What do you typically use?
2
1
6
536
Tony Felefly retweeted

This is what we do at @pmcancercentre and SIB to 30Gy for any gross tumor
1
4
196
Tony Felefly retweeted
Jun 7
Is 25Gy/5 to post-op cavity after resection brain met effective?
Yes, according to this study
~90% LC at 1 and 4 years
Symptomatic Radiation Necrosis 3%
3
22
47
2,509
Tony Felefly retweeted

Jun 4
Among the thousands of abstracts presented at #ASCO26, one that generated a lot of attention was by an amazing team I'm fortunate to work with at the Los Angeles and St. Louis VA medical centers. Not only did our work get an oral presentation, but we also got an ASCO Daily News highlight. Likely because of the scale and fidelity of the analysis on a 1 million patient cohort with structured smoking history. @BrendanHeiden
dailynews.ascopubs.org/do/ne…
3
6
18
1,969
Tony Felefly retweeted

May 31
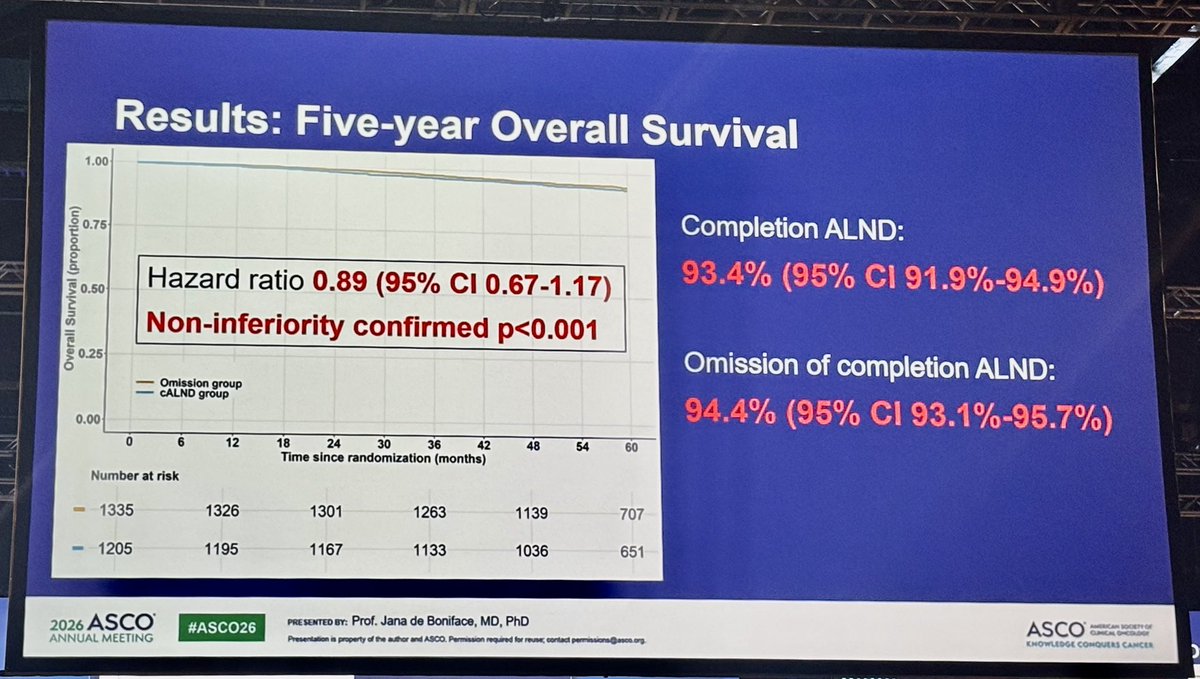
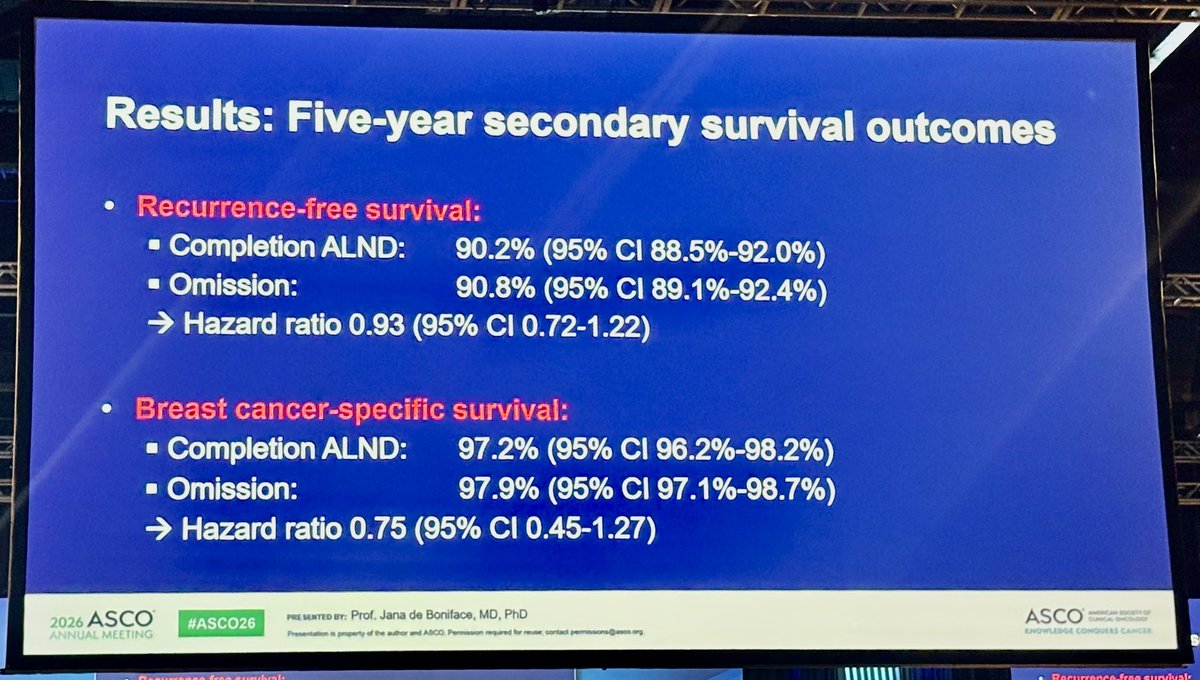
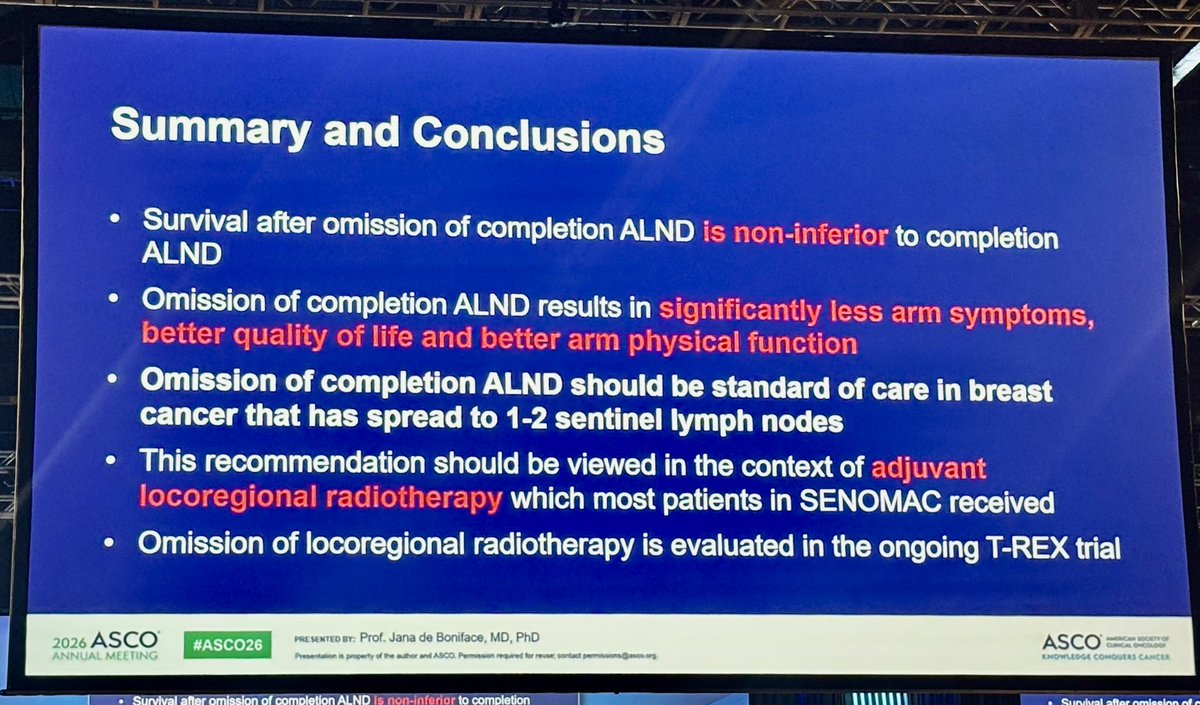
Omission of ALND in #breastcancer with 1-2 sentinel nodes macrometastases - OS from SENOMAC trial - Jana de Boniface #ASCO26
Recommendation should be viewed in the context of postoperative locoregional #radiotherapy
@OncoAlert #OncoAlert
2
15
38
2,596
Tony Felefly retweeted

Maybe cite our data - we have the largest series! pubmed.ncbi.nlm.nih.gov/3557…. It’s a made up
criterion to help get urologists to buy into referral by making them do extra stuff. No proven benefit and possible harm eg perforation.

In clinical practice I still see a lot of push back if you downplay the role of TURB as part of treatment. Some clinicians view it as an integral part of bladder sparing. No (maximal) TURB, no chemorads.
2
9
27
6,613
Tony Felefly retweeted

OK so some of my thoughts about #PROTEUS, presented at Plenary session during #ASCO26
💠This was a tough trial to do, congratulations to the team for getting this done! 💪
🔷I think this is going to muddy the waters, esp for us rad oncs who get sent pts post-prostatectomy 1/n
1
11
29
8,601
Tony Felefly retweeted
To clarify a few things about this thread ⬇️
🔸Not only do we need think about this in the context of upfront tx considerations for men with HR PCa...
🔸Inevitably, there are going to be pts tx'd this way. What I am referring to is, what do we (rad oncs) do after? 1/n

2
1
6
2,158
Tony Felefly retweeted

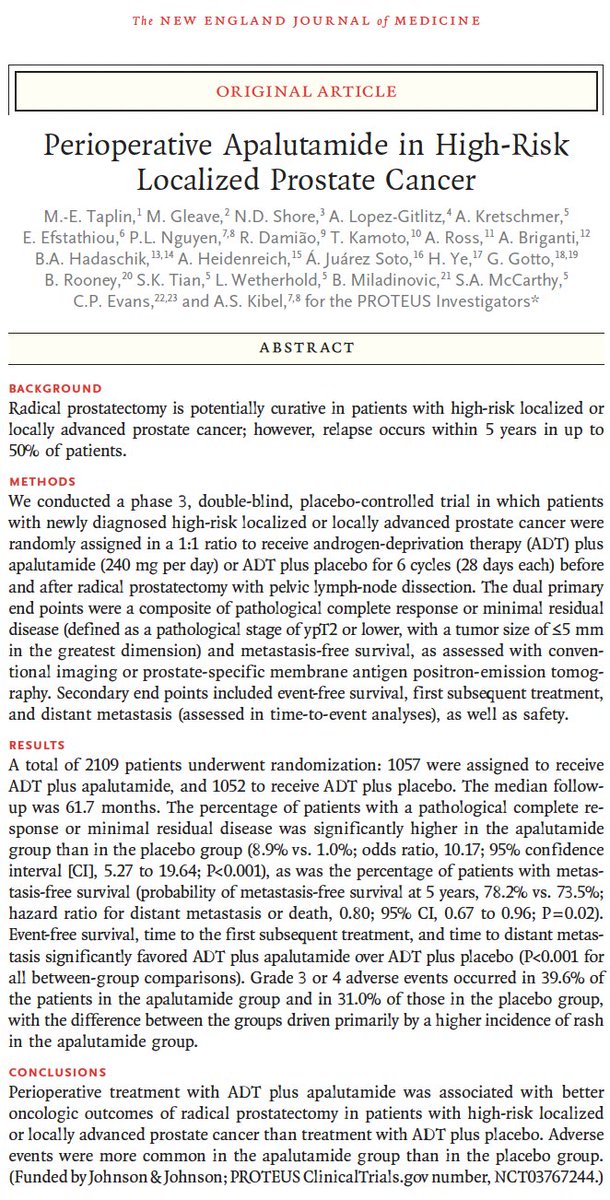
🚨 PROTEUS: perioperative apalutamide moves into high-risk localized #prostatecancer
Just out in @NEJM
🧬 2109 men w/ high-risk localized or locally advanced PCa randomized to ADT apalutamide vs ADT placebo around radical prostatectomy.
🎯 Both stated primary endpoints met.
⚠️ But the trial deserves nuance. Thread 🧵
#ASCO26 @ASCO @PCF_Science
4
28
64
6,586
Tony Felefly retweeted

May 31
Trials in localized prostate cancer are incredibly difficult to pull off, especially given the rapidly changing imaging and therapeutic landscape, so major congrats to the investigators.
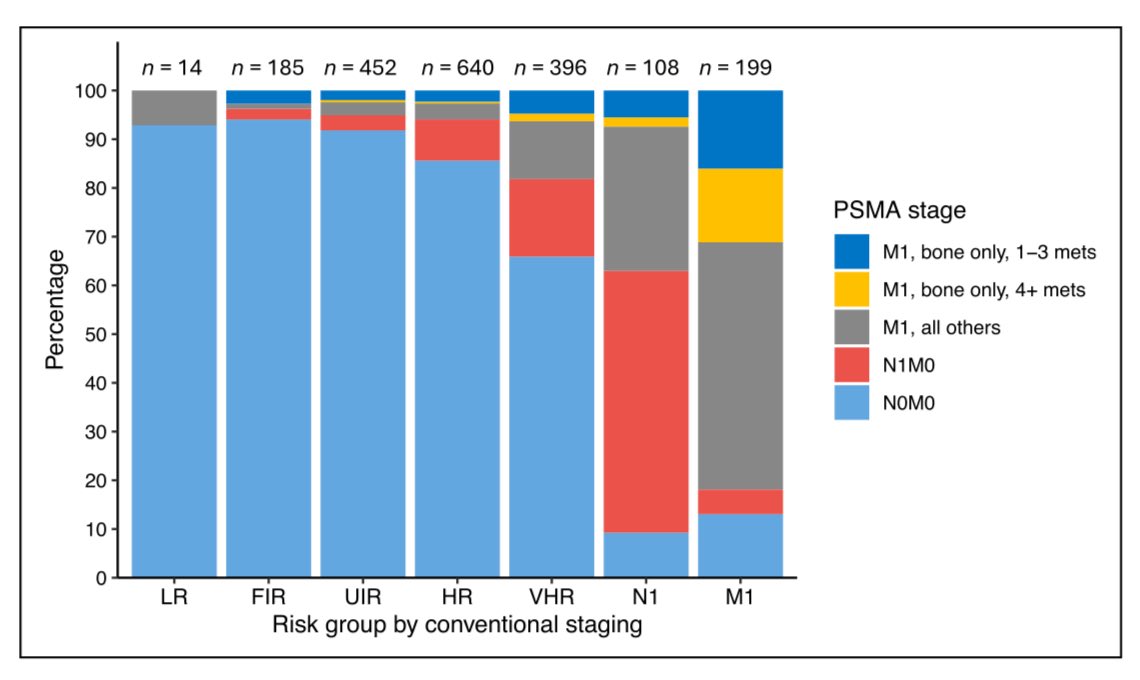
For me, top line results: small MFS benefit when MFS is defined by either conventional imaging or PSMA PET. No MFS benefit by conventional imaging.
Critically, there were significant differences in PSMA PET utilization. Post hoc analysis showed that 686 patients (64.9%) in the apalutamide group and 755 patients (71.8%) in the placebo group underwent PSMA PET at least once.
That difference is greater than the absolute MFS benefit (when MFS is defined by either conventional or PSMA imaging) and may mean that the MFS benefit is confounded by the differential use of PSMA PET at biochemical recurrence. The extent of that confounding will depend on the comparative probability of detecting Mets at BCR using PET vs conventional imaging in the trial cohort. Would be interested in that data.
Does PROTEUS change practice? Given the above, I'm not sure the argument is there to go from RP alone (the current standard) to RP ADT ARPI. Will be interested in the substudy results.
#ASCO26 #radonc #medtwitter #pcsm
nejm.org/doi/full/10.1056/NE…
7
18
66
6,588
Tony Felefly retweeted

May 31
The real question is the Enzarad data, which is not a subgroup analysis like STAMPEDE.
STAMPEDE is hands down my favorite trial ever, but important to note that the M0 analysis was a subgroup analysis and not all patients even had local therapy. Some patients had PSAs in the 1000s.
Enzarad a bit more relevant where MFS and OS were not significantly improved in N0M0 patients. Just like PROTEUS MFS and OS were not improved by conventional imaging.
Given we now often get PSMA PET/CT upfront for staging, ARPIs in N0M0 patients have no proven role.
May 31

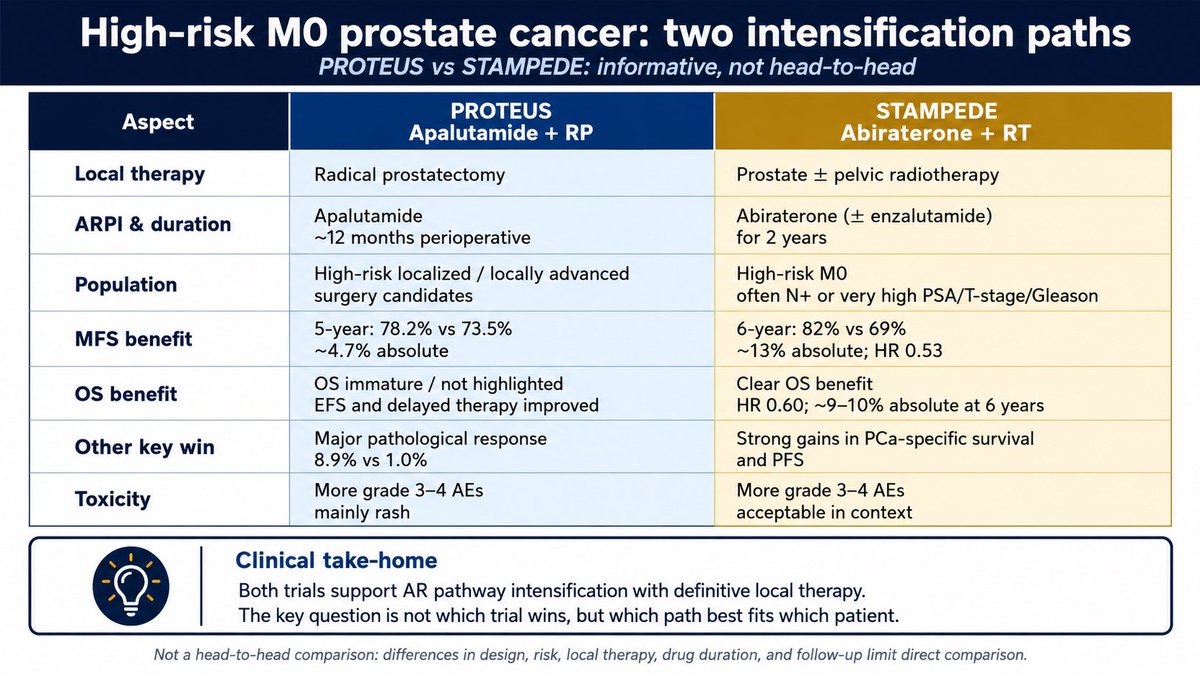
PROTEUS and STAMPEDE both support ARPI intensification in high-risk M0 prostate cancer, but across different designs and local treatments.
The real advance is not “which wins?”
It is “which patient, which path?”
#ASCO26
@DrChoueiri @TiansterZhang @CathyEngMD @montypal @tompowles1 @brian_rini @cdanicas @GlopesMd @PGrivasMDPhD @nataliagandur @yekeduz_emre @neerajaiims @ASCO @ONCOassist @OpenMedicineHQ @MedwatchKate @scserendipity1 @CParkMD @urotoday @OncLive @crisbergerot @urologysummit @SuyogCancer @Larvol @IMG_Oncologists @piet_ost @DrSpratticus @GGiannarini @declangmurphy @NehaVapiwala @Prof_Nick_James @AttardLab @Silke_Gillessen @APCCC_Lugano
1
21
42
6,886
Tony Felefly retweeted
May 31
#ASCO26
Talk about real-time updates. NEJM paper now online and my predictions and inferences appear true.
Majority of MFS events were by PET not conventional imaging. "Most distant metastases were identified by PSMA PET (53.0% of those in the apalutamide group and 60.7% in the placebo group)"
VERY IMPORTANTLY: "No significant between-group difference was observed in metastasis-free survival assessed with conventional imaging alone (hazard ratio, 0.84; 95% CI, 0.67 to 1.07)"
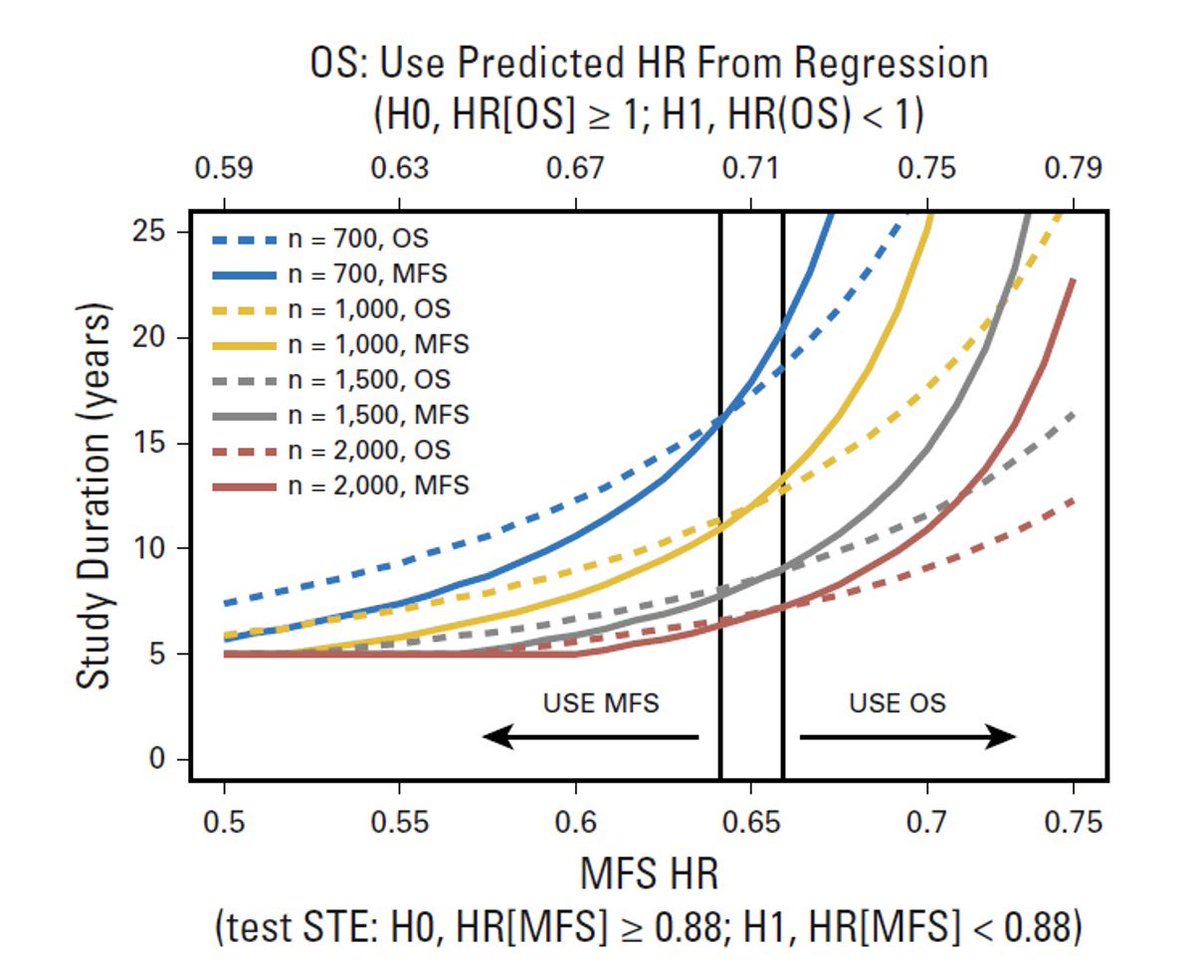
Not only does MFS cross 1, but the HR also crosses the surrogate threshold effect (0.81).
@urotoday @PCF_select @US_FDA
May 31

#ASCO26
The PROTEUS trial results are now online...buckle up as we wait to see the full presentation. This is going to be a trial that is likely highly controversial until the full results are published.
Some may call this a homerun, others may call this the largest negative trial @ASCO 2026. Up to you to interpret!
@urotoday @EricTopol @DrChoueiri @neerajaiims @ASCO @US_FDA @NCCN @myESMO @ASTRO_org @PCF_Science @declangmurphy @mcuban
3
30
74
12,424