
Lecturer @UniversidadMH 👨🏫 PhD in Sport & Health🔬📊 MSc in High performance and Health Sport 🏊♀️🏃♂️ Interested in #HRV ❤️ #cycling 🚴♂️ and #training
Joined June 2012
- Tweets 6,770
- Following 810
- Followers 1,079
- Likes 18,272
313 Photos and videos








Pinned Tweet

25 Nov 2025
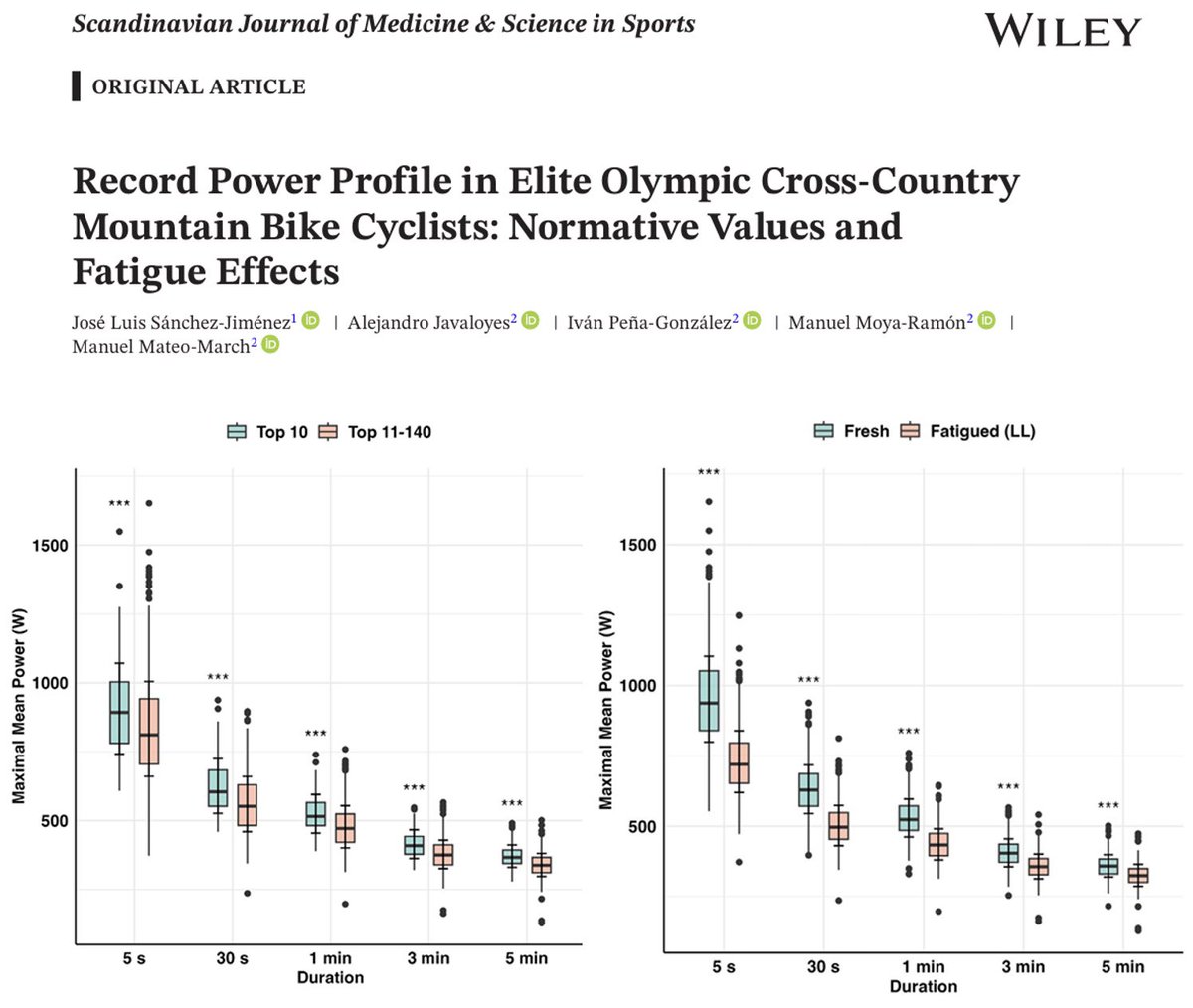
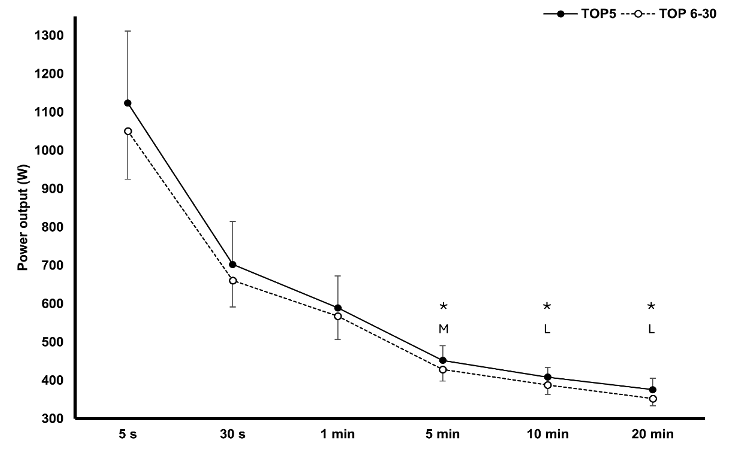
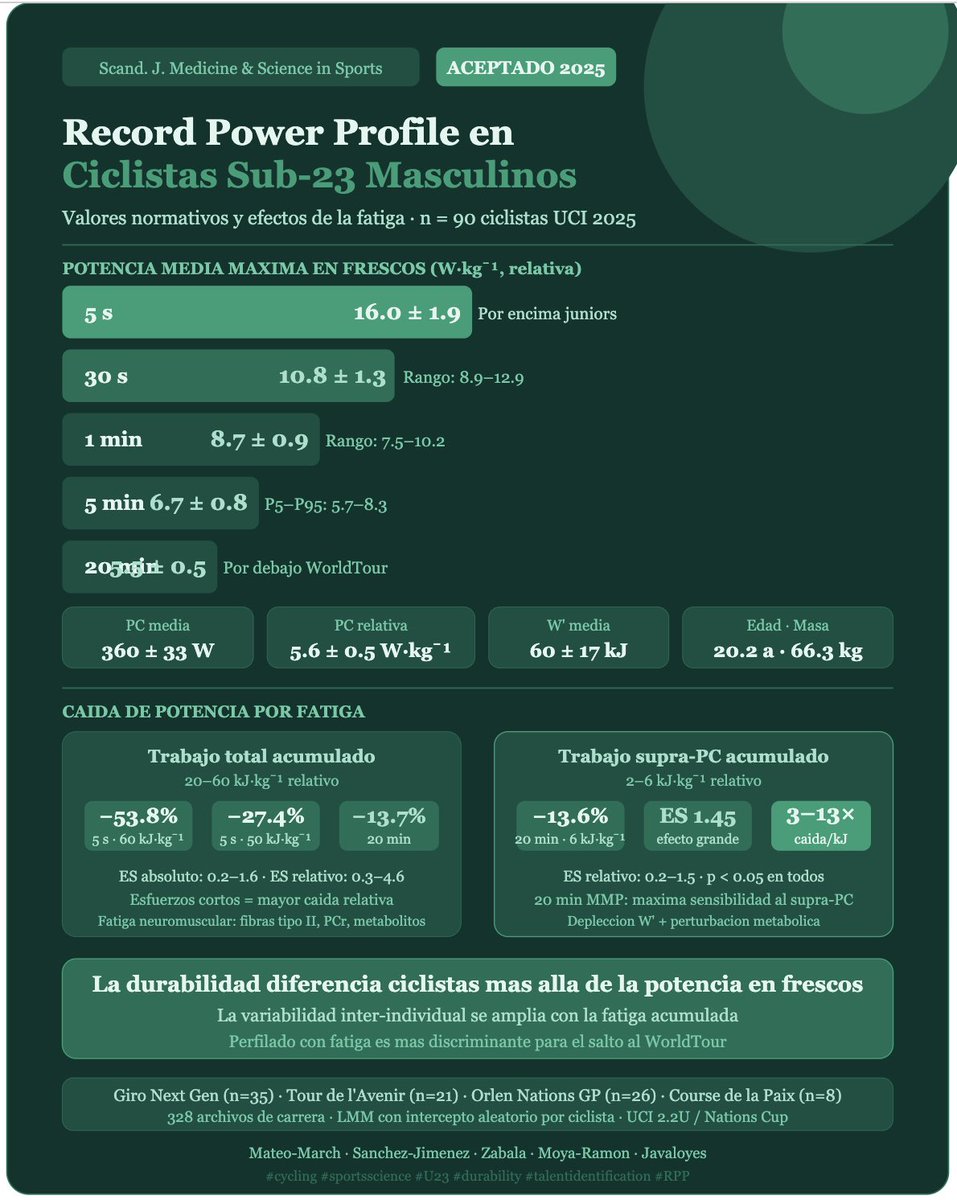
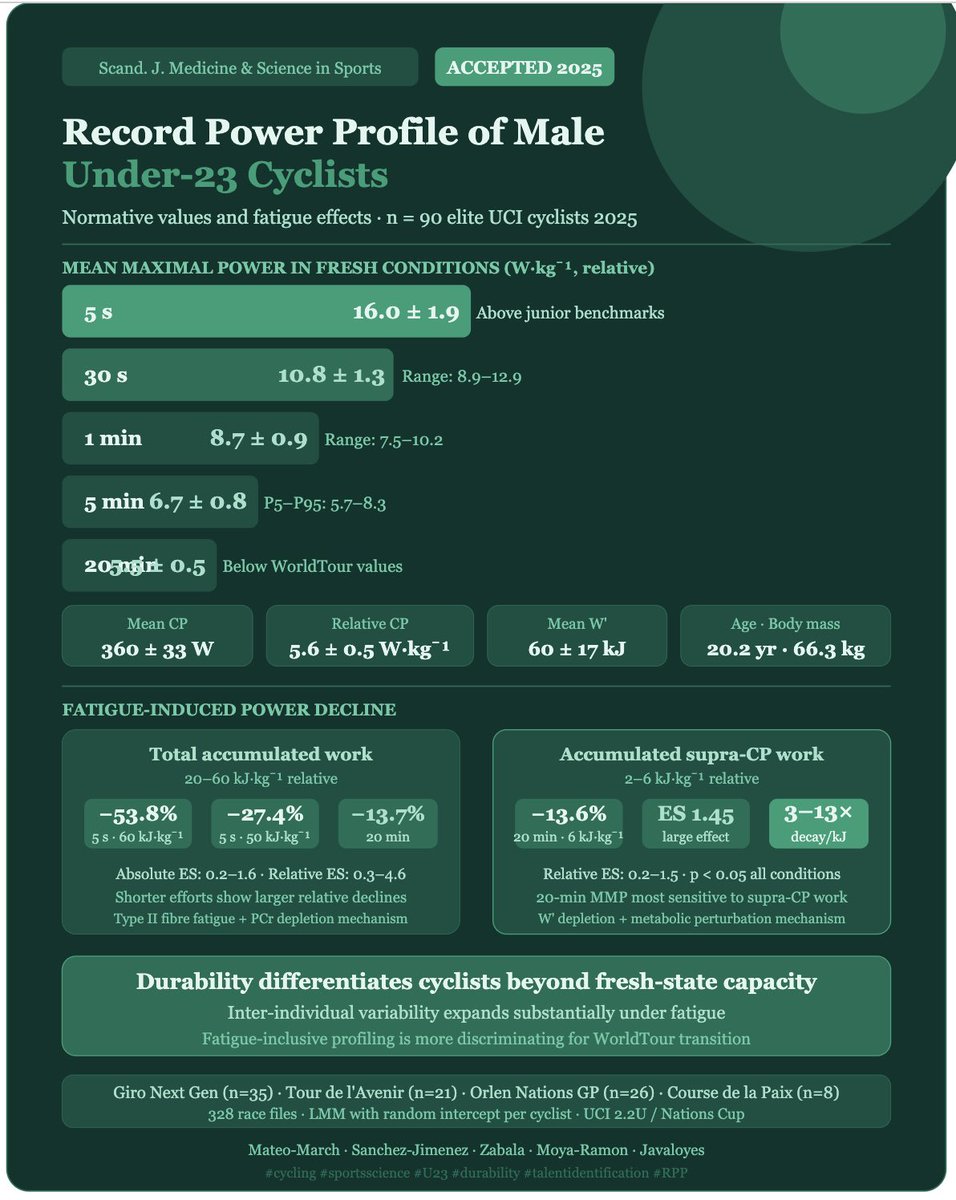
Elite XCO cyclists exhibit distinct power profiles, with notable declines due to fatigue, particularly in short efforts (<1 min)
Our last paper just got published in Scandinavian Journal Of Medicine & Science in Sports:
onlinelibrary.wiley.com/doi/…
7
34
2,562
Alejandro Javaloyes retweeted

1/10🧵
Is Durability related to Aerobic Fitness?
In other words, having higher VO2max and exercise thresholds necessarily means having a superior Durability?
Short answer: no
Long answer:👇
5
8
61
13,744
Alejandro Javaloyes retweeted

Apr 27
About Seixas being dropped by Pogačar in Liege-Bastogne-Liege 💪
“Task Failure in Endurance Sports: A Review”
link.springer.com/article/10…
· Juan‑José Pérez‑Díaz @erdecazalla
· José‑Antonio Salas‑Montoro
· James Hopker @JamesHopker
· Mikel Zabala
7
32
2,925

Alejandro Javaloyes retweeted

Feb 28
Your phone camera can measure HRV. Your Polar H10 can show real-time ECG with arrhythmia detection.
That's DeepHRV — and it's just getting started.
Sign up for release updates (no spam, ever): deepmetric.fit/newsletter
2
1
20
2,149
Alejandro Javaloyes retweeted

Feb 17
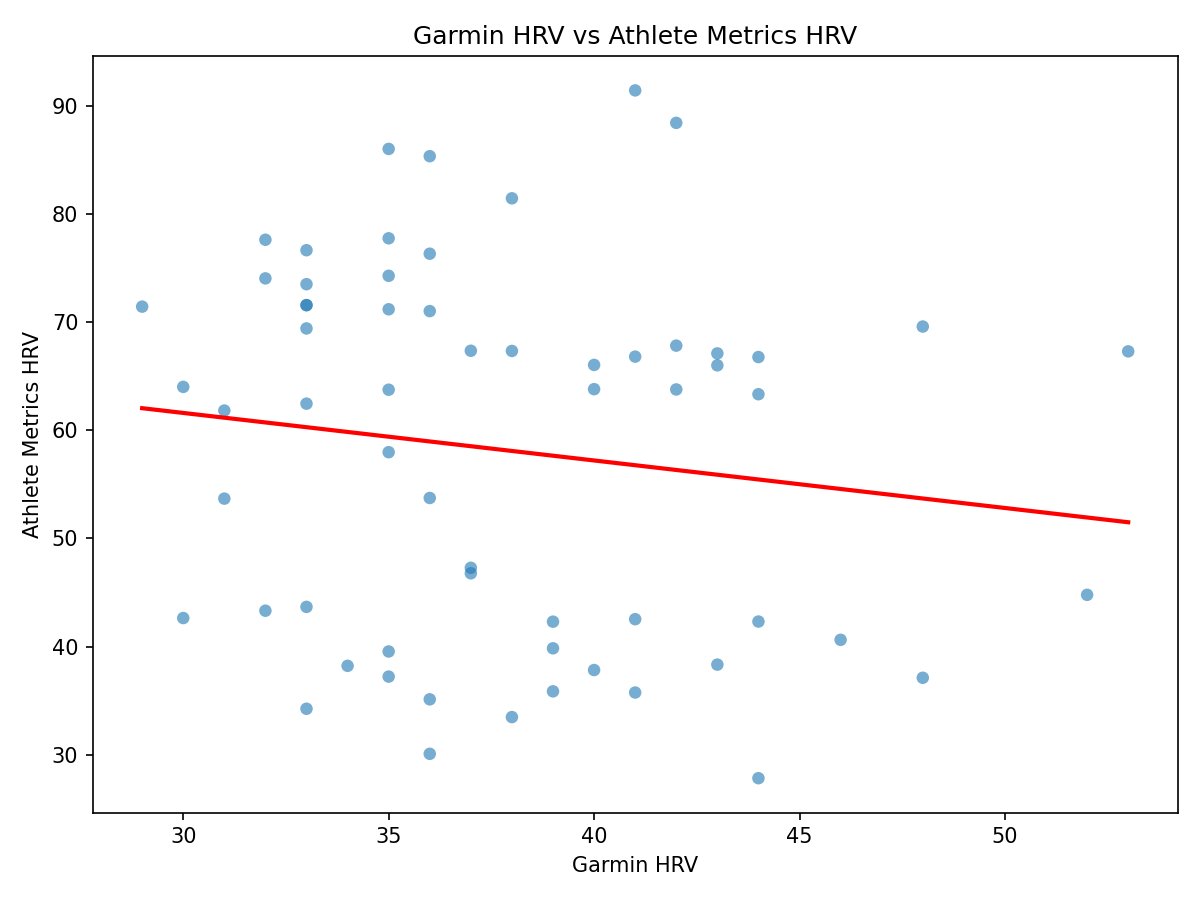
Just pulled my last 90 days of HRV data from my Garmin (wrist) data vs my 2 min morning HRV test with a heart rate strap.
Not even directionally accurate...
r = -0.13 !
Stop being lazy. Wear the damn strap.
Feb 17

Anyone who has tried to use wrist heart rate on a run knows that it's basically a random number generator.
This makes it completely worthless for #HRV, because even a few erroneous beats can have a HUGE effect on the HRV calculation.
Manufacturers know this, so they apply HEAVY filters to their algorithms that can push things in the opposite direction - removing true variability...
This means wrist HRV can read way above or way below true HRV in unpredictable ways!
Bottom line: If you care about HRV accuracy (you should!), the only acceptable method is a morning test with a heart rate strap.
20
10
181
40,823
🔝🔝🔝

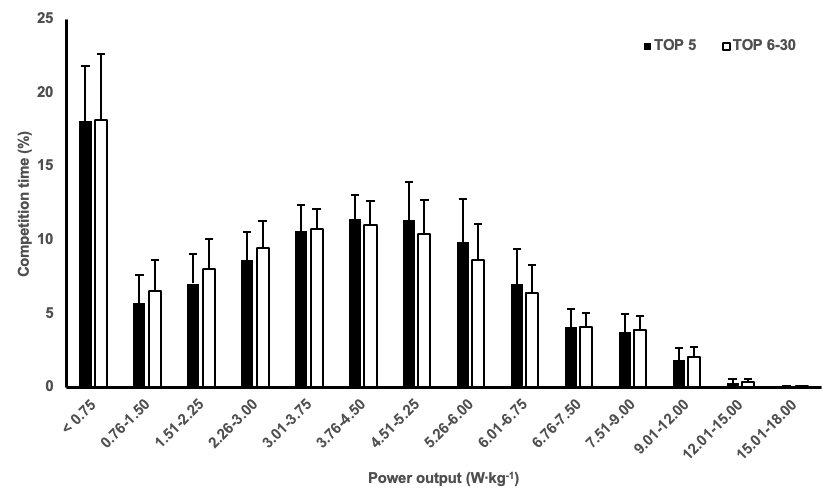
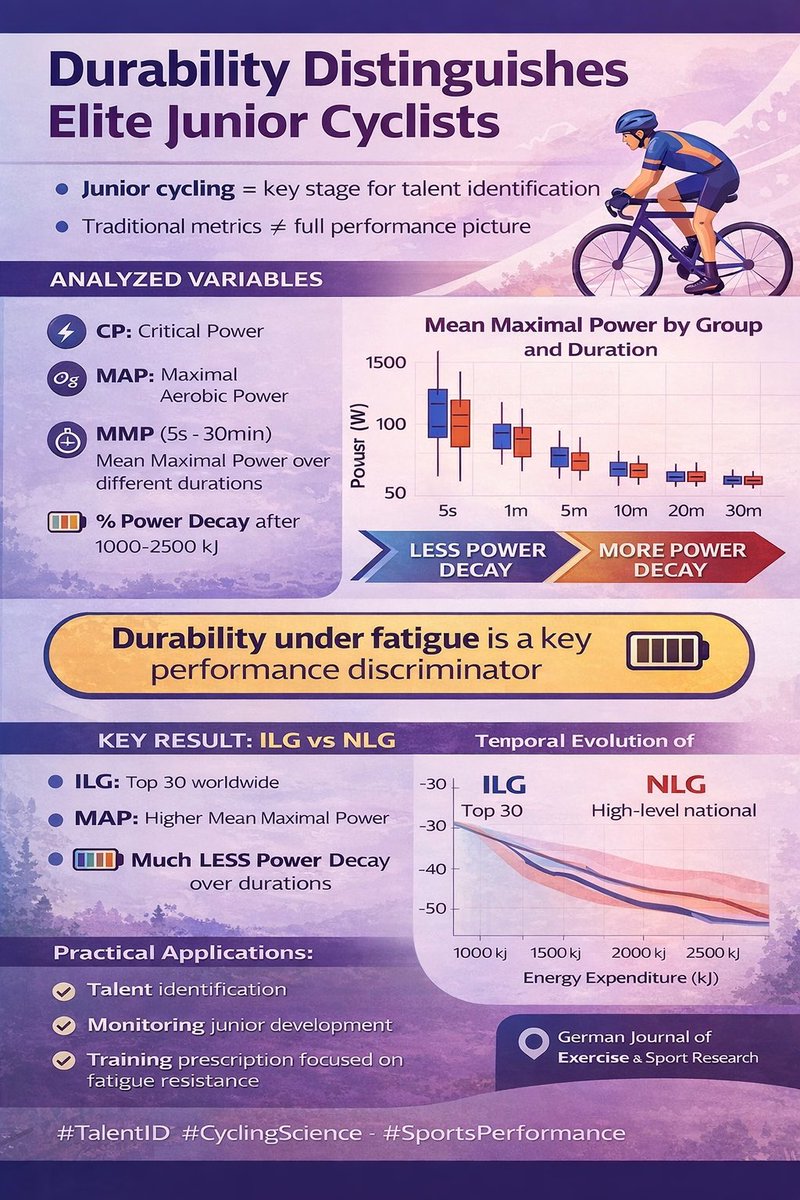
What separates elite junior cyclists from the rest?
Our new research reveals that international-level riders sustain power far better under fatigue — a decisive factor for future success.
Normative benchmarks included to support talent identification and coaching decisions.

1
404
Alejandro Javaloyes retweeted
What separates elite junior cyclists from the rest?
Our new research reveals that international-level riders sustain power far better under fatigue — a decisive factor for future success.
Normative benchmarks included to support talent identification and coaching decisions.
1
5
24
2,411
Alejandro Javaloyes retweeted
APPLIED SCIENCES SPECIAL ISSUE.
Innovative Wearable Sensors for Health Performance Evaluation mdpi.com/si/271711 #mdpiapplsci a través de @Applsci
2
8
554
Alejandro Javaloyes retweeted

🚀 New editorial published in the EJHM — “Acronym inflation in sport science: are we naming progress or renaming it?”
I reflect on the accelerating rise of acronyms in our field and question whether they signal real innovation or simply rebranding.
👉🏻 eurjhm.com/index.php/eurjhm/…


1
11
855
Alejandro Javaloyes retweeted
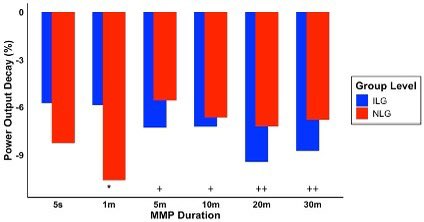
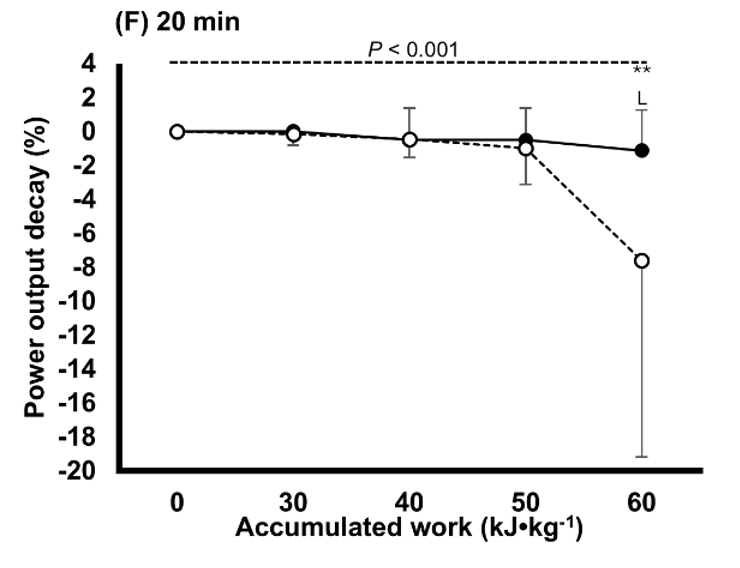
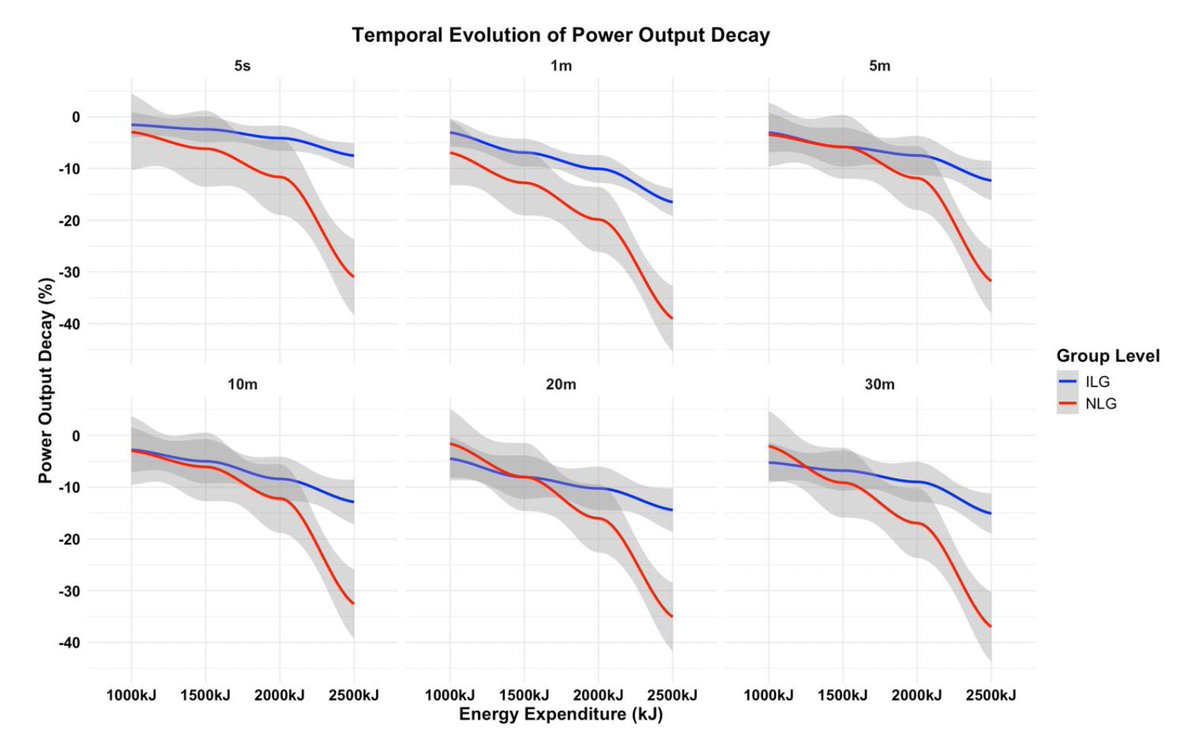
International-level junior cyclists demonstrate superior durability, with lower power decay than national-level peers, providing normative data from an exceptionally high-level sample in the current focus category.
5
28
1,695
Alejandro Javaloyes retweeted
🎉 New paper accepted!
🔍 International-level junior cyclists show superior durability (lower power decay) compared to national-level peers. German Journal of Exercise and Sport Research
📊Field-based data | Real competition demands
#SportsScience #CyclingPerformance #Durability
13
39
3,359
Alejandro Javaloyes retweeted
Jan 23
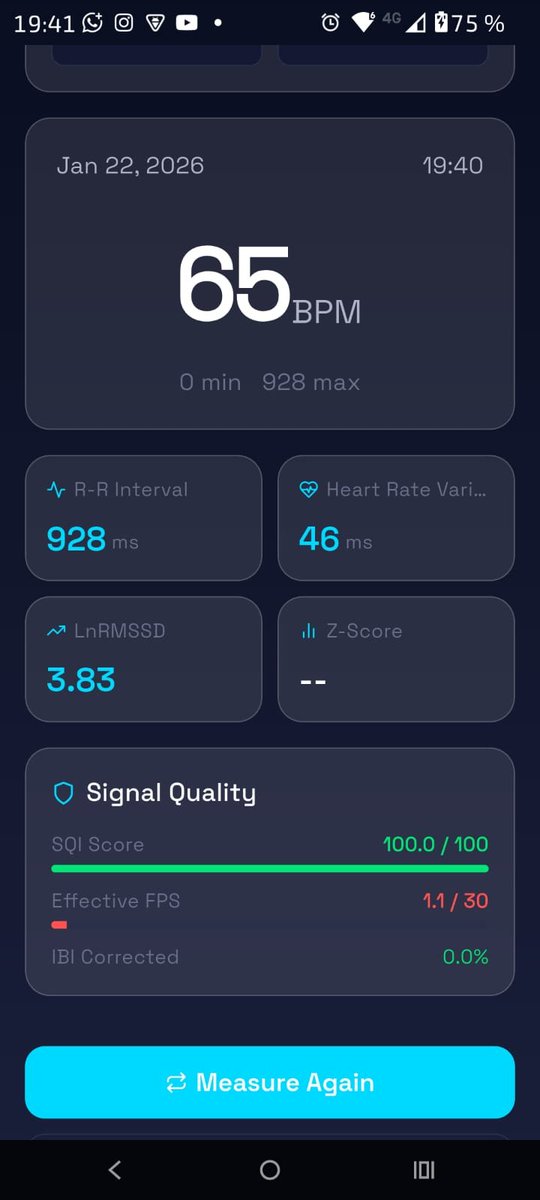
Development update on my HRV mobile app.
Comparison between PPG-based HRV (smartphone camera) and ECG using Polar H10.

2
1
6
885
Alejandro Javaloyes retweeted

Jan 20
Algo muy difícil de digerir y cruel después de todo lo invertido en la pretemporada para llegar a punto al principio de año a tan solo 3 días de arrancar.
Desde aquí hago un llamamiento si algún equipo está interesado. Actitud y ganas no me faltan. Gracias. 🫂

Comunicado oficial
Illes Balears Arabay no iniciará la temporada 2026 como equipo UCI Continental.
Una decisión responsable ante circunstancias ajenas al equipo, pese a tener el proyecto deportivo y empresarial completamente preparado.
🔗arabay.team/illes-balears-ar…
8
88
252
48,856
Alejandro Javaloyes retweeted
Jan 16
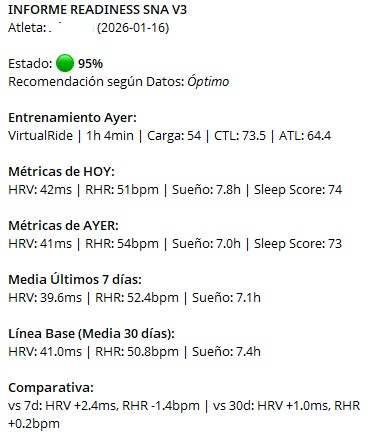
We built an automation that connects to @intervalsicu via API and sends a daily HRV-based readiness report to the coach on Telegram.
It helps spot abnormal values early and act fast.
Want to implement this alert system? DM me.

1
9
775

Alejandro Javaloyes retweeted
INSCRIPCIÓN ABIERTA: universite.umh.es/formate/in… Curso de Formación en Data Science Aplicada al Ciclismo.

4
12
1,266
Alejandro Javaloyes retweeted
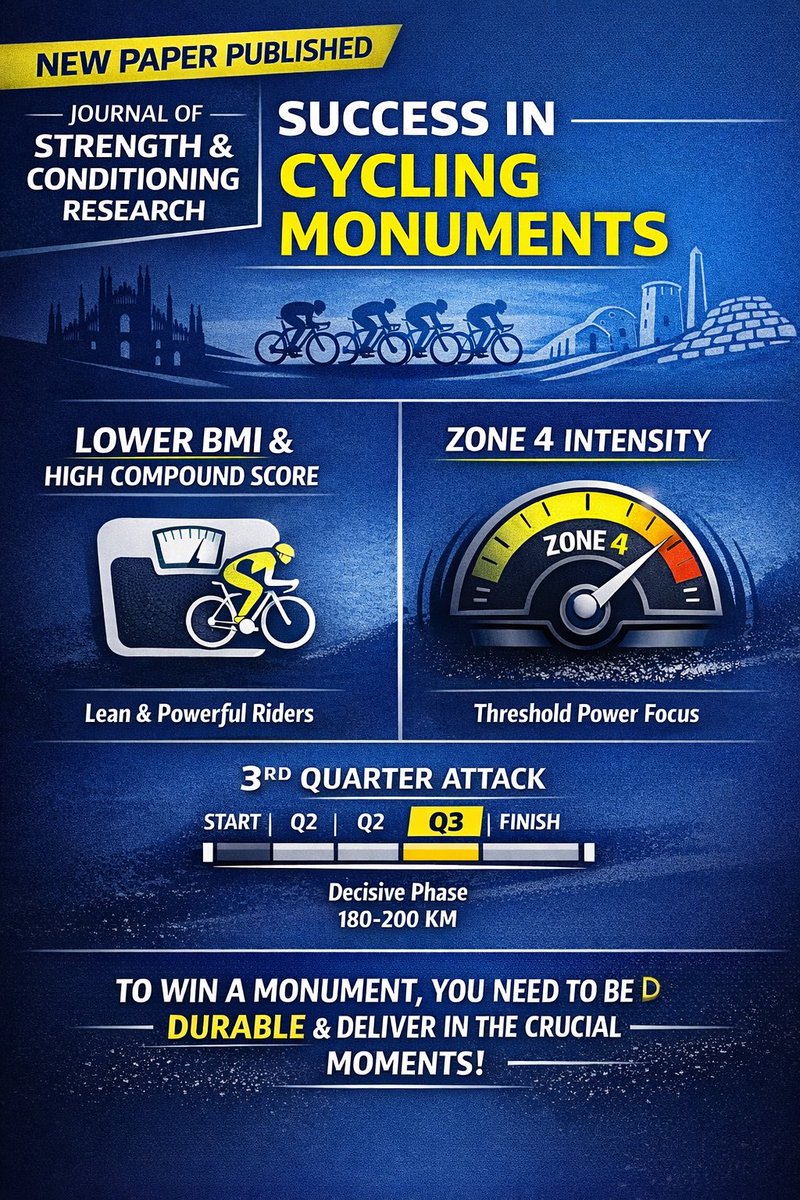
NEW PAPER 📝 PUBLISHED! Pacing Strategy and Workload Distribution as Determinants... : The Journal of Strength & Conditioning Research journals.lww.com/nsca-jscr/a…
1
4
23
1,388
Alejandro Javaloyes retweeted

3 Dec 2025
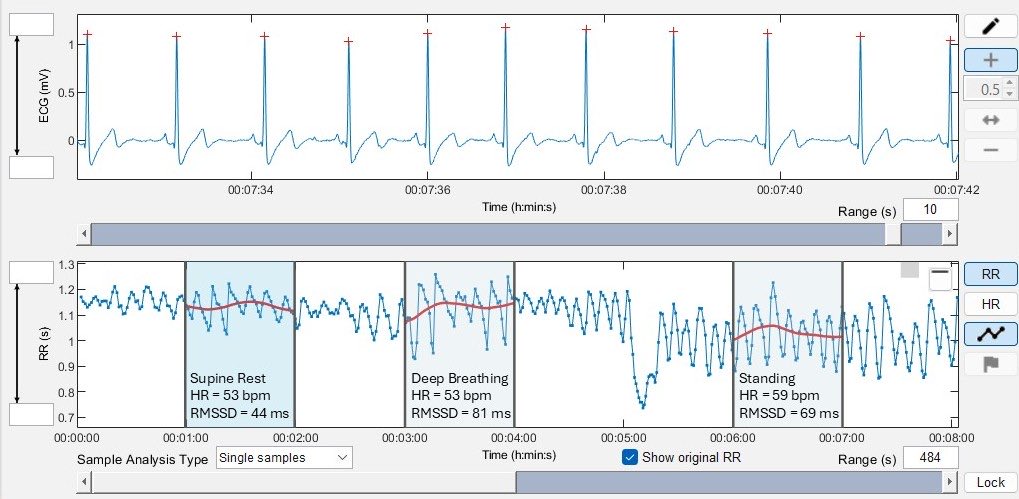
Here's an example of "parasympathetic saturation", highlighting an important limitation of supine (or sleeping) HRV.
When HR is <55 bpm, HRV often decreases, despite high parasympathetic activity. Thus, HRV becomes an invalid marker of parasympathetic control.
In the example below, RMSSD is 25 ms higher in the standing position despite a higher HR and the well-established vagal withdrawal induced by orthostatic stress.
This explains many (not all) cases of low HR with low HRV among fit individuals.
To overcome this issue, and due to its superior sensitivity to stress/fatigue, HRV is best measured after waking in the standing position, IMO.
10
19
141
11,894