
MBC advocate, microbiologist, educator, nature lover, gardener, reader, and feminist. She/her/hers.
Joined May 2014
- Tweets 2,465
- Following 504
- Followers 621
- Likes 17,053
108 Photos and videos










19 Dec 2025
Recovering from #SABCS25 (and working on a report back) and want to say thank you to all the researchers who presented and/or had any part in presented work. It's truly amazing the dedication and hard work by so many people. Appreciate you all!
1
13
1,347
13 Dec 2025
If I remember correctly this happened last year as well….disappointing doesn’t quite cover it.
2
360
Amy Beumer, Ph.D. retweeted

11 Dec 2025
Patient advocate Samantha Horn opens with a powerful question: “what were you doing in your 20s?” For her, it was chemo.
ICYMI, this is a must-watch educational session on breast cancer in young women.
#sabcs25 #oncoalert

5
12
562
11 Dec 2025
Disappointed in the mass exodus as the patient advocate is coming in to discuss the patient perspective on mTNBC. #SABCS25
1
1
5
240
11 Dec 2025
Looking forward to this- join me!!
11 Dec 2025

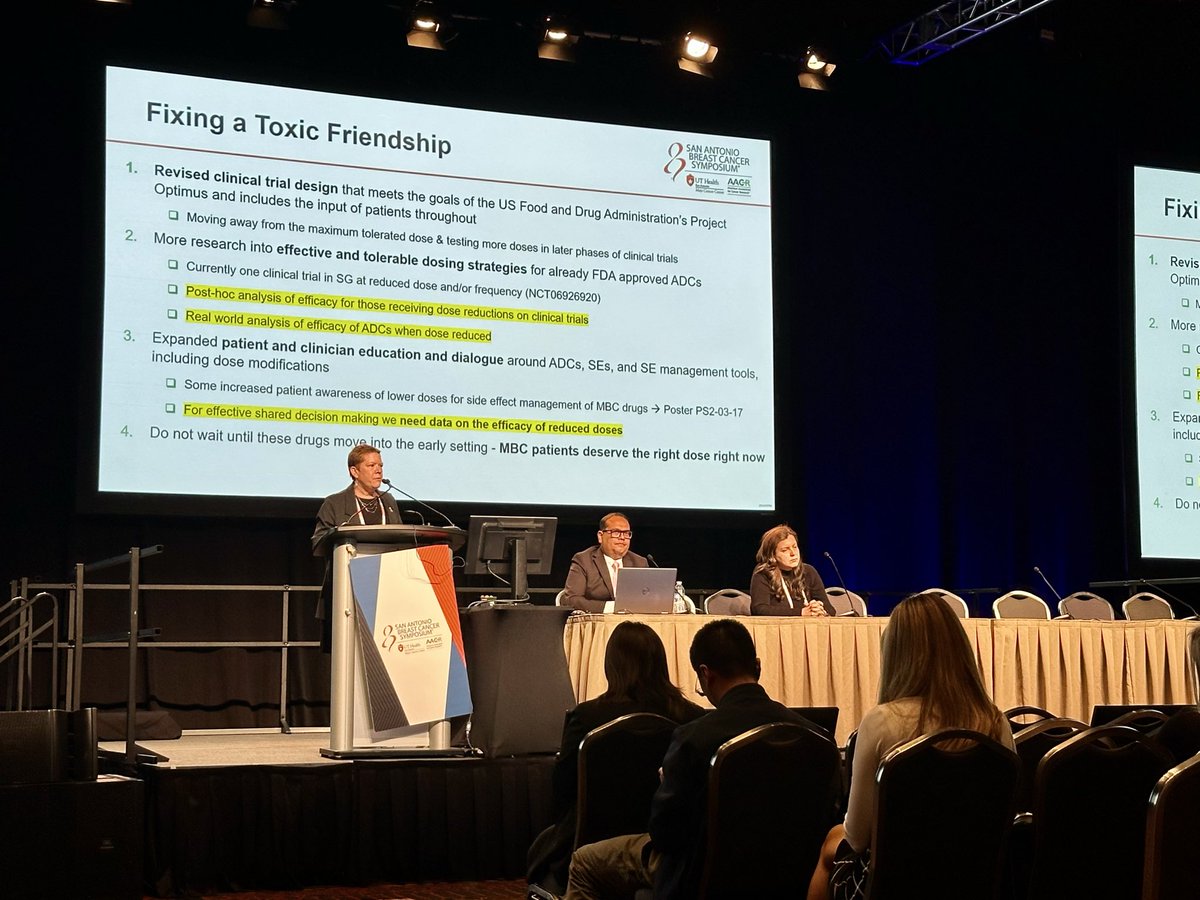
Quality of life matters! Join Poster author @amybeumer of the Patient-Centered Dosing Initiative (PCDI @TheRightDose) at poster walkthroughs next week to discuss findings from a large MBC patient survey that highlight the need for more individualized dosing strategies.
1
2
468
Amy Beumer, Ph.D. retweeted

11 Dec 2025
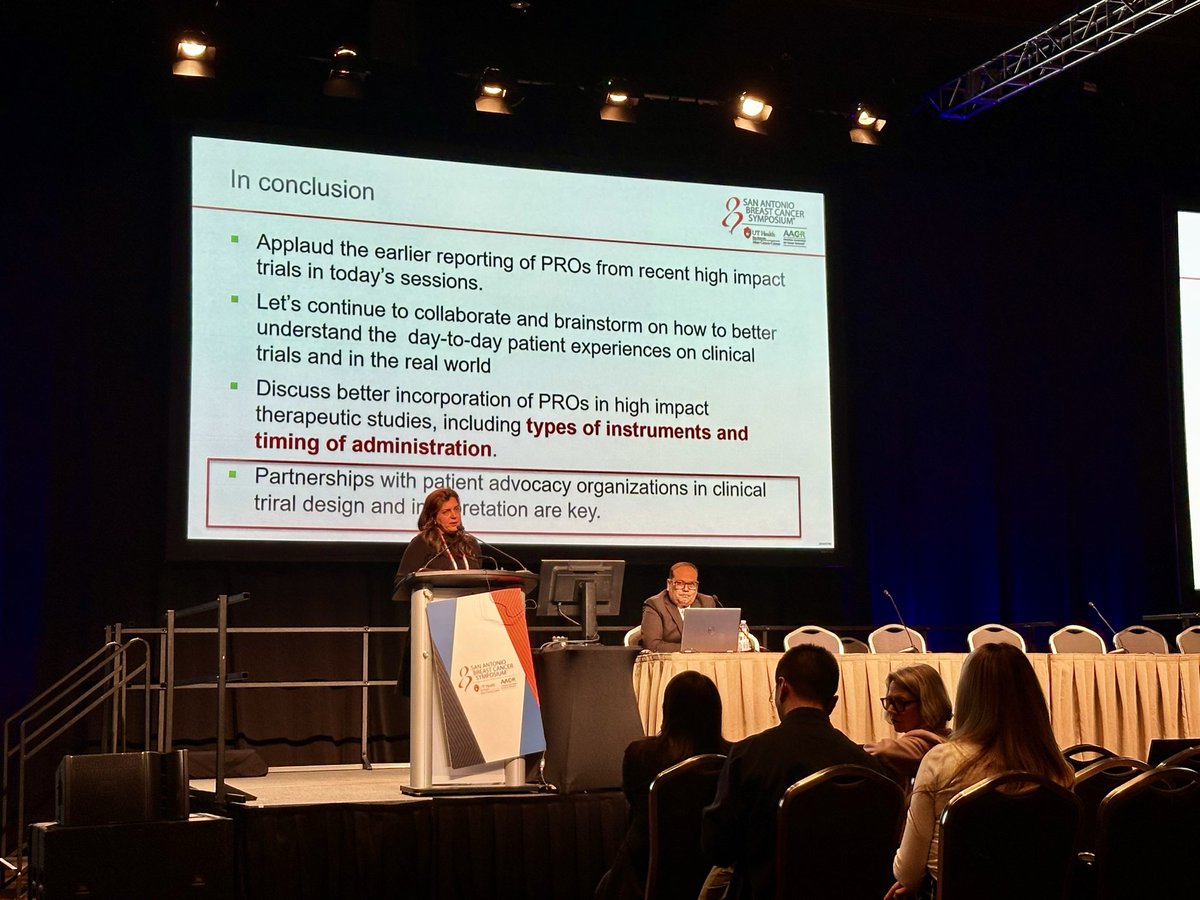
📢 Amazing talks by @amybeumer & @maryam_lustberg on PROs in cancer trials
🤝partnership w/ patient advocates in design
🔹consider type & timing of PRO
🔹research needed in effective & tolerable dosing strategies
🔹real world data provides key insight
@GRASPtweets @the_rightdose
6
8
729
Amy Beumer, Ph.D. retweeted

9 Dec 2025
Grateful to @christeeny513 for sharing her story - and how her concerns of a lump were initially dismissed with something far too many hear: “you’re too young for breast cancer”. No one is too young and everyone deserves to have their concerns addressed. #SABCS25 #bcsm

7
20
830
Amy Beumer, Ph.D. retweeted
9 Dec 2025
This exactly what we need - guidance to mitigate the side effects from our treatments. Many of us start antihistamines a few days before beginning capi and never have to deal with the rash. And for those super sensitive to loperamide 🙋♀️off label crofelemer can be a game changer.
8 Dec 2025

As we kick off #SABCS25, excited to share our new recommendations paper for capivasertib in HR MBC: 10 practical recommendations to optimize treatment and patient experience.
nature.com/articles/s41523-0…
@HeatherMoore16 @ErikaHamilton9 @jhaveri_komal @hoperugo @WinshipAtEmory
1
3
6
820
5 Dec 2025
I’ll be there and hope to see you there too!
4 Dec 2025

Attending #SABCS25? Join the @GRASPtweets
reception, one of the few opportunities for scientists, clinicians & patient advocates to connect.
It's where so many collaborations are born to bring the patient experience to research!
Register here: graspcancer.org/event/sabcs2…
1
3
183
Amy Beumer, Ph.D. retweeted

13 Nov 2025
This is going viral!!
Join us tomorrow at 1:30 PM EST.
Free to watch but registration required at link below.
31 Oct 2025

What are the most important takeaways from #ESMO25 for #BreastCancer care? Join @DanaFarber experts on Nov 14th for our live #BreastCancerBreakthroughs webinar discussing the latest clinical advances, research highlights, and their impact on patient care.
📅November 14, 1:30–2:30 PM EST
👉Register for free today: bit.ly/3WvQUhi
Moderator: @DrHBurstein Panelists: @stolaney1 @nlinmd @FilipaLynce #AnaGarridoCastro

2
10
30
6,926
13 Nov 2025
Raising the bar is what I like to hear. Helpful algorithm too- thank you Dr. Sammons #bcsm
12 Nov 2025

I gave a talk this weekend at Curio Expert Meeting in Tampa, FL with the task of educating the community on updates in ER , HER2- MBC. It is getting to be quite the challenge!
Here are my thoughts on likely algorithms in 2026. The bar is getting higher on safety and efficacy.

1
1
4
213
Amy Beumer, Ph.D. retweeted

1 Nov 2025
Share your MBC side effects & experiences in this MBC patient-led survey from PCDI. Your MBC story can help PCDI work to improve treatment dosing, clinical trial design, and quality of life on long-term treatment. E-mail surveys @ therightdose . org to get a personal link (copy, paste & delete the extra spaces)
#metastaticbreastcancer
#bcsm
#research
#QoL

4
10
668
Amy Beumer, Ph.D. retweeted
31 Oct 2025
MBC doesn’t stop just because October ends. Neither does the need for research.
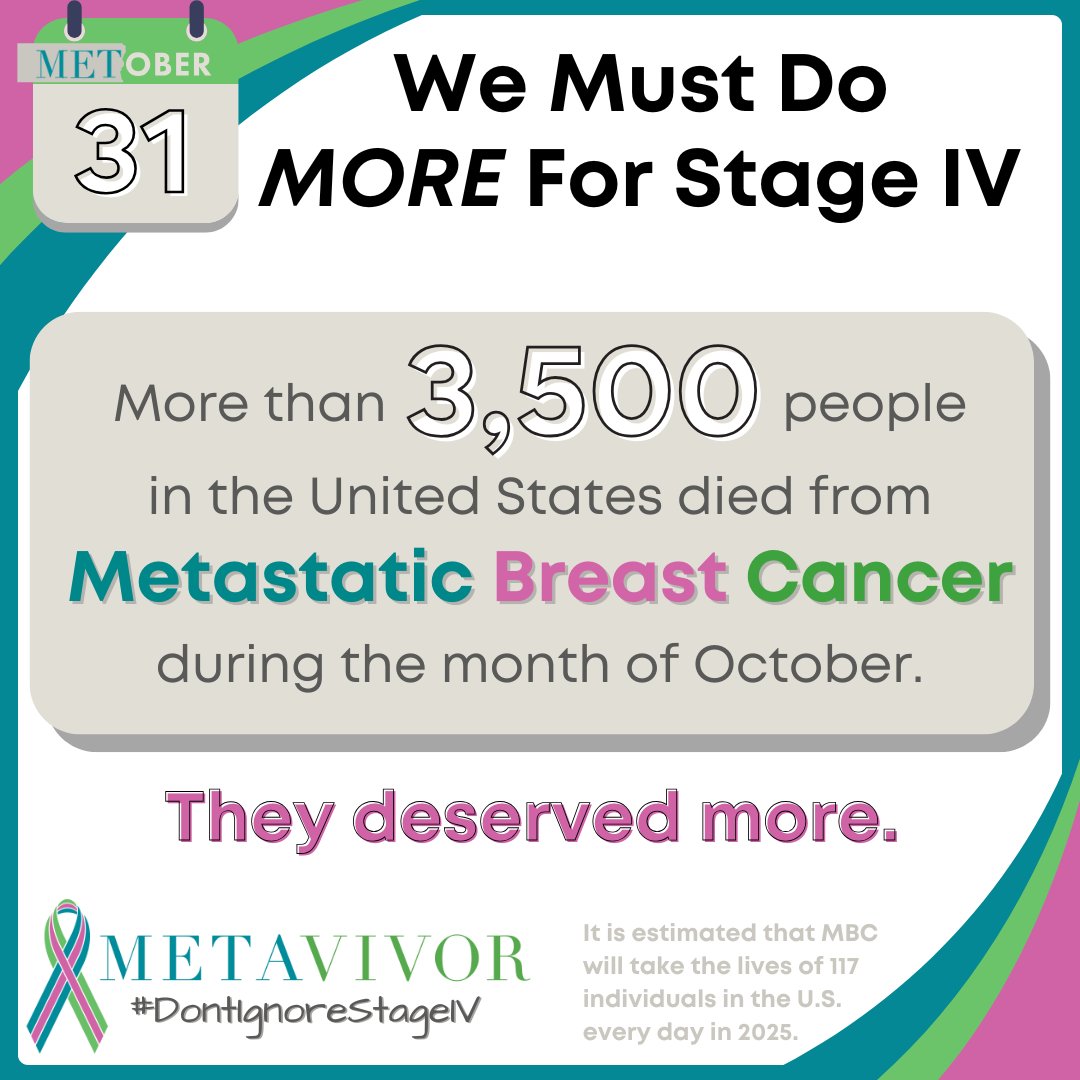
31 Oct 2025

As October ends and pink ribbons fade, we cannot forget Stage IV—not for a single day. Only 13% of breast cancer research funding goes to the disease that kills.
Thank you for following our #METober posts. Please keep sharing and spreading the word #UntilNoOneDiesFromMBC
10
22
1,829
Amy Beumer, Ph.D. retweeted

20 Oct 2025
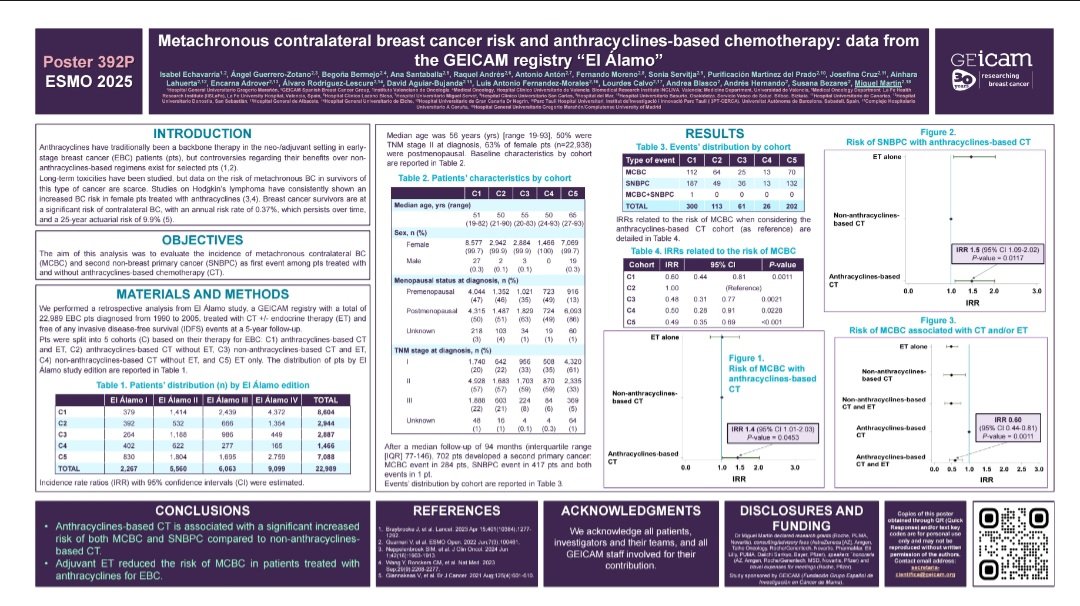
#ESMO25
🇪🇸 GEICAM “El Álamo” (n=22,989)
Anthracycline-based chemotherapy significantly increased the risk of contralateral breast cancer and second primary malignancies (IRR 1.46; p=0.039).
💬 Real-world data remind us once again: long-term toxicity cannot be ignored.
18 Oct 2025

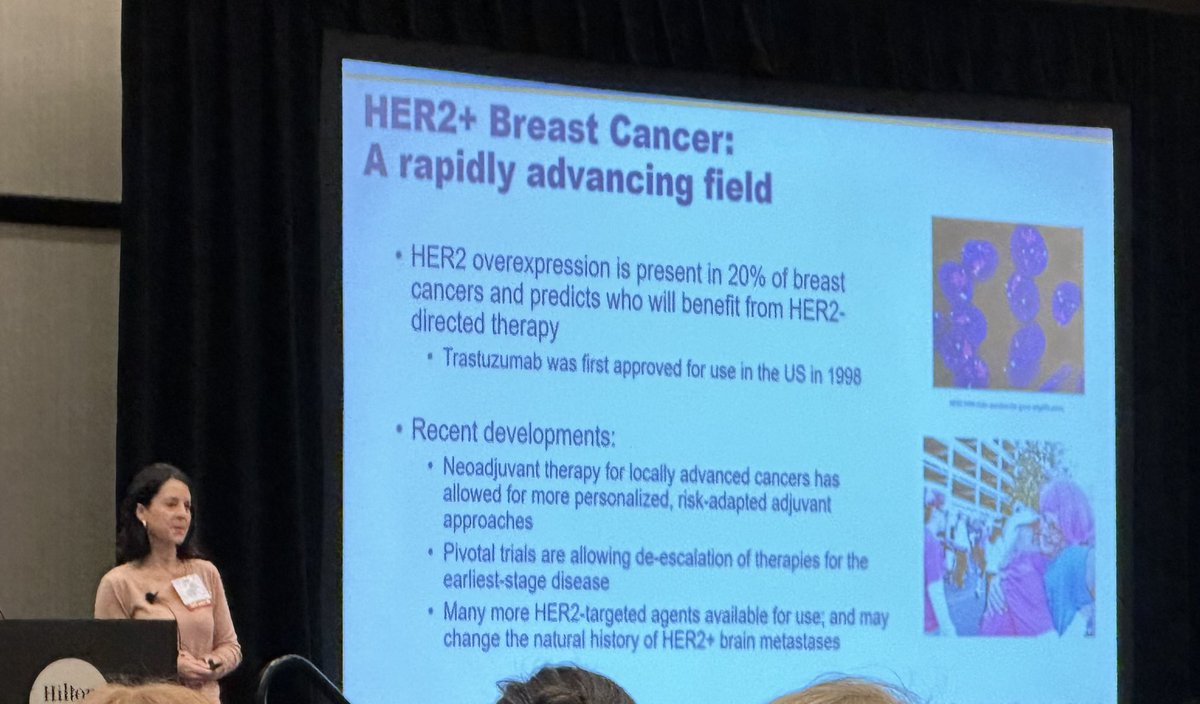
Ask any breast oncologist today, and they’ll tell you they prefer anthracycline-free regimens in HER2-positive breast cancer — and that anthracyclines don’t improve response rates.
So how did we accept a control arm containing anthracyclines in the DESTINY-Breast11 trial, which began in October 2021?
We can’t simply call this a sponsor-driven choice.
It’s the physicians who persuade patients to enroll — physicians who also receive payment for every screening and treatment visit.
Let’s be honest: how do you justify to your patients a control arm that doesn’t reflect your own real-world practice?
I’m open to any kind of criticism; just don’t come to me with the fairytale that anthracycline-containing arms are still the “standard.”
I know this sounds a bit harsh, but we’re exhausted from having to point out flaws in control arms every time new trial results are presented. We’re now seeing control arms that no longer represent today’s standards — some even belong to history (eg. ARANOTE trial).
It’s a call to all of us, as physicians, to think more carefully about the trials we support — if our genuine goal is the health and well-being of every patient, including those in the control arm.

2
12
25
5,448
22 Oct 2025
RT @stage4kelly: Grateful to all our elected representatives who understand the need for research funding and supporting bills that help th…
2
Amy Beumer, Ph.D. retweeted
21 Oct 2025
I’ve been in the liver met “club” for a year or so now, thankfully responding to the treatment targeted to mutations my cancer has. I’m alive and doing pretty darn well thanks to #research. Please support @metavivor #UntilNoOneDiesFromMBC
21 Oct 2025
About two-thirds of MBC patients have liver metastases at death, and 1 in 4 already have liver involvement at diagnosis.
Liver transplants aren’t an option for MBC patients—another reason why we need more research for better treatments.
#UntilNoOneDeisFromMBC #Research

4
15
927
Amy Beumer, Ph.D. retweeted

19 Oct 2025
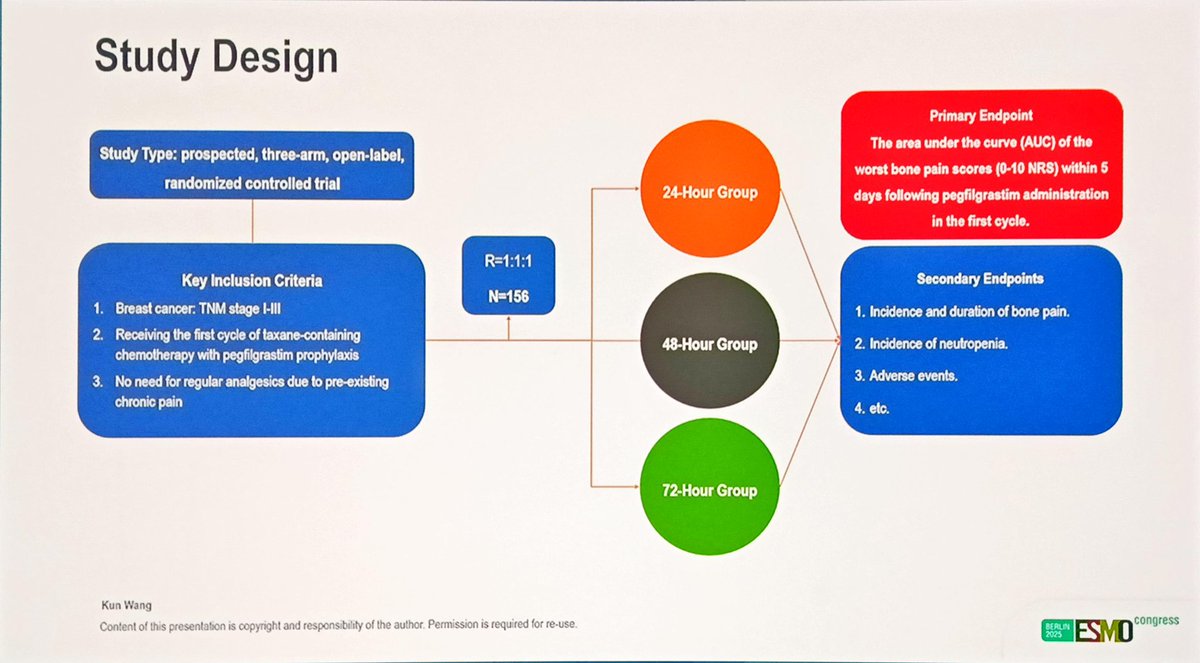
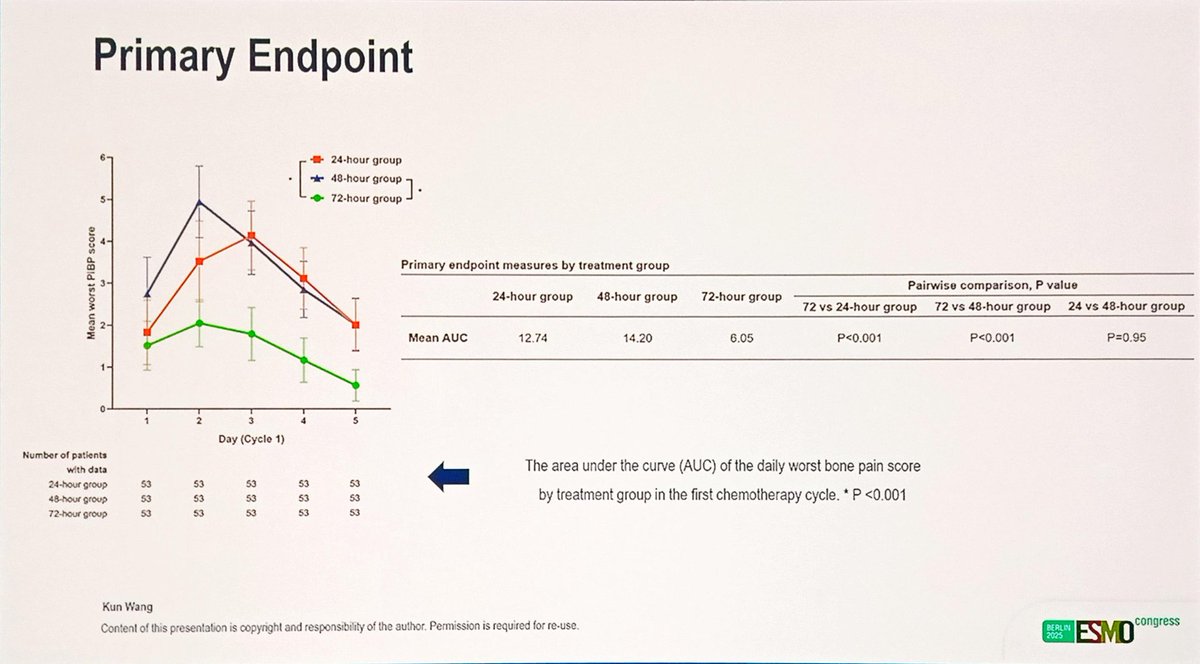
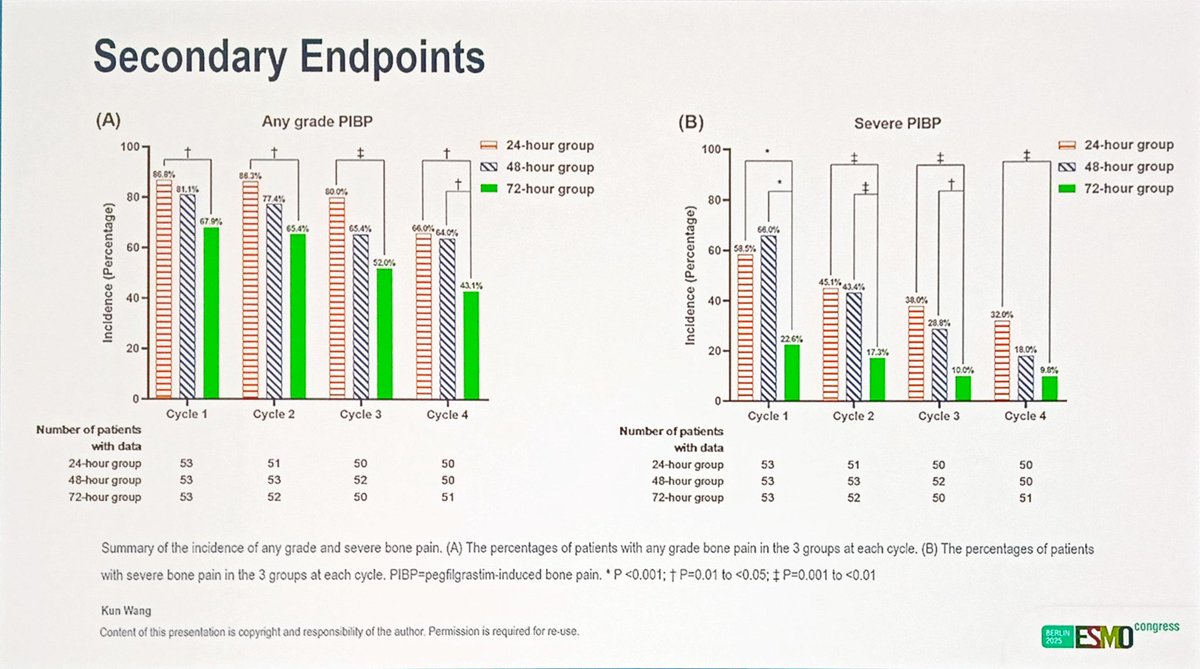
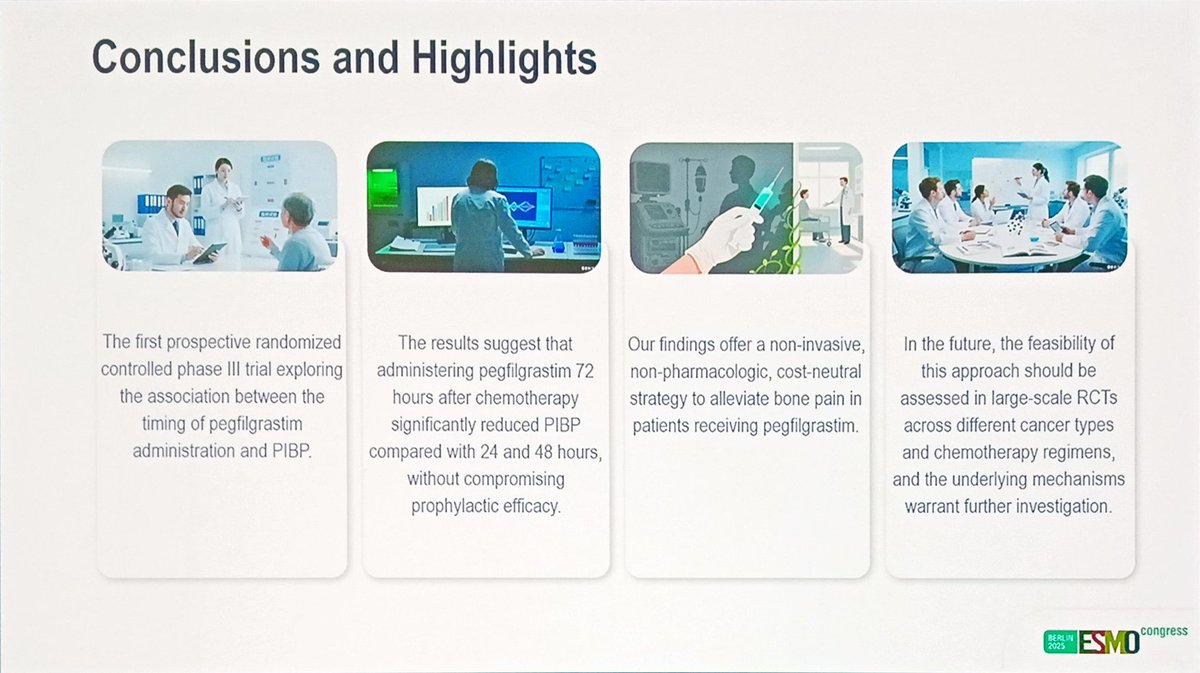
Interesting study on ⬇️ bone pains by delaying timing of peg-filgrastim after taxane
Though better is to omit routine peg-filgrastim, which is feasible in most pts getting dose dense paclitaxel … (we still use routine growth factor with docetaxel)
pmc.ncbi.nlm.nih.gov/article…
19 Oct 2025

RCT on timing of pegfilgrastrim after CT shows significantly reduced bone pain with 72-hour timing as compared to 24- and 48-hour timing
#ESMO25 @myESMO @OncoAlert
8
29
3,689
21 Oct 2025
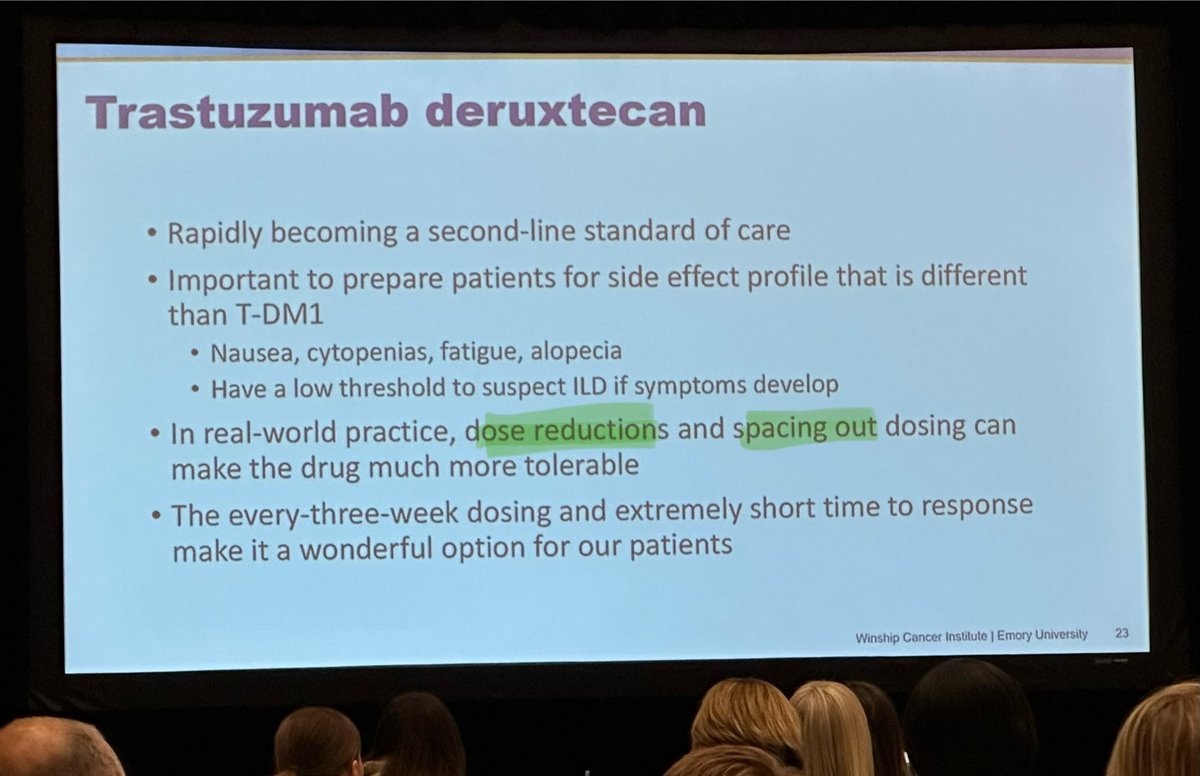
Let me fix this, "since ADCs have moved to standard of care it's been critical to be aware of how to mitigate their side effects". Yes, more people and different goals, but eBC v. aBC we all deserve QoL and fewer AEs. Love the focus but words matter. #bcsm #ESMO25
21 Oct 2025

Grateful for the chance to chair the #ESMO25 ADC educational session & present on ADC toxicities. With ADCs moving to the curable setting across cancers, it’s critical to be aware of how to mitigate their side effects. For an in-depth dive into the topic: nature.com/articles/s41571-0…

1
2
11
1,135
21 Oct 2025
Remember that M/aBC patients have been suffering AEs for years now with little push to examine reduced dosing for efficacy AE mitigation. Now is a good time but it shouldn't take treating eBC to put out the call. Our lives & QoL matter too. #bcsm #ESMO25 dailyreporter.esmo.org/esmo-…
2
2
9
287
20 Oct 2025
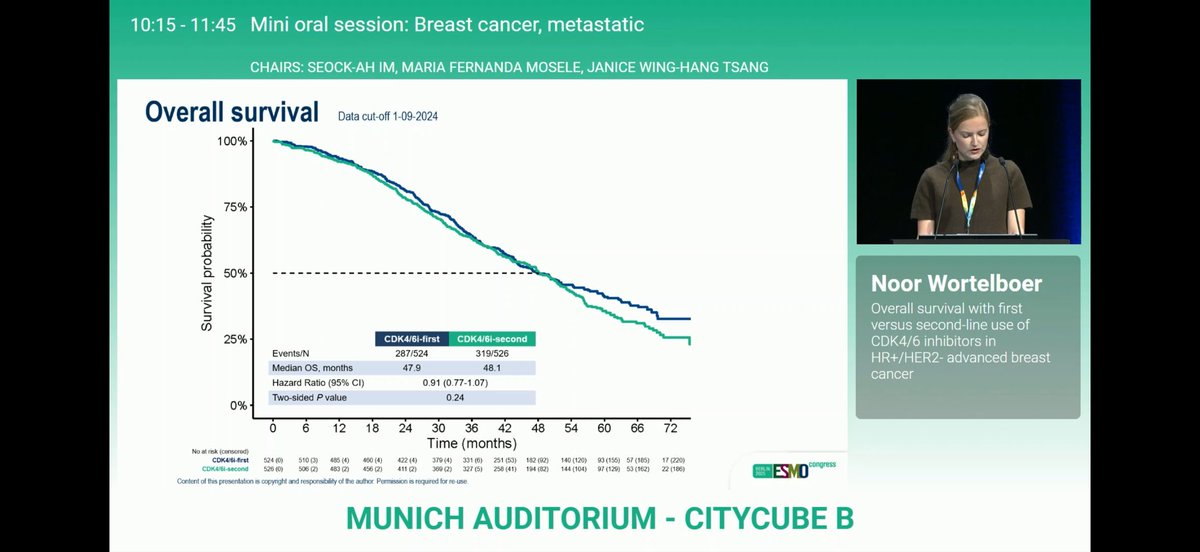
Can HR MBC forego CDK 4/6 inhibitors in the first line? More data from a necessary trial showing…maybe? Dr. Graff laying out the caveats from the ongoing study #bcsm
20 Oct 2025

SONIA overall survival analysis = no significant difference 1L vs 2L CDK4/6i, except premenopausal; draws same criticisms RE: low OS compared to historical trial, non-standard of care single agents & CDK4/6. Still impressive data adding value. #ESMO25 @OncoAlert


2
3
305