Cardiology Point-of-Care Ultrasound Solutions: Integrating Hardware, Software, Artificial Intelligence, Education, and Training: The EchoScope Project
Joined May 2011
- Tweets 1,137
- Following 1,024
- Followers 416
- Likes 2,536
99 Photos and videos

Pinned Tweet

16 Jan 2022
"For the heart to effectively pump, it must first effectively fill."
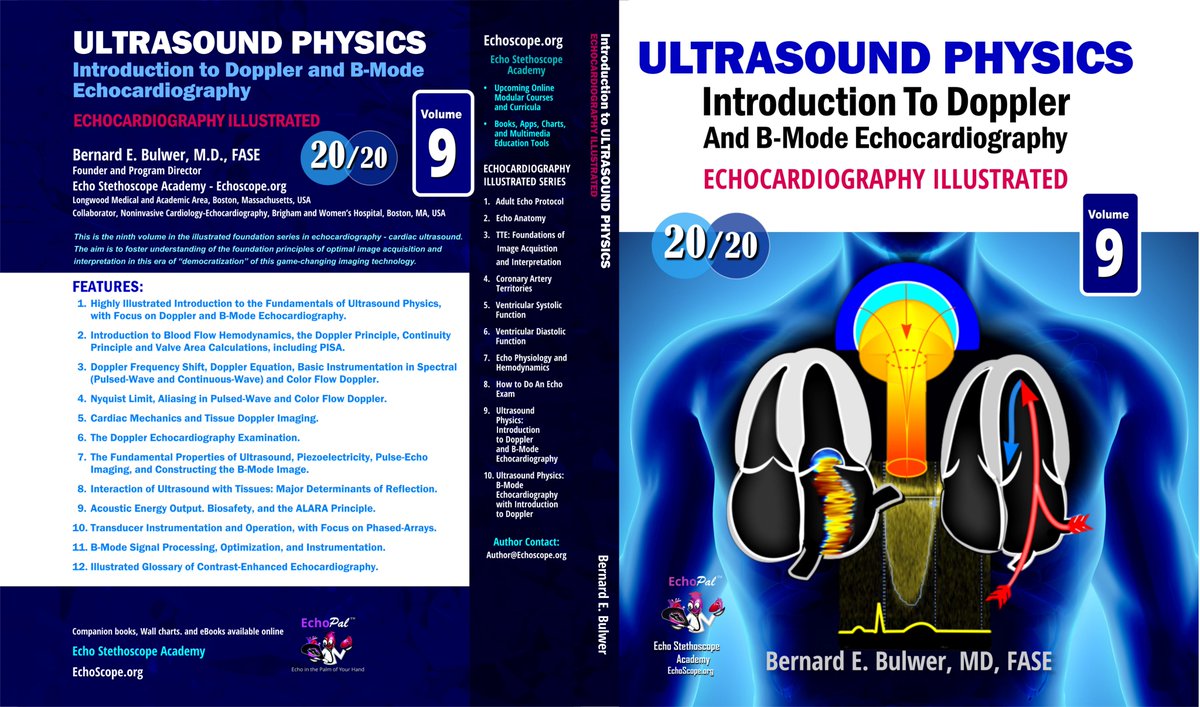
Ventricular Diastolic Function: FEATURES: 351 pages, > 2,000 Illustrations and Images. Publication date: Jan 16, 2022.
LOOK INSIDE: amazon.com/dp/B09QFJ4S4W?ref…
2
5
16
Bernard E Bulwer retweeted

Jun 11
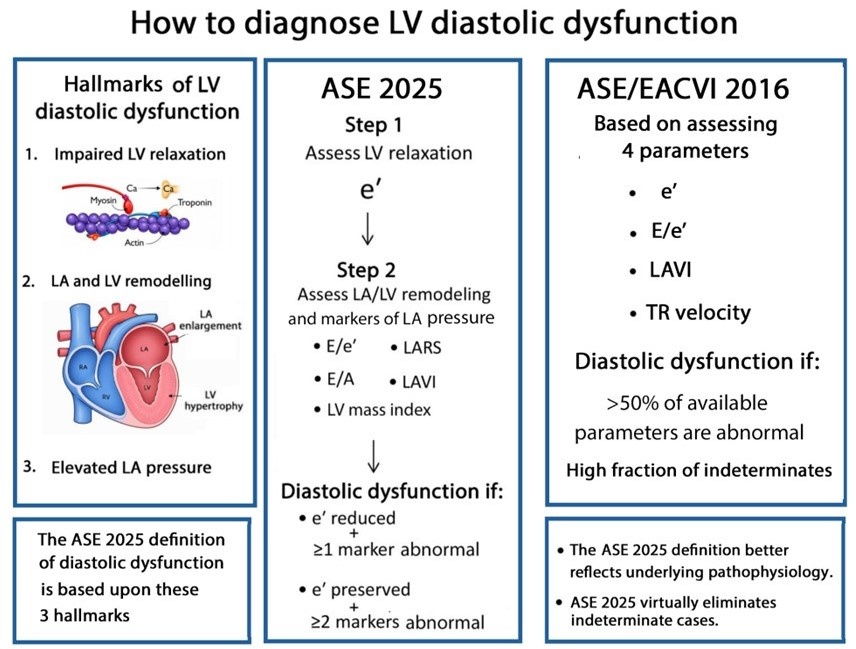
Most echocardiography laboratories have adopted the 2016 diastolic guidelines. With the release of the 2025 update, an important question arises:
What are the key conceptual differences between the 2016 and 2025 approaches to diagnosing diastolic dysfunction?
academic.oup.com/ehjcimaging…
@JGrapsa
12
83
254
17,155
Bernard E Bulwer retweeted

Our 6th Advanced Imaging Techniques: Virtual Experience will be held August 29-30! 🫀
Sign up: bit.ly/4mzI1za
Attendees will gain a systematic approach to the evaluation of MR and TR using 3D technology, providing the precision required for modern clinical practice.
13
47
3,539
Bernard E Bulwer retweeted
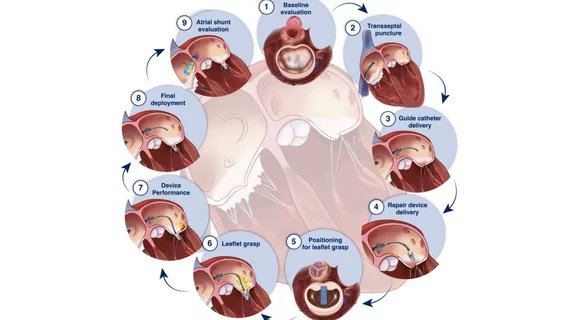
Check out this excellent @CardioBusiness article by @DaveFornell about our new #ASEGuideline, "Guidelines for the Intraprocedural Imaging for Mitral Valve Transcatheter Edge-to-Edge Repair (M-TEER)!"
Read it: bit.ly/4eeaVBn
6
26
2,277
Bernard E Bulwer retweeted
We've released a #new State-of-the-Art Review, "The Effect of General Anesthesia and Mechanical Ventilation on the Echocardiographic Evaluation of Cardiac Function!"
Read it now: bit.ly/4eokgaT
39
88
4,146
Bernard E Bulwer retweeted
🫀PRODUCT OF THE MONTH🫀
#AdvancedEcho 2026 online course is a comprehensive program designed to update cardiology and imaging professionals on the forefront of cardiovascular ultrasound.
Sign up: bit.ly/4tzfWKr

2
9
30
1,940
Bernard E Bulwer retweeted

Great point @NephroP 🌟
Yes - in acute PE the septal shift is often most pronounced in late systole and early diastole rather than uniformly throughout systole.
👉 adult and pediatric patients with acute PE #echofirst
👉 TG mid SAX
May 21

Since you’re clearly not a beginner, that part is too easy for you!
But I do have a question for advanced users like you who have likely seen a lot of acute PE cases.
When exactly does septal flattening occur in acute pulmonary embolism, assuming the patient does not have chronic pulmonary hypertension with RV hypertrophy? My understanding is that for septal flattening throughout systole, the RV pressure would need to exceed LV pressure, which seems less likely in an acute event. So wouldn’t the flattening be more prominent during late systole and early part of diastole instead?
2
12
56
12,566
Bernard E Bulwer retweeted

May 22
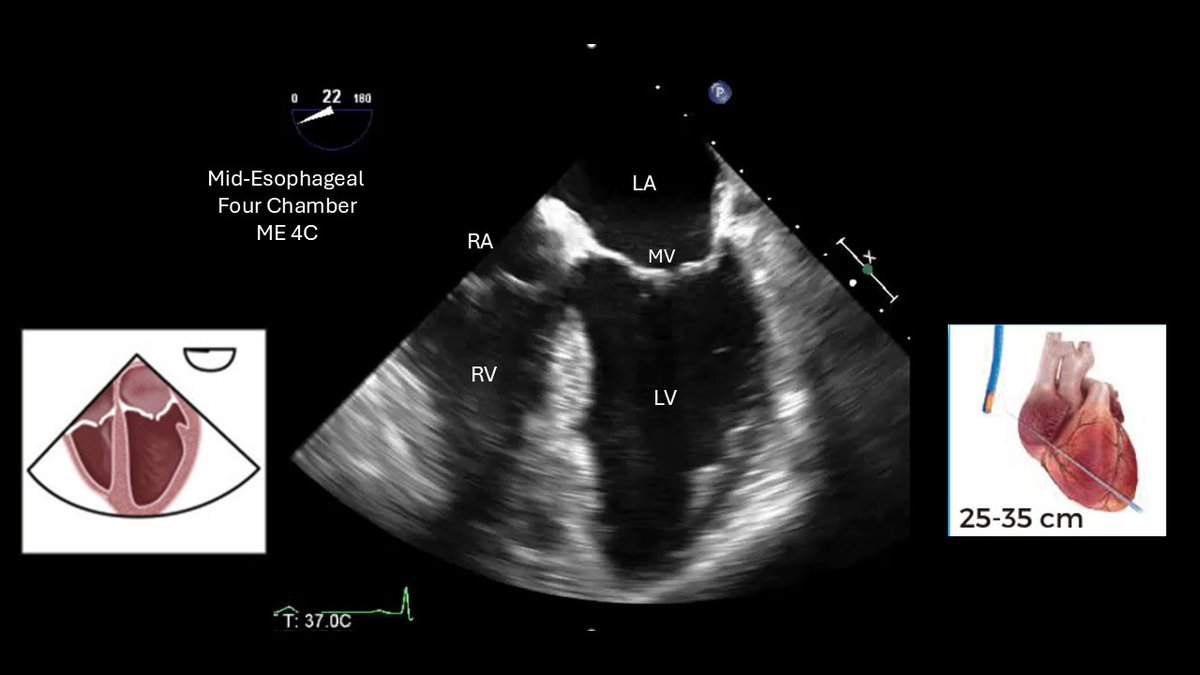
#CardioNuggets™
TEE views for fellows starting out🫀
Your FIRST view should usually be the mid-esophageal 4 chamber (~0–20°).
Why?
Because it helps orient you to:
• RA vs LA
• RV vs LV
• Mitral vs tricuspid valve
• Septum
• Overall probe position
Everything else builds from this view.
ProTip:
• The UMN TEE Simulator app is incredibly helpful for understanding how probe movement changes anatomy in real time
#CardioNuggets™ #CardioTwitter #TEE #EchoFirst
1
26
77
3,287
Bernard E Bulwer retweeted

May 22
What is best formula to estimate mPAP on #echofirst?
📝 finds minimal end-diastolic PR pressure best correlation (R = 0.92) & diagnostic accuracy AUC 0.96 bit.ly/4nQrzvm in almost 600 pts referred for RHC for PH dx, integrates both PR & TR signals
At 24.5 mm Hg cutoff, mPAPDPmin 89% sensitivity, 94% specificity
At 20 mm Hg, mPAPDPmin sensitivity⬆️99% w/ net reclassification driven by more accurate downgrading of pts w/o PH



1
54
163
8,345
Bernard E Bulwer retweeted
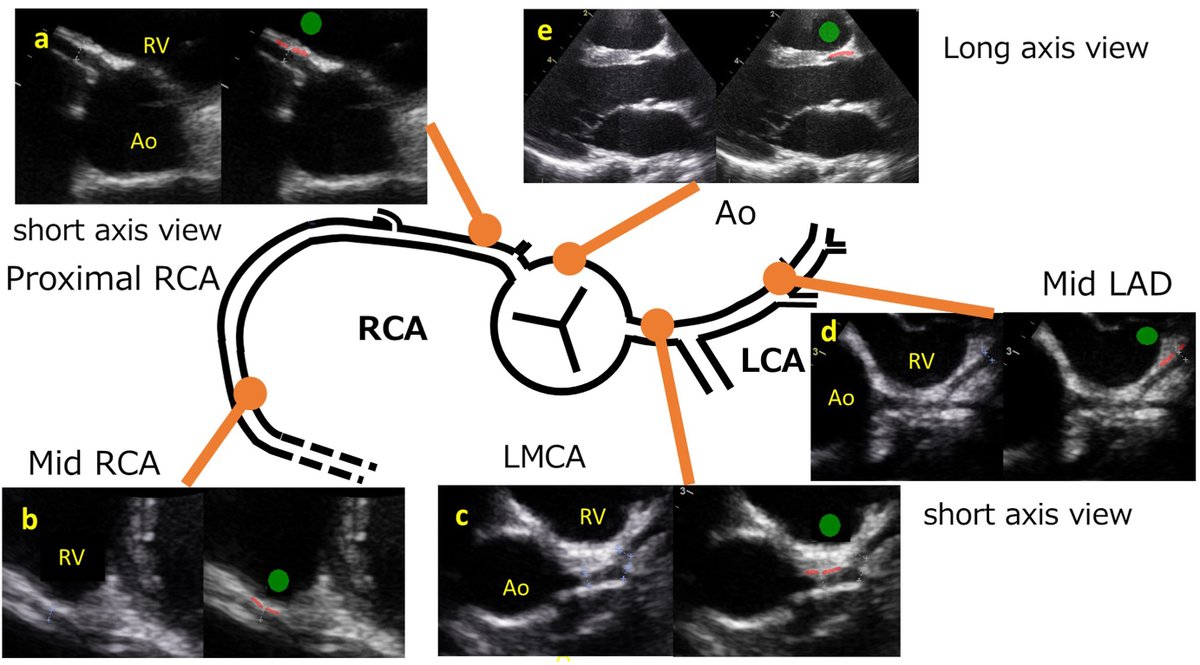
We quantitatively assessed the degree of echogenicity in the proximal and mid segments of both coronary arteries to determine its additional diagnostic value in 109 patients with clinically suspected Kawasaki disease.
Read our @JournalASEcho article: bit.ly/4dzdHkg
1
50
124
14,932
Bernard E Bulwer retweeted

How many cusps does this aortic valve have?
1️⃣ Unicuspid
2️⃣ Bicuspid
3️⃣ Quadricuspid
42
38
182
33,237
May 7
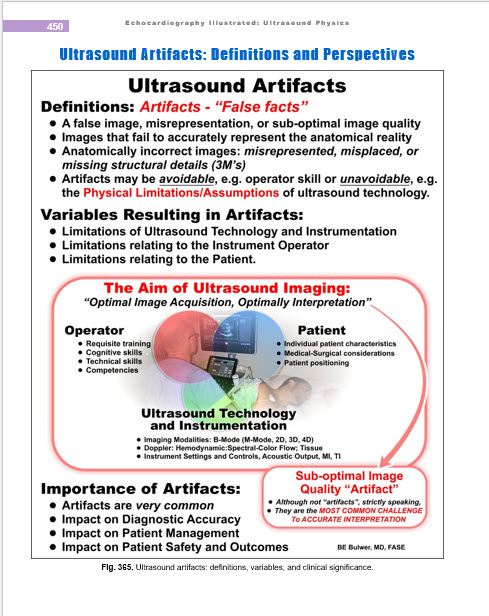
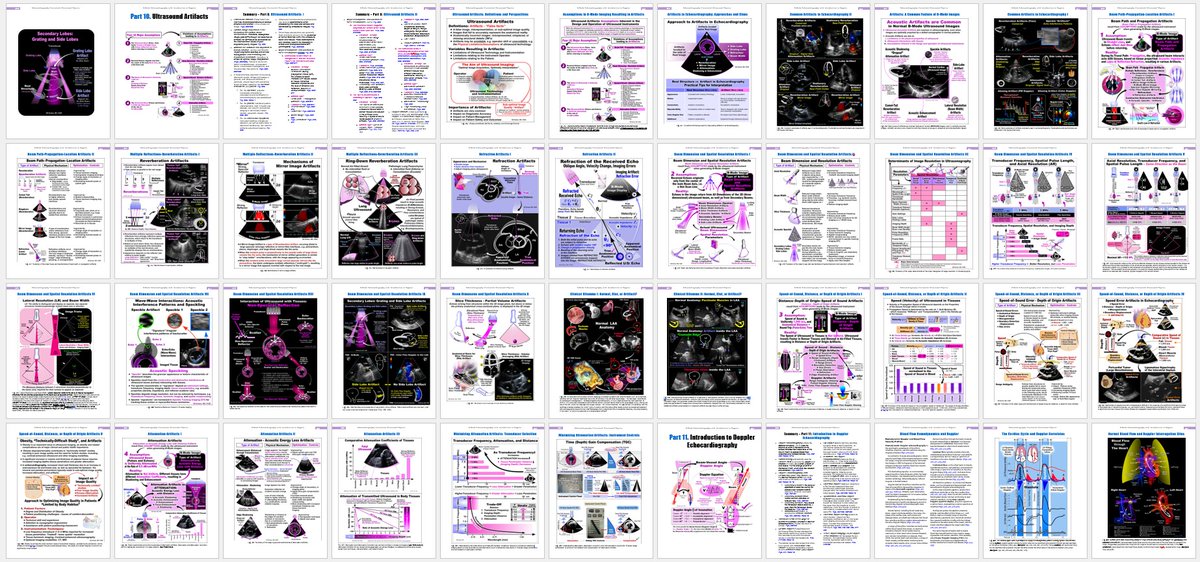
Artifacts in Echocardiography: Complementary charts and infographics. References: Echocardiography Illustrated: Ultrasound Physics: B-Mode Echocardiography and Introduction to Doppler (Echocardiograhy Illustrated Vols 9 and 10; 590 pages).
Vol 9: lnkd.in/eVcjSZcR
Vol 10: lnkd.in/eGU3n5WU
1
4
139
Bernard E Bulwer retweeted

In the fourth 👶, when a markedly dilated coronary sinus is seen : think about associated PLSVC, which can coexist with D-TGA. @iamritu @ASE360 @CASivaram1 @alex1708ander
@loomba_rohit @SIwa23288585 @CardioNeo @WithAScalpel @AEPCcongenital @swatigar @sujithsp
21 Aug 2025

In the first 👶 - just one great vessel is seen (normal)
In the second 👶 - two great vessels in parallel are seen (this usually occurs in TGA), the anterior one being the aorta
In the third 👧 - just one great vessel overriding 🏇the IVS is seen (this usually occurs in TOF)
11
41
4,593
Bernard E Bulwer retweeted
This video provides a structured approach for healthcare professionals to teach patients the Instructed Valsalva maneuver while identifying and correcting common imaging artifacts.
Learn more about our new "Goal Directed Valsalva Education Series!" bit.ly/4lR9MmF
1
8
26
3,551
Bernard E Bulwer retweeted
During intraoperative TEE in a septuagenarian undergoing aortic valve replacement and coronary artery bypass grafting, eccentric mitral regurgitation is identified. Which echocardiographic parameter should be relied upon to accurately quantify its severity?#echofirst
8
9
47
4,441
Bernard E Bulwer retweeted
In prosthetic MVR, a comet-tail artifact is a classic form of complex reverberation artifact caused by the highly reflective metallic components of the valve. @ASE360 @iamritu @CASivaram1 @alexsfelixecho @loomba_rohit @alex1708ander @SIwa23288585 @WithAScalpel @swatigar

This document provides a uniform & structured approach to managing ultrasound artifacts, including the appearance of the artifact, the mechanism behind the artifact generation, the clinical impact of the artifact on the diagnosis, & examples of real cases. bit.ly/4tKDSvf
4
30
1,637
Bernard E Bulwer retweeted
We evaluated and compared the diagnostic performance of 5 echocardiographic formulas for estimating mPAP in a large cohort of consecutive patients undergoing both RHC & TTE, applying the updated hemodynamic PH definition.
Read our @JournalASEcho article: bit.ly/3R5gqu5
1
50
191
16,516
Bernard E Bulwer retweeted
This document provides a uniform & structured approach to managing ultrasound artifacts, including the appearance of the artifact, the mechanism behind the artifact generation, the clinical impact of the artifact on the diagnosis, & examples of real cases. bit.ly/4tKDSvf
24
47
4,504
Bernard E Bulwer retweeted
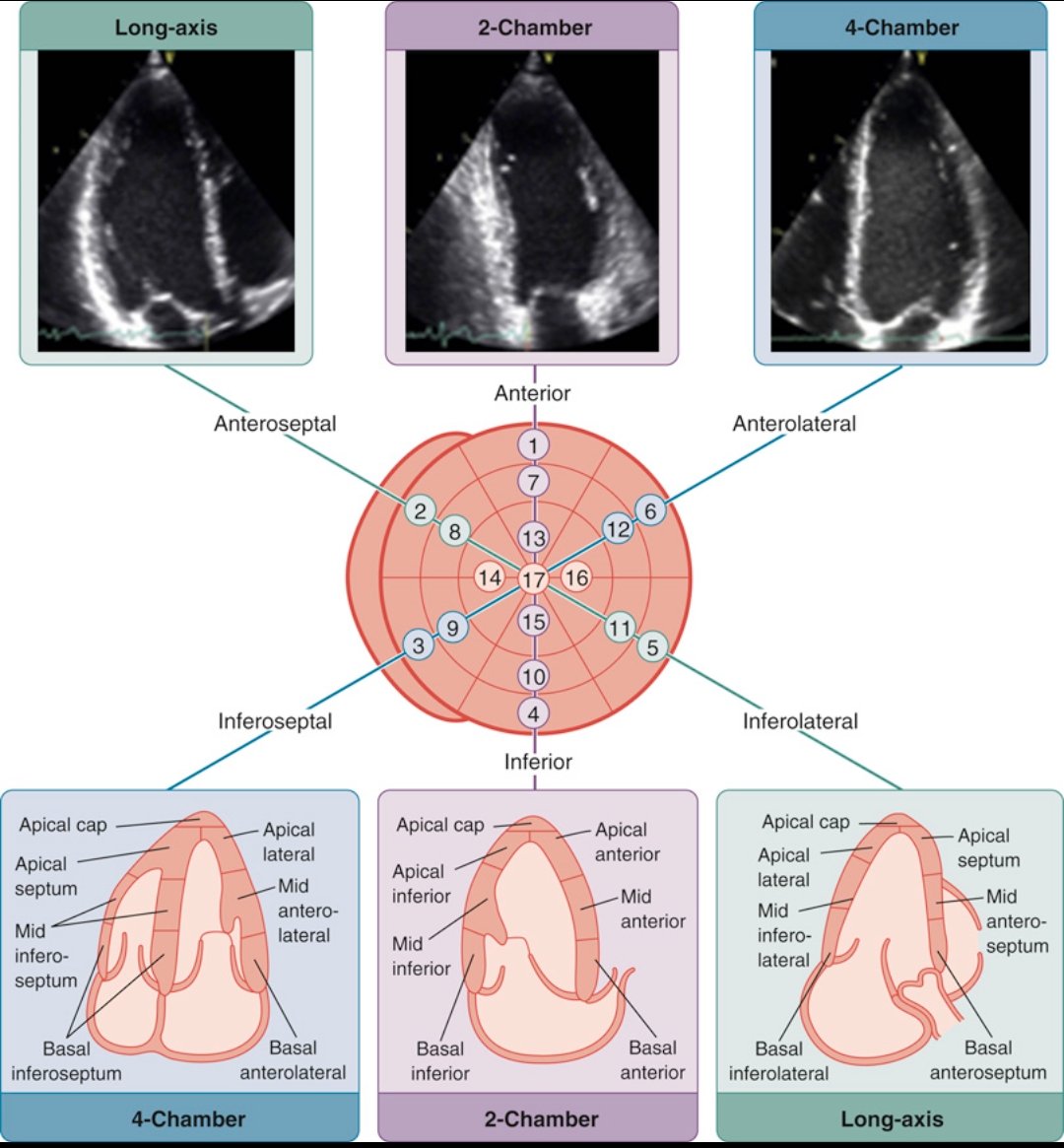
Standard echocardiographic imaging planes and the standard 17-segment model.😍
47
280
7,356
Bernard E Bulwer retweeted
Comprehensive tricuspid valve TEE analysis (mid-esophageal & transgastric views) @iamritu @OungSavly @CASivaram1 @NMerke @DrRajeshG1 @alexsfelixecho @WithAScalpel
1️⃣ ME 4Ch
2️⃣ ME RV in-out
3️⃣ ME bicaval
💚 anterior TV leaflet
💛 septal TV leaflet
💙 posterior TV leaflet
1
21
95
6,462
Bernard E Bulwer retweeted

Which all parameters to decide severity of MR in such jets?
19
25
120
29,326