I tweet in a personal capacity. ENTJ. CBE. Against brexit/Govt lies. #FBPE osf.io/pnxcs/ dbkgroup.org/longcovid/. Nothing I say is medical advice
- Tweets 273,638
- Following 10,182
- Followers 13,719
- Likes 187,360






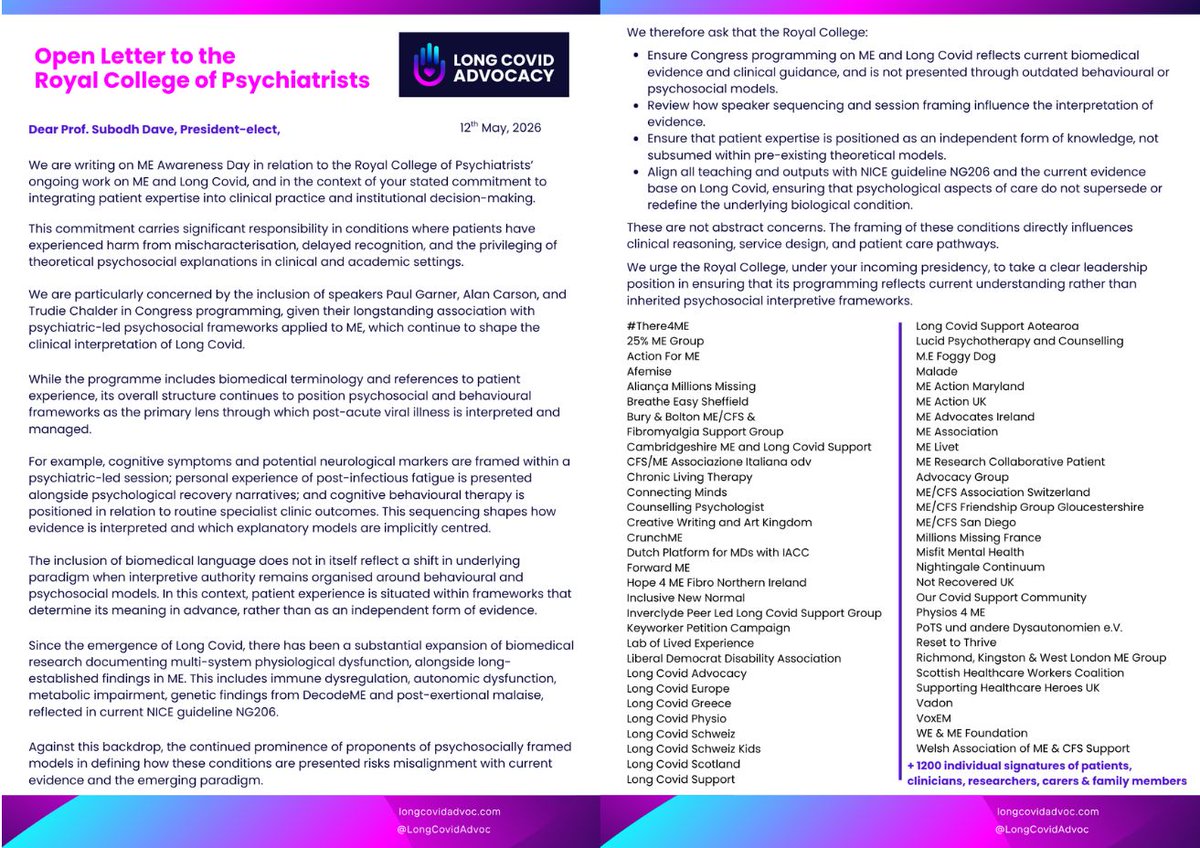
ALT Two-page Open Letter from Long Covid Advocacy to Prof. Subodh Dave, President-elect of the Royal College of Psychiatrists, dated 12th May, 2026. The letter expresses concern over Congress programming framing ME and Long Covid through outdated psychosocial/behavioural models rather than current biomedical evidence. It flags the inclusion of speakers Paul Garner, Alan Carson, and Trudie Chalder, arguing their frameworks risk misaligning with NICE guideline NG206. The text outlines four demands: Ensure programming reflects biomedical evidence, not psychosocial models. Review how speaker sequencing shapes evidence interpretation. Position patient expertise as independent knowledge. Align all teaching with NICE guideline NG206. The letter is signed by a two-column list of 58 supporting organizations (including Long Covid Advocacy, Action for ME, ME Association) and " 1200 individual signatures of patients, clinicians, researchers, carers & family members." Footer lin

ALT Campaign infographic titled "#HearOurVoices" and "#RCPsychIC", demanding better ME and Long Covid framing from the Royal College of Psychiatrists. Left side shows a woman pushing a young woman in a wheelchair on a path. Below this, a dark block titled "1 Why?" states 58 orgs and 1200 people signed an Open Letter regarding concerns over Long Covid framing at the 2026 International Congress, noting "our concerns remain." The main text outlines a "Social Media Campaign" with three steps: 1) JOIN community outreach on June 15th, 2) POST your story for congress attendees, 3) AMPLIFY using tags #RCPsychIC and #HearOurVoices. It provides a post template supporting up-to-date scientific representation and meaningful patient engagement. Bottom right includes a pink QR code, a link to "longcovidadvoc.com", and the "LONG COVID ADVOCACY" logo. A bright pink footer reads: "International response raises concern about Congress framing of Long Covid."