
Engineering👨💻 #WSWS supporter ☭ 🇵🇸#CovidIsAirborne #N95 😷#ZeroCOVID #BanCars
Joined October 2008
- Tweets 30,360
- Following 3,885
- Followers 1,315
- Likes 153,101
1,245 Photos and videos












Pinned Tweet

27 Jul 2024
I have 350,000 lines of mostly JavaScript, PHP, SQL, and browser extension code related to completing microtasks on Amazon Mechanical Turk (mturk.com). I don't really have any use for it anymore. But I spent nearly 10 years working on it. 1/
4
1
4
342
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

Trump is planning a ground invasion of Iran
A ground invasion of the Iranian coastline would not be a limited or contained operation. It would be a protracted and gruesome bloodbath. @WSWS_Updates
wsws.org/en/articles/2026/03…
4
4
79
Mar 10
RT @BigBadDenis: "Leading vaccinologist Helen Petousis-Harris says there's not enough awareness of the impact of COVID-19 on overall health…
558
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

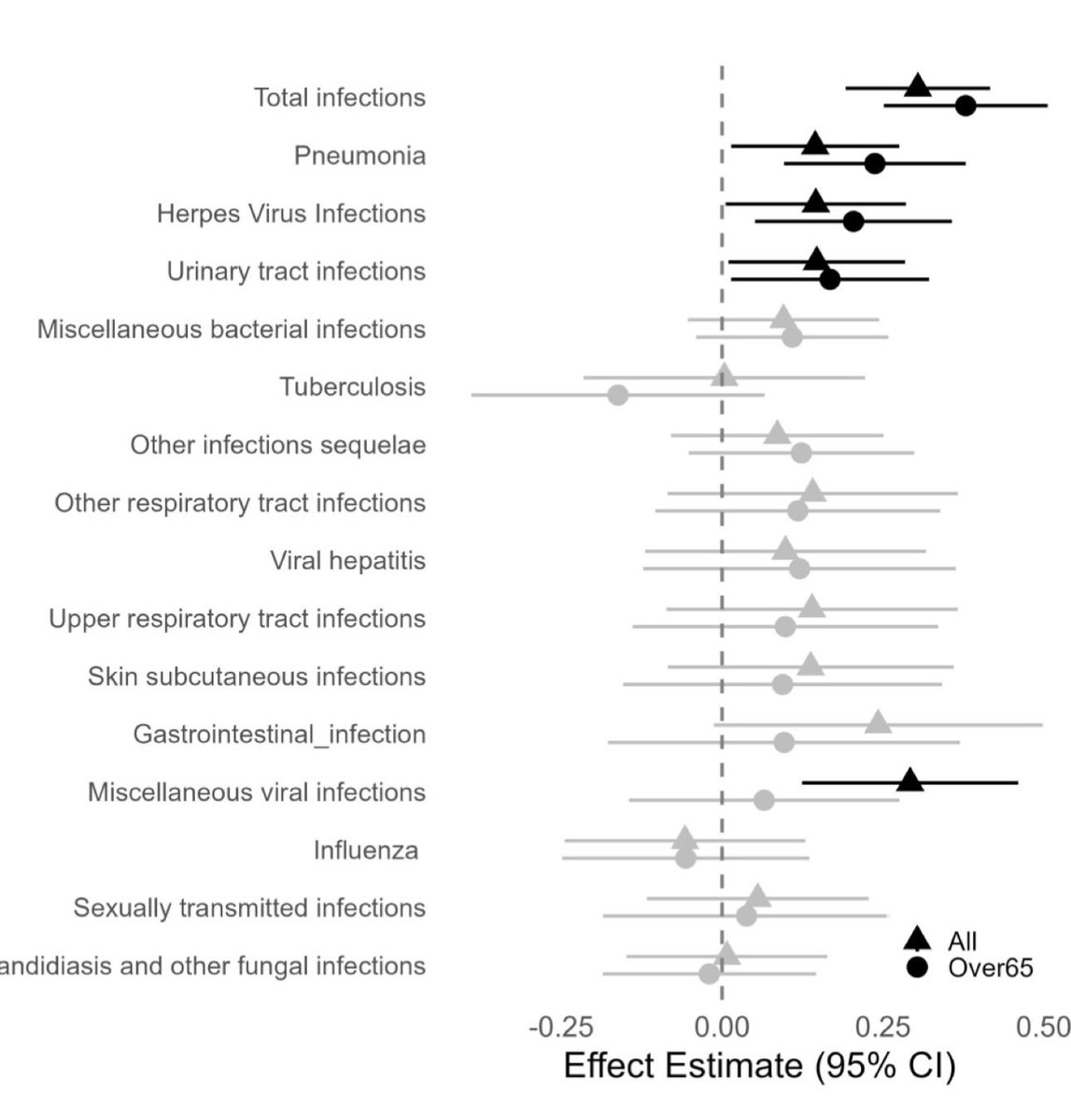
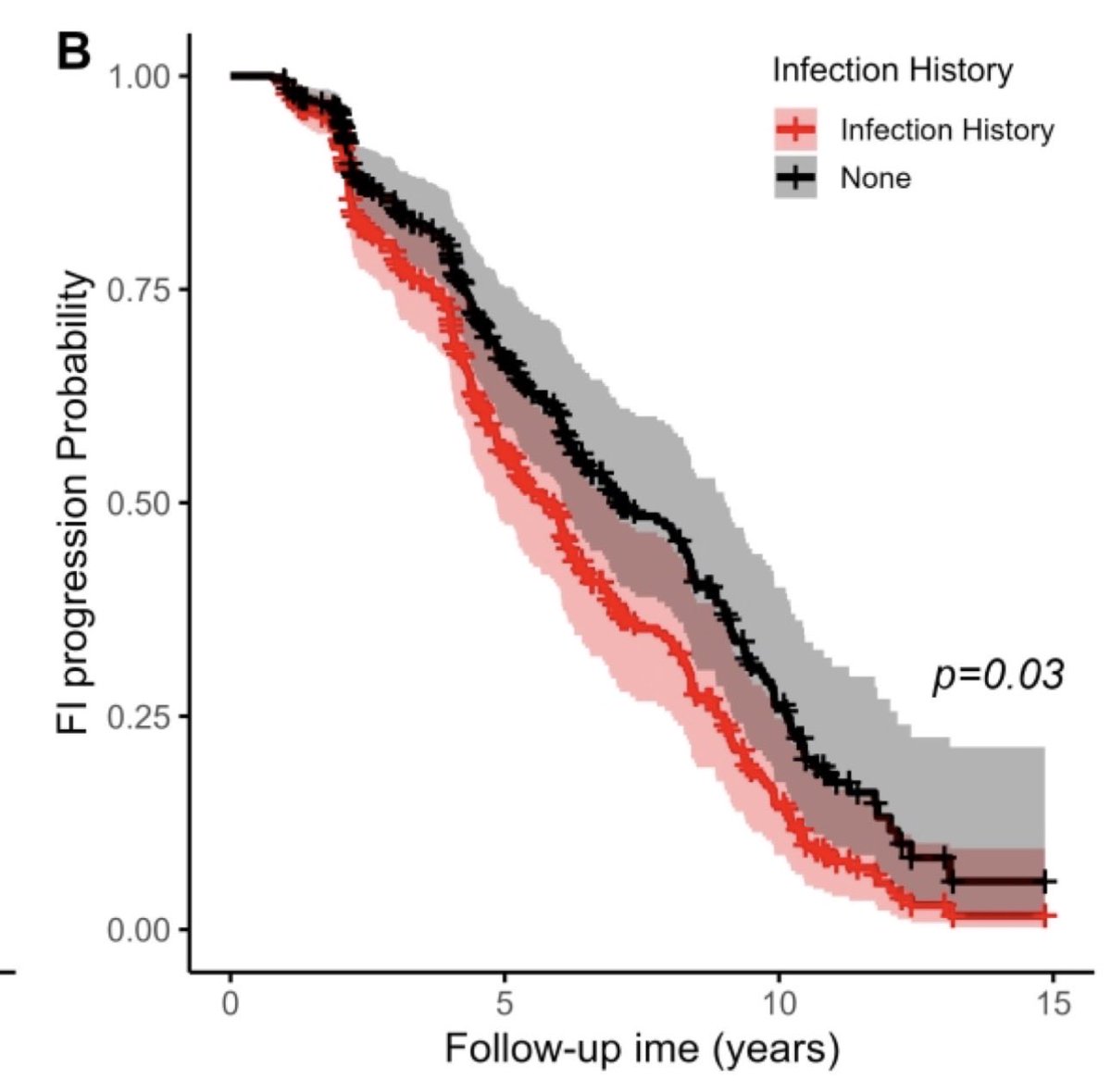
During their lives, centenarians rarely get sick. New paper with 1,400 subjects finds a history of infections (pneumonia, herpes, UTIs) associates with earlier frailty. The authors speculate that obesity makes people more susceptible & that viral infections may accelerate aging
81
327
2,216
222,774
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

Feb 22
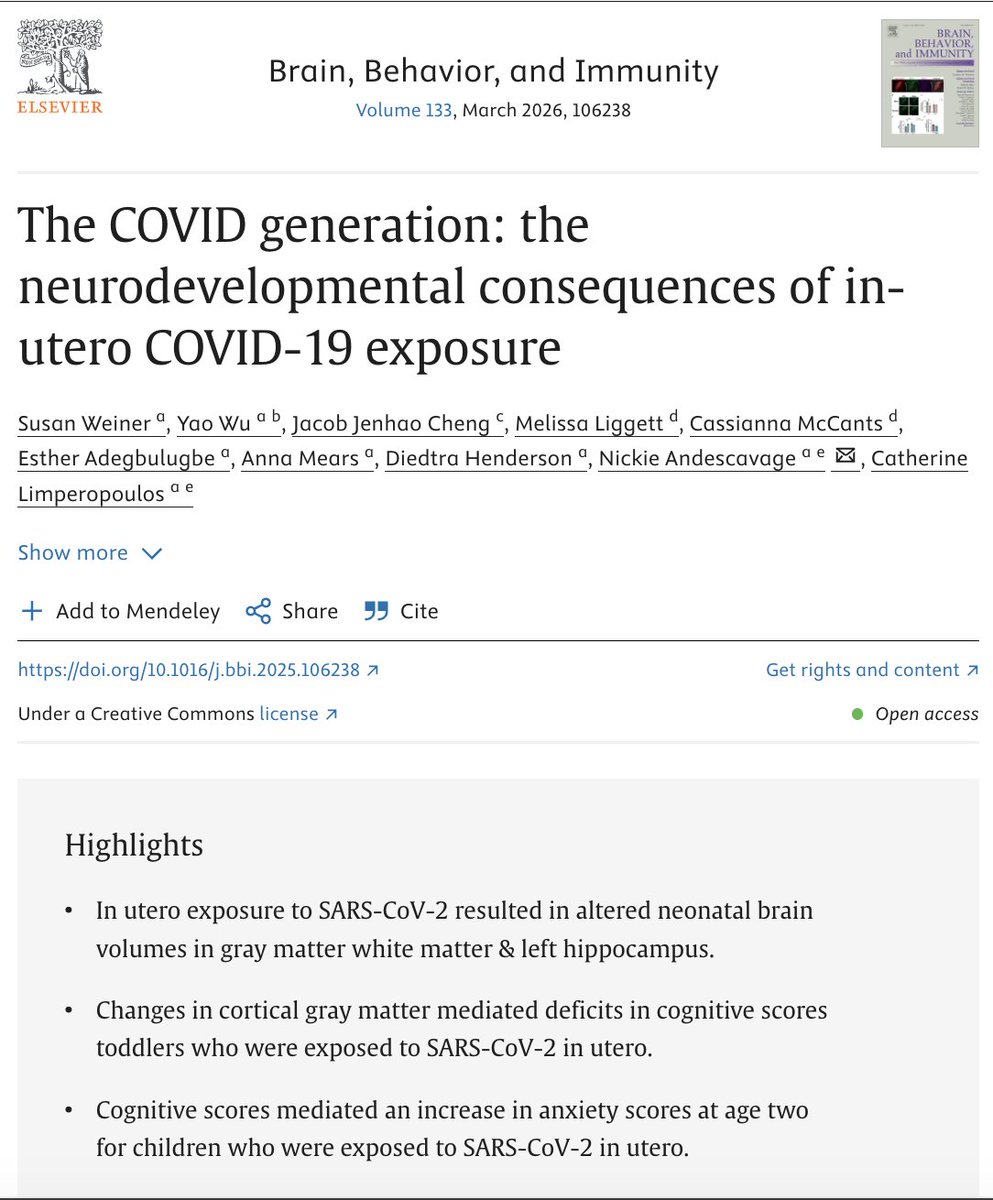
This is not good news, and explains some of what we are seeing in K-1 classrooms right now:
Increased emotional dysregulation.
Memory and learning issues.
Speech delays.
Fine and gross motor delays.
So many kindergarten kids coming to school still in diapers.

36
570
1,348
37,894
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

Feb 19
The authors of this study no doubt spent hundreds of hours of their lives on this - all of that time was completely wasted.
As you would expect just from the headline, this study suffers from numerous methodological problems and biases. I'd be ashamed to have my name associated with it. A few examples:
1. The authors compare patients who had a healthcare visit and tested positive for COVID to patients who had a healthcare visit and tested negative for COVID.
Fine, but people do not go to the doctor and get a PCR test for no reason. The "control" group that tested negative for COVID was sick enough, or exposed enough, to warrant a medical visit and a test. This means they really don't have a control group. If not COVID, those people will have other infections that can also cause long lasting symptoms. Thus, the study is not comparing the effects of COVID to a healthy baseline. It is comparing Long COVID to "Long Flu", etc. This makes the excess risk of COVID look less significant.
2. PCR tests are not perfect, and their accuracy depends heavily on timing.
The "test-negative" group will contain false negatives due to people who tested too early or too late. If these false negatives go on to develop Long COVID, it dilutes the difference between the two groups.
3. And finally the worst of all: billing codes. This methodological flaw is well known to anyone with even a passing interest in this space. It should be disqualifying from ever doing research on Long COVID. Long COVID symptoms (brain fog, PEM, etc) do not easily fit into billing codes, and many doctors don't understand them, so they don't get coded at all.
The authors conclude that patients see a "return to baseline health within approximately one year" due to lack of billing codes. This doesn't mean that they returned to health - only that they stopped seeking treatment. Which makes sense, since there are no effective treatments for Long COVID, and the ones that do exist aren't found within the traditional medical system.
Feb 19

Stanford University researchers analyzed 14.4 billion claims from 244.7 million US patients and found long COVID may be far less common and shorter lasting than thought, with most excess risks fading within 1 year after infection.
medrxiv.org/content/10.64898…
10
67
355
14,366
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

Feb 11
🔥 Proud dad moment — and this needs to be seen. 🔥
My freshman daughter is actively bringing attention to masking at her high school — not because it’s trending, but because it matters for her classmates’ health and comfort during an ongoing pandemic. 🎓💪
She wrote an opinion piece for her school paper about what a simple mask reveals about individual choice, respect, and safety — and it deserves to be read by more than just her classmates.
📎 Read her full piece here: champaignchronicle.com/staff…
Whether you agree or disagree — let’s have a real conversation in the comments.
❤️ Share if you agree with her courage.
🔁 Retweet so more people see this.
#MaskingMatters #StudentVoice #ProudDad #PublicHealth #ChampaignCentral
champaignchronicle.com/staff…
36
132
582
7,932
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

Some major fucking dots getting connected here


5
82
349
9,214
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

Feb 9
As a retired public health policy person, I cannot get over the suspension of the Precautionary Principle.
With a BSL-3 virus.
After almost 20 years of data on those who survived SARS-CoV-1.
While knowing that coronaviruses tend to mutate frequently.
10
217
874
18,113
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

Jan 17
A couple of very important studies out just in the last 24 hours confirming what we've been saying for years and years now: Covid infections affect your immune system *badly*.
Here's a few things you may have missed in them.
32
590
1,793
89,949
Jan 17
RT @GangstHannah: Your fight against fascism should include resisting state sponsored forced Covid infections.
You should be masking to pr…
278
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

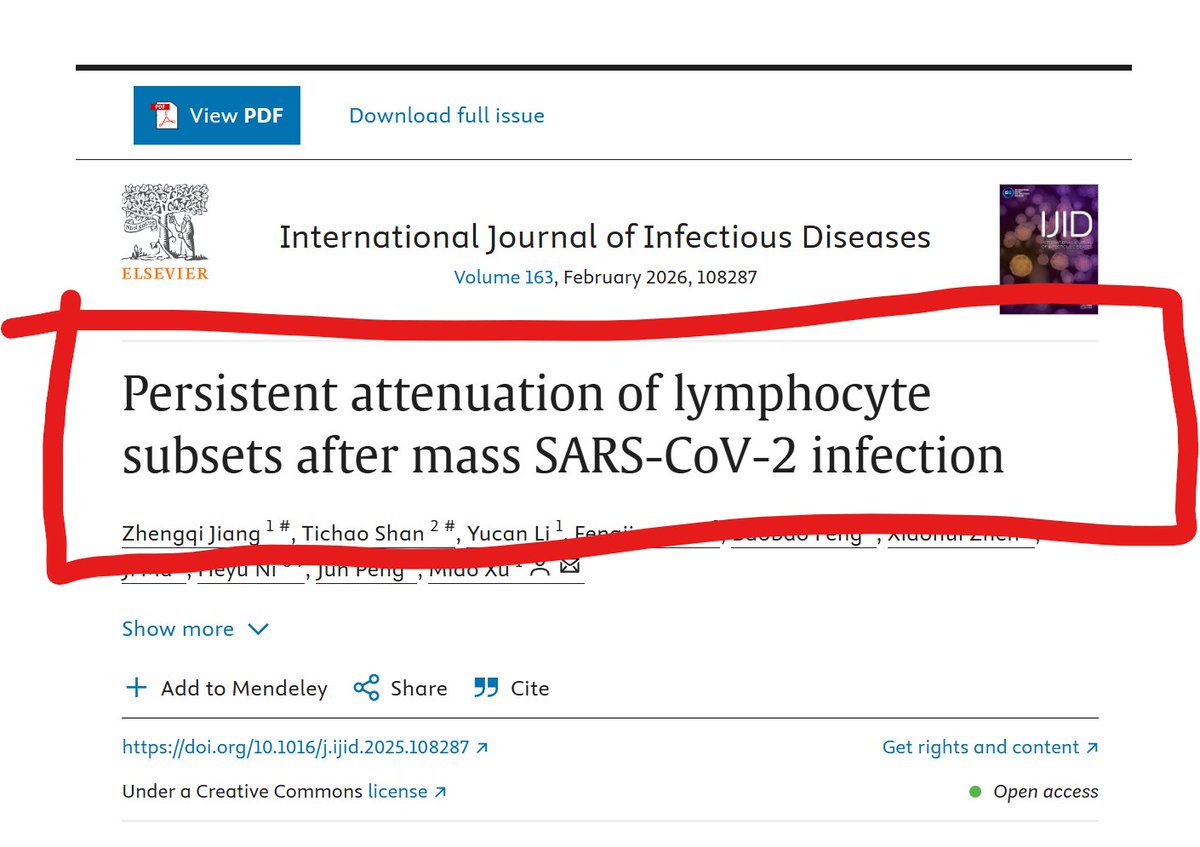
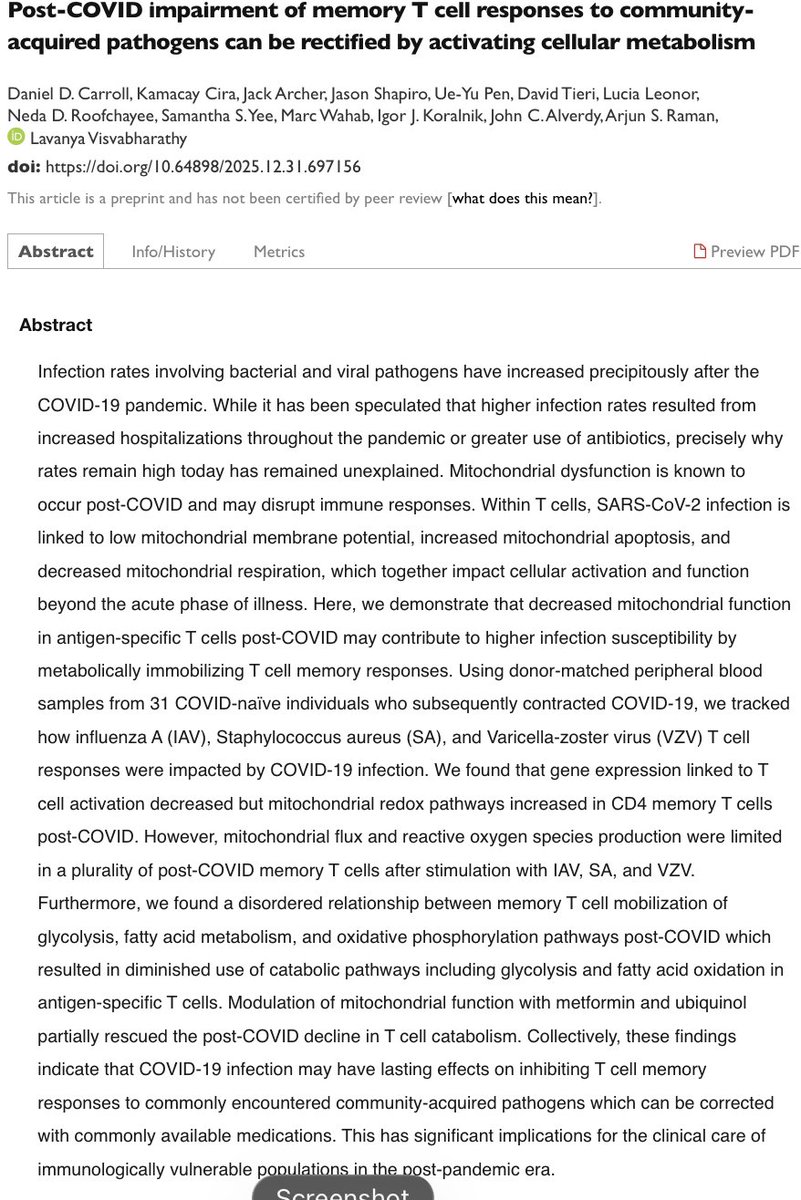
Key finding: Post-COVID patients show markedly reduced T cell reactivity to common pathogens (influenza, Staph, VCZ) which is evidence of lasting immune dysregulation favoring secondary infections and viral reactivation
Link:
biorxiv.org/content/10.64898…
2/5
18
457
1,275
128,026
Jan 4
RT @themermacorn: Joe Biden carried out a GENOCIDE. Obama bombed and starved Yemen for the entirety of his presidency. Toppled governments…
6,184
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

Jan 3
⚡️#BREAKING Venezuela's defense minister is alive and has released a video message calling for an "anti-imperialist and liberation war" against the American empire.
1,430
8,363
40,736
1,266,251
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

27 Dec 2025
Xiamen University scientists analyzed brain tissue from COVID-19 patients and found that infection changes how brain cells process mRNA, disrupting genes tied to memory, cognition, and psychiatric disease.
journals.plos.org/plosone/ar…
14
268
1,203
305,463
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

28 Dec 2025
Fucking hell @jonstewart. Way to use your platform to punch down at the people FOLLOWING THE ACTUAL SCIENCE unlike you, who sucked up all the capitalist propaganda

19
115
796
8,770
28 Dec 2025
RT @Lizzardo77: Hey @jonstewart from one former fan... You fancy yourself a social justice warrior? Covid infections (even mild) are ruinin…
272
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

26 Dec 2025
John Stewart and the guy (Favreau 🤮) who harassed us for advocating for respirators, LC research/funding, etc are having fun mocking people who wear respirators out there.
This is why we call them all "shitlibs".
20
197
1,640
59,237
ZeroCovidNow 🇵🇸😷☭🚲 retweeted
26 Dec 2025
Source @JudahWorldChamp (I took the video from Instagram)
46
181
1,400
340,524
ZeroCovidNow 🇵🇸😷☭🚲 retweeted

27 Dec 2025
This shit is so depressing. I am simply trying to survive as a person who was disabled by a covid infection. Why would @jonstewart of ALL ppl go out of his way to mock me. It’s like they’re trying to make the world completely unsurvivable for us. The lack of empathy is staggering
109
565
3,537
179,852