
Sur 1 mois. Pas de quoi s'affoler.
On verra bien sur l'année.
Rappelons que les AcVC font davantage de morts que les AVP.
128


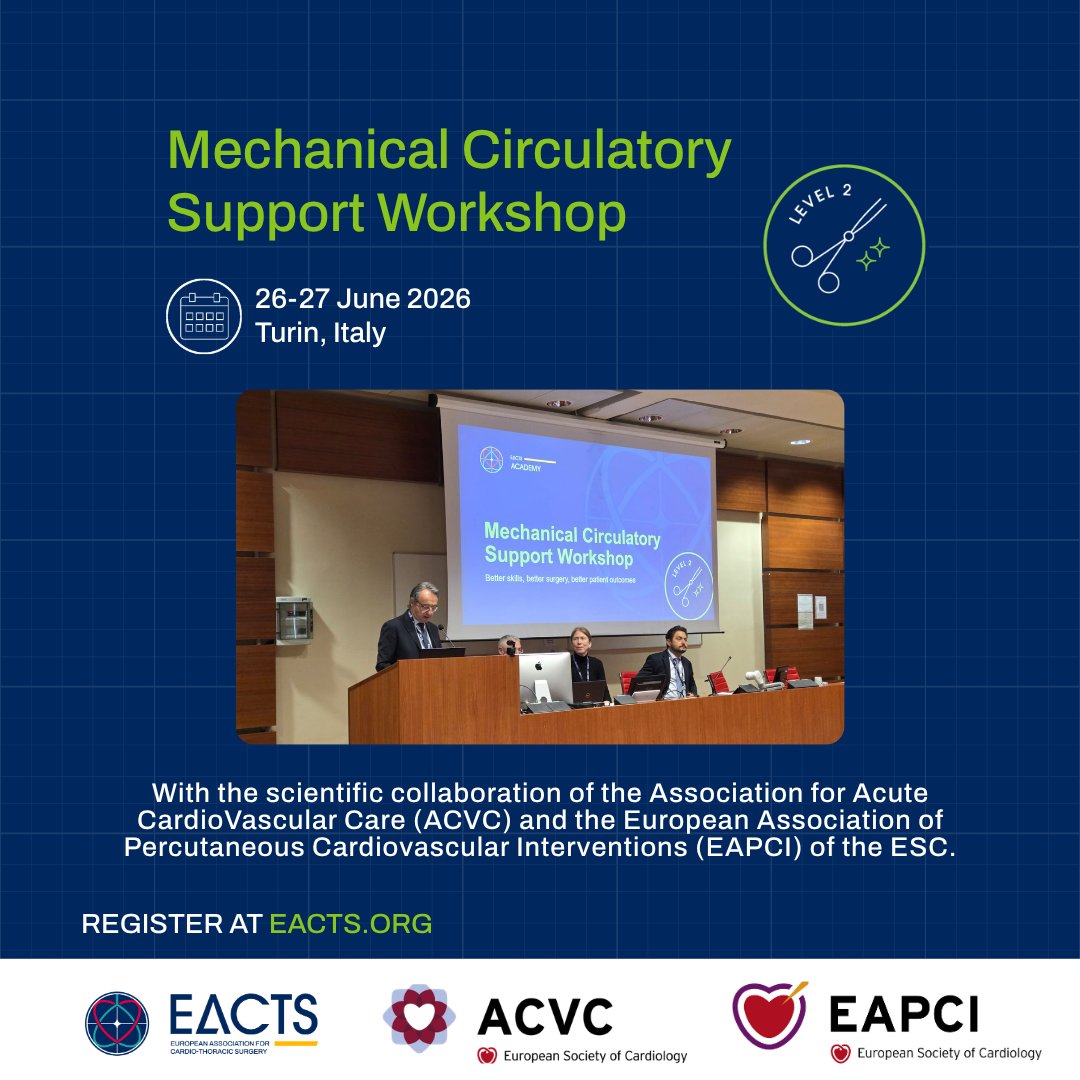
⏳ Just two weeks to go until the Mechanical Circulatory Support (MCS) Workshop!
Be part of this intensive two-day workshop featuring lectures, debates, and hands-on surgical practice. You will receive didactic instruction, dry-lab operative experience, and practical demonstrations in surgical techniques essential for both short-term and durable MCS systems.
If you plan to attend the annual EACTS MCS Summit, the MCS Workshop provides a valuable opportunity to gain practical experience and deepen your understanding in preparation for the Summit.
Delivered in scientific collaboration with the Association for Acute CardioVascular Care (ACVC) and the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC.
🗓️ 26-27 June 2026
📍 Turin, Italy
We are grateful to our platinum sponsors of the Mechanical Circulatory Support Workshop: Abbott, Abiomed (Johnson & Johnson MedTech), Getinge and HXCORMED.
Secure your place today 🔐 eacts.org/education/eacts-ac…
@EAPCIPresident
@alaide_chief
@marioiancardio
@VPanoulas
@ACVCPresident
@ASionis
2
261
Epic Literary Artist retweeted

May 31
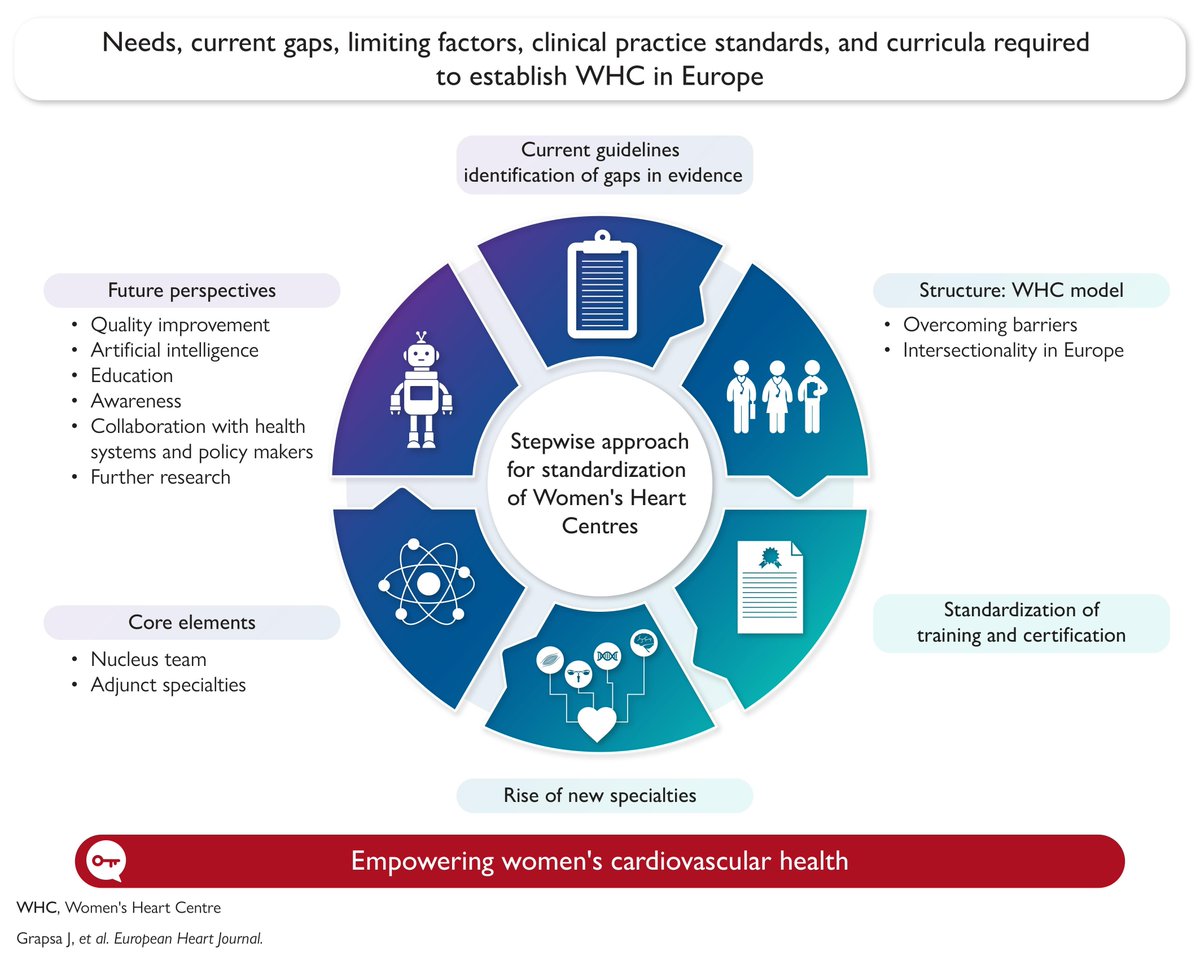
Women's hearts deserve dedicated care. New ESC clinical consensus from EACVI, EAPCI, HFA & ACVC defines what a true Women's Heart Centre should look like. Read more in #EHJ.
doi.org/10.1093/eurheartj/eh…
#women #cardiotwitter @ESC_Journals @escardio
14
29
2,016

Jun 7
⎐كُـود⎐كوبِون⎐خـِصم⎐
⎐الدهام⎐
⊵DW682⊴
⎐مذركير⎐
⊵A7BAu⊴
⎐نون⎐
⊵CBB54⊴
⎐ممزورلد⎐
⊵jor⊴
⎐ماماز▬اند▬باباز⎐
⊵M24⊴
⎐بلومنغديلز▬بلومينغديلز⎐
⊵d15⊴
اتش اند ام
A6JP
A6MA
⎐بوما⎐
⊵X70⊴
***
aCVc
2

AcuteCVDays over the last 5 weeks delivered an excellent educational journey through the modern spectrum of cardiogenic shock and acute cardiovascular care. 🫀💓
From STEMI related shock to electrical storm, right ventricular failure, inflammatory heart disease, and acute heart failure progressing toward shock, one message became clear:
Cardiogenic shock is not a single diagnosis. It is a dynamic syndrome.
Week 1 reminded us that mechanical circulatory support is not “one size fits all.” VA ECMO may save selected patients, but routine early ECMO for all STEMI related cardiogenic shock is not supported by current evidence.
Week 2 moved into electrical storm, showing that recurrent ICD shocks are not only arrhythmic events, but also drivers of sympathetic activation, myocardial stress, and hemodynamic collapse.
Week 3 focused on the right ventricle, perhaps one of the most underestimated determinants of acute deterioration. RV failure forces us to think beyond LVEF and integrate afterload, ventilation, pulmonary circulation, and venous congestion.
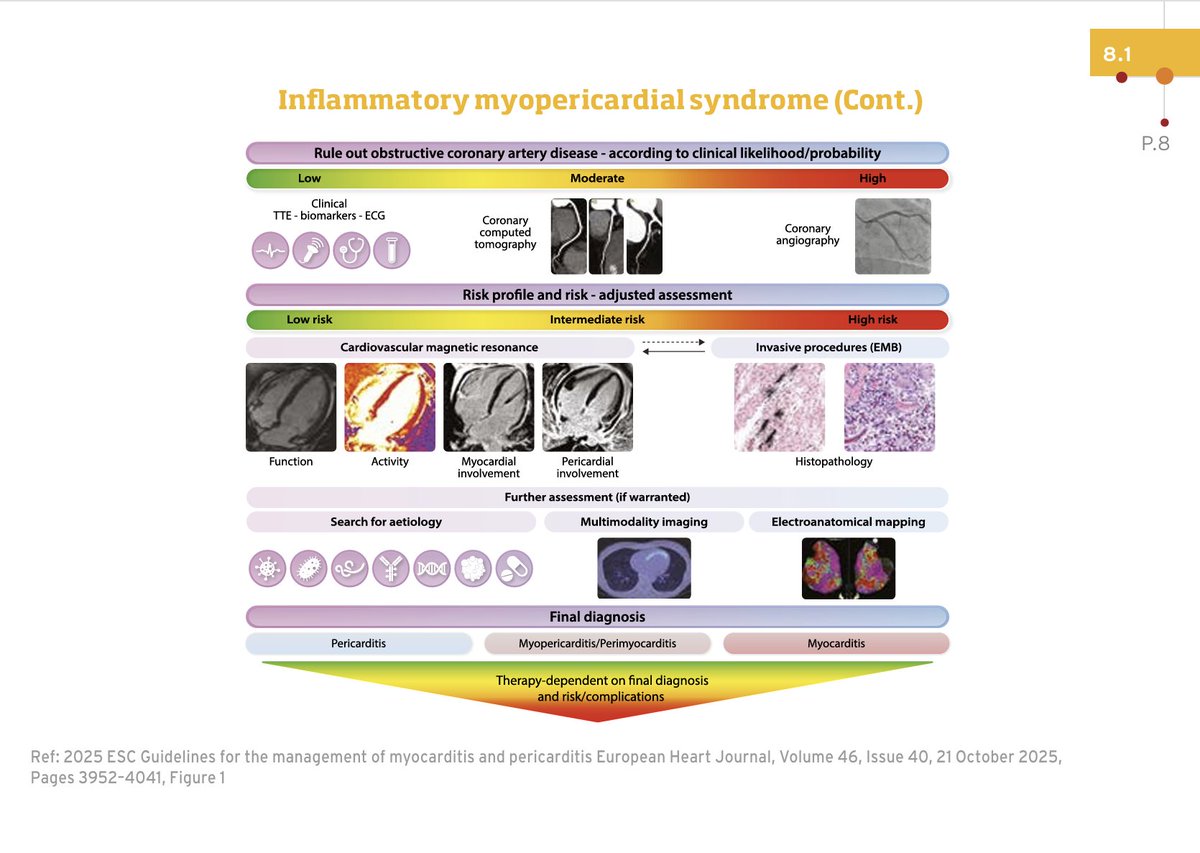
Week 4 explored the inflamed heart: myocarditis, pericarditis, endocarditis, and beyond. It challenged us to recognize that elevated troponin and ST changes with unobstructed coronaries may represent inflammatory myocardial disease, where cardiac MRI, biopsy in selected cases, and early risk stratification matter.
Week 5 completed the spectrum by addressing acute heart failure and the transition toward cardiogenic shock. The key lesson: shock is not defined by blood pressure, but by inadequate tissue perfusion.
Across all five weeks, the common thread was physiology based decision making.
Not every shock patient needs ECMO. Not every ST elevation is coronary occlusion. Not every preserved LVEF excludes cardiovascular collapse. Not every hypotensive patient is the same. And not every deteriorating patient gives us time.
Excellent initiative by ACVC, bringing together clinical cases, expert discussions, quizzes, and practical tools for the acute cardiovascular community.
escardio.org/communities/ass…
#AcuteCVDays #ACVC #ESC #CardiogenicShock #AcuteHeartFailure #ElectricalStorm #RightVentricularFailure #Myocarditis #CriticalCare #Cardiology #IntensiveCare #MedEd
ALT
2
6
609
Join leading heart failure specialists in Turin for two days of expert learning and exchange at the Mechanical Circulatory Support Workshop, taking place from 26-27 June.
Delivered with the scientific collaboration of the Association for Acute CardioVascular Care (ACVC) and the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC.
You will explore evolving technologies, patient selection strategies, clinical outcomes, and surgical approaches alongside internationally recognised experts in the field of MCS.
Whether you are a surgeon, interventional cardiologist, anaesthesiologist, perfusionist, acute care specialist, VAD coordinator, or heart failure nurse, the Workshop is designed to strengthen your multidisciplinary understanding and improve patient care.
🚨 Don’t miss this chance! Register now ⛓️💥 eacts.org/education/eacts-ac…
@EAPCIPresident
@alaide_chief
@marioiancardio
@VPanoulas
@ACVCPresident
@ASionis
1
3
395

Jun 5
★ブランドニュース★
ArmorSource
米国 防弾ヘルメット
2026年5月28日に米陸軍向けに2万5000個のAdvanced Combat Helmets 戦闘ヘルメット第2世代(ACH Gen II)を製造・納入する1,760万ドル(約28億1,600万円)の契約を獲得
ACH Gen IIヘルメットシステムは、高度な防弾性能を提供すると同時に、全体の重量を軽減し、戦闘員の快適性を向上させるように設計されています。
軽量構造、人間工学に基づいた設計、そして実証済みの性能により、幅広い作戦環境における任務遂行能力を支援します。
この契約はArmorSource社が長年にわたり築いてきた、米陸軍、海兵隊、海軍、米特殊作戦軍を含む米国防衛関連組織とのパートナーシップに基づいています。
また、ArmorSource社は次世代型CREW II先進戦闘車両乗員用ヘルメットシステム14,000個の納入に成功したことを受け、2025年に追加契約として1,860万ドル(約29億7,600万円)契約を獲得。
2030年までに米陸軍へ最大3万個のACVCヘルメットの追加納入が行われます。
詳細価格は下記製品ページよりご確認いただけます。
【ArmorSource ヘルメットシステム】
militive.com/shopbrand/ARMOR…
【AireSupport Max Premium Suspension System ヘルメットパッド】
米陸軍およびNIJレベルIIIA試験プロトコルに対応。
米陸軍AR/PD 14-01規格に準拠した鈍的衝撃保護性能と背面変形性能を提供します。
militive.com/shopdetail/0000…

7
52
5,340
🤔A provocative ICU thought from Week 4 of #AcuteCVDays:
Sometimes the inflamed heart behaves more aggressively than the ischemic heart.🫠
Fulminant myocarditis may evolve within hours from:
• Mild chest pain
• Preserved LVEF
• Modest troponin elevation
…to refractory cardiogenic shock requiring:
• High dose vasopressors
• VA ECMO
• Mechanical ventilation
• Temporary pacing
• Mechanical circulatory support, and yet early diagnosis remains difficult because presentations are extraordinarily heterogeneous.
This week’s ACVC material highlights a critical concept: Myocarditis is not one disease. It is a spectrum.
Viral injury.
Immune mediated inflammation. Autoimmune overlap.
Toxic triggers.
Genetic susceptibility.
Inflammatory cardiomyopathies.
The real challenge is identifying which patient will deteriorate.
That is why contemporary management increasingly integrates:
• Clinical phenotype
• Arrhythmic burden
• Biomarkers
• Echocardiography
• Cardiac MRI
• Selective endomyocardial biopsy
• Hemodynamic profiling
The old paradigm viewed myocarditis mainly as a diagnosis of exclusion.
The modern paradigm treats it as an active inflammatory cardiovascular syndrome requiring early risk stratification, and perhaps the most important question: Are we recognizing fulminant myocarditis before circulatory collapse occurs?
Worth watching this week’s case discussions and quiz 🤓.
#ACVCDays #FulminantMyocarditis #VAECMO #ShockTeam #CriticalCareCardiology #HeartFailure #Inflammation #ESC
References
Arad, M. Trends in Cardiovascular Medicine. Advance online publication. doi.org/10.1016/j.tcm.2026.0…
Schaubroeck, H. (2026). ESC Acute CardioVascular Care 2026 Congress Presentation. esc365.escardio.org/presenta…

ALT
1
6
14
3,571
🗓️ One month to go until the Mechanical Circulatory Support (MCS) Workshop.
Join us in Turin on 26-27 June for two days dedicated to the latest developments, challenges, and practical uses in mechanical circulatory support.
This hands-on workshop brings together experts and multidisciplinary heart failure teams, creating a focused setting to share knowledge, discuss new technologies, and explore different approaches to temporary and long-term MCS systems.
Delivered with the scientific collaboration of the Association for Acute CardioVascular Care (ACVC) and the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC.
Secure your place today 🔐 eacts.org/education/eacts-ac…
@EAPCIPresident
@alaide_chief
@marioiancardio
@VPanoulas
@ACVCPresident
@ASionis
1
4
334

May 27
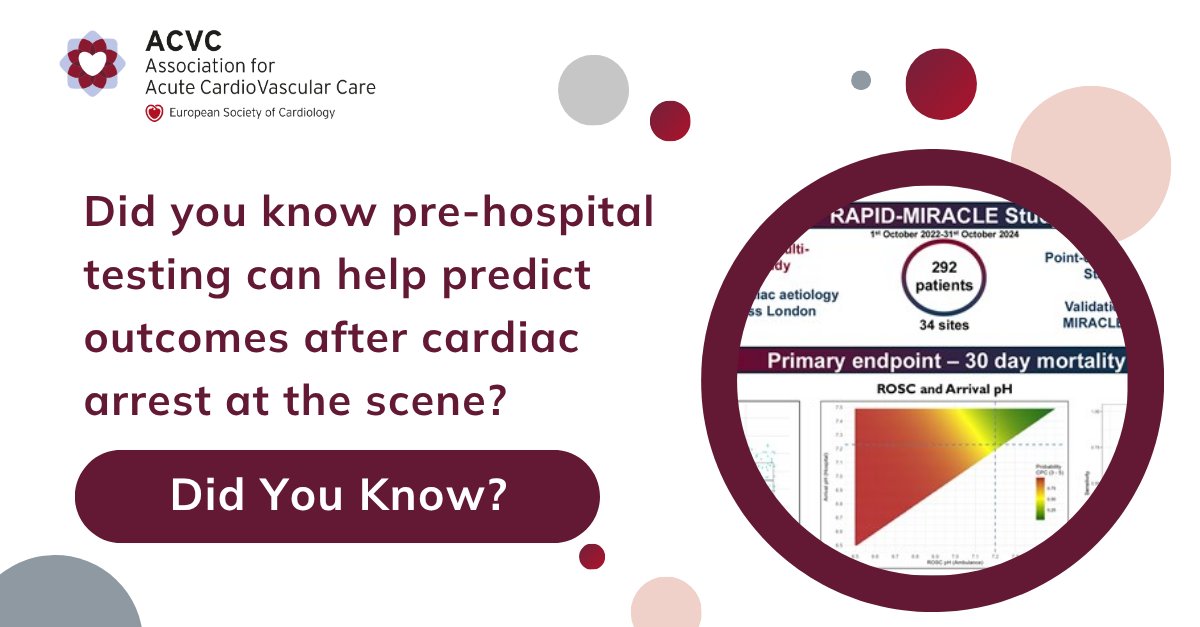
Did you know new insights are refining risk assessment in acute cardiovascular care?
Research in EHJ-ACVC highlights emerging approaches to improve outcome prediction and management.
Learn more 👇
oxford.ly/4fJ56ht
#DidYouKnow #Cardiology #EHJACVC @EHJACVCEiC @escardio
ALT EHJ-ACVC Did You Know Series\n
2
484
May 27
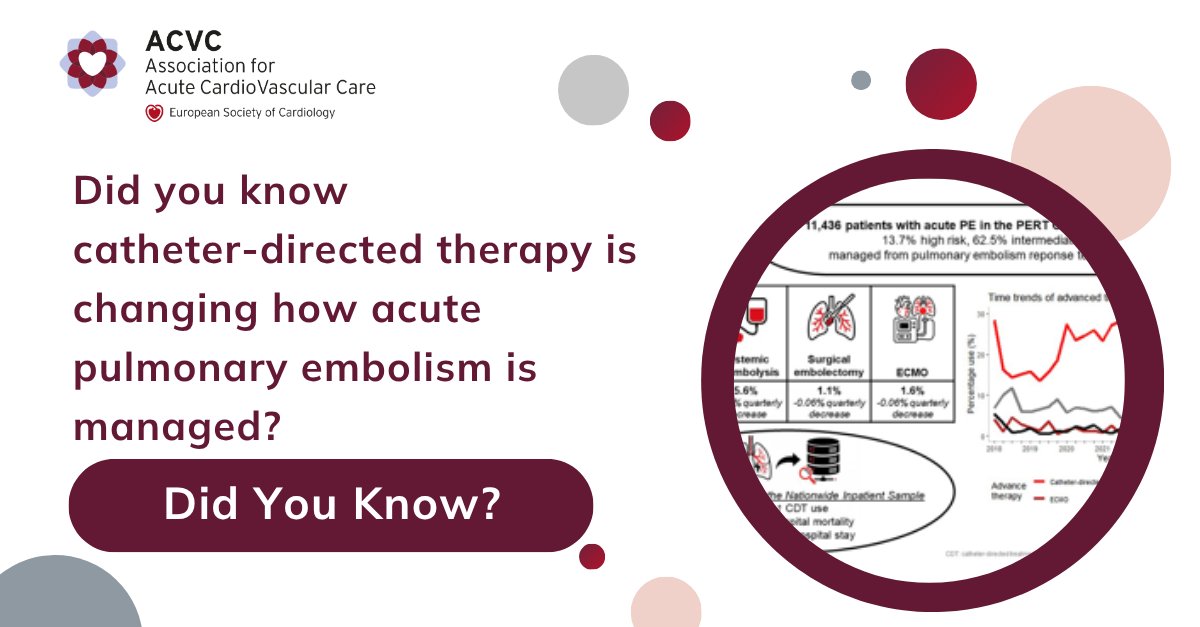
Did you know catheter-directed therapy is changing how acute pulmonary embolism is managed?
New research in EHJ-ACVC shows a shift towards advanced therapies and wider use of PERT models.
Read more 👇
oxford.ly/49p2npK
#DidYouKnow #PulmonaryEmbolism #EHJACVC
ALT EHJ-ACVC Did You Know Series\n
1
395

May 26
⭐️Just published in @ESC_Journals #EHJ
Women's heart centres: a clinical consensus statement of the European Association of Cardiovascular Imaging (EACVI), the European Association of Percutaneous Cardiovascular Interventions (EAPCI), the Heart Failure Association (HFA), and the Association for Acute CardioVascular Care (ACVC) of the ESC academic.oup.com/eurheartj/a…
4
17
891

Week 4 of #AcuteCVDays is ongoing with the topic "The Inflamed Heart: (peri)Myocarditis, Endocarditis & Beyond"
You can join a lot of free #ACVC resources and dedicated ACVC #Toolkit Chapter here: lnkd.in/dgyvbzKK
1
6
185

May 25
#AcuteCVDays continue with always hot topic
This week's focus is on the inflammatory heart syndromes ♨️
How and did the guidelines really changed our practice?
This week on our website you can find:
✅ Overview of #ESCCongress Guidelines session
🧑🏿💻ACVC Webinar
💬Case-based discussion by #ACVC_ESC experts
📖#ACVCToolkit chapter
🧑🏿🏫An expert practical review
⁉️ Quiz, MCQs
Don't miss it, all the resources are FREE
lnkd.in/dgyvbzKK
@HannahSchaubro1 @CVandenbriele @escardio
6
8
1,444
💓Chest pain. Diffuse ST elevation. Elevated troponin. Normal coronaries.
How many “STEMI activations” are actually inflammatory heart disease?
Week 4 of #AcuteCVDays explores one of the most clinically dangerous diagnostic crossroads in acute cardiovascular care: distinguishing acute myocarditis and myopericarditis from acute coronary syndromes.
The challenge is not theoretical. It is real world emergency medicine.
Because myocarditis can present with:
• ST elevation
• Troponin release
• Ventricular arrhythmias
• Cardiogenic shock
• Fulminant biventricular failure
• Sudden death and sometimes the patient is only 18 or 28 years old with no cardiovascular history.
One of the most important contemporary shifts highlighted this week is the growing central role of cardiac MRI. In hemodynamically stable patients with suspected inflammatory myocardial disease and non obstructive coronaries, CMR is increasingly becoming the diagnostic cornerstone rather than an optional second step.
But the provocative question is this:
How many patients with “MINOCA” are actually inflammatory syndromes that remain underdiagnosed?
The new ESC perspective on inflammatory myopericardial syndromes is pushing clinicians toward earlier phenotyping, risk stratification, and multimodality imaging integration.
Because not all troponin elevations are ischemic. And not all ST elevation belongs in the cath lab algorithm.
Excellent ACVC educational content this week.🤓
#ACVCDays #Myocarditis #Pericarditis #MINOCA #CardiacMRI #CardiogenicShock #CriticalCare #AcuteCardiovascularCare #ESC
References
Arad, M., Trends in Cardiovascular Medicine. Advance online publication. doi.org/10.1016/j.tcm.2026.0…�
Chiorazzo, L. Journal Acute Cardiovascular Care. esc365.escardio.org/journal/…

ALT
9
18
2,815
Not all cardiogenic shock is “cold and wet” left ventricular failure.
Some patients are actually dying from a ventricle we still systematically underestimate.
🫀The right ventricle operates at the edge of physiologic reserve. Small increases in pulmonary vascular resistance can trigger:
• RV dilation
• Septal shift
• Reduced LV filling
• Coronary hypoperfusion
• Multi organ failure.
And unlike LV failure, compensatory mechanisms are limited.
What makes RV shock especially dangerous is diagnostic delay.
The patient may initially appear:
• “Fluid responsive”
• Only mildly hypotensive
• With preserved LVEF
• Without obvious pulmonary edema
Meanwhile, venous congestion and systemic hypoperfusion are already progressing.
This week’s ACVC educational material correctly places echocardiography at the center of acute RV evaluation. Not as an optional imaging modality, but as a real time hemodynamic tool.
The key question is no longer: “Does the RV look bad?”.🤔
The better question is: “Is the RV still coupled to the pulmonary circulation, or is decompensation already underway?”
That distinction may determine whether the patient requires:
• Fluids
• Diuresis
• Pulmonary vasodilators
• Inotropes
• Mechanical support
• Or immediate reperfusion for pulmonary embolism
Excellent topic choice by ACVC and EACVI because RV failure remains one of the least standardized and most physiologically demanding areas in cardiovascular intensive care.🫶🏻
#AcuteCVDays #RVFailure #PulmonaryEmbolism #CardiogenicShock #Hemodynamics #CriticalCare #EACVI #EchoFirst #IntensiveCare #ESC

ALT
1
16
46
1,811
What did participants think of last year’s Mechanical Circulatory Support Workshop?
📊 98% said the course met their expectations, was a good investment, and that they would recommend it to a colleague.
Participants appreciated the expert-led discussions, dry-lab training, and the positive impact the workshop had on their clinical practice and understanding of MCS.
Find out why last year’s participants rated the Workshop so highly and join us this year in Turin from 26-27 June. You’ll experience two days of hands-on learning, device simulations, operative sessions, and multidisciplinary discussions focused on both temporary and durable mechanical circulatory support.
Delivered with the scientific collaboration of the Association for Acute CardioVascular Care (ACVC) and the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC.
Register now 🔗 eacts.org/education/eacts-ac…
@EAPCIPresident
@alaide_chief
@marioiancardio
@VPanoulas
@ACVCPresident
@ASionis

1
2
346
🫀Week 3 of #AcuteCVDays asks a deceptively simple question:
What happens when the right ventricle fails?
For decades, acute cardiovascular care focused predominantly on the left ventricle. Yet in the ICU, RV failure often represents the tipping point between compensation and collapse.
A dilated RV is not merely an echocardiographic finding. It is a hemodynamic warning signal:
• Reduced LV preload
• Systemic venous congestion
• Worsening renal and hepatic perfusion • Escalating vasopressor requirements
• Progressive cardiogenic shock.
And perhaps most importantly: RV shock is frequently underestimated until late stages.
This week’s ACVC and EACVI collaboration highlights one of the most challenging realities in modern cardiovascular intensive care: the right ventricle is exquisitely sensitive to afterload, volume strategy, and ventilatory settings.
How often do we unintentionally worsen RV failure?
• Excessive PEEP
• Aggressive fluids
• Delayed pulmonary embolism recognition
• Inadequate echocardiographic assessment
• Overreliance on LV oriented shock paradigms.
🤓The provocative question is not whether RV failure is dangerous.
The question is whether we diagnose it early enough.
The interactive case and quiz are excellent reminders that echocardiography is not simply confirmatory in RV shock. It is central to diagnosis, phenotyping, and therapeutic guidance.
Would you confidently distinguish:
• Acute cor pulmonale?
• RV infarction?
• Massive PE?
• Chronic pulmonary hypertension with acute decompensation?
• Septic RV dysfunction?
Because management changes dramatically depending on the answer.
Excellent educational initiative from ACVC and EACVI.
escardio.org/communities/ass…
#AcuteCVDays #RVFailure #CardiogenicShock #EACVI #CriticalCare #Echocardiography #PulmonaryEmbolism #AcuteCardiovascularCare #IntensiveCare #ESC
ALT
1
6
14
1,970