Commodore Computer Museum 🕹 retweeted

14 Jun 2025
N* PETSCII #01 for ATL (31st May 2025) 🎶PETSCII graphics for the Commodore 64
Download from CSDB. Released by NthSt4r.
5
15
1,742


Jun 8
경상수지 측정의 자의성(안물안궁)
비거주자(외국인)가 국내의 부동산을 구입하는 것은 금융계정(Financial Account)의 '직접투자(FDI)'로 처리합니다.
예를 들어 한국 사람이 뉴욕의 신축 아파트를 $100만에 구입하면, 미국의 국제수지에서 경상계정, 금융계정은 어떻게 변화할까요?
🔴현존 회계 방식: 직접투자로 분류하며 금융계정에 나타남
원칙: CSDB± (Sell한 것은 Credit에 , Buy 한 것은 Debit에 -로)
미국 금융계정
Credit: $100만(주택 매각)
Debit : -$100만(달러 예금을 매입한 것으로 해석)
금융 계정에서만 거래를 포착하므로 경상수지에는 영향이 없음
🔴그런데 만약 신축 아파트를 소비재(또는 투자재)로 분류하면?
미국 경상계정
Credit: $100만(주택 매각)
미국 금융계정
Debit : -$100만(달러 예금을 매입한 것으로 해석)
결과 👇👇👇
경상수지(흑자) $100만
금융수지(적자) - $100만
🔴 결론
신규 주택 거래는 GDP에서는 투자에 속합니다. 신규 주택을 투자재로 보는 것이죠. 그런데 이것을 외국인이 매입하면 투자재를 수출한 것이 아니라 외국인이 직접투자를 하는 것으로 분류합니다.
미국 기계 설비 생산은 미국 GDP에 잡힙니다. 이를 한국 기업이 매입했을 때는 미국의 경상수지 흑자로 잡힙니다. 신규 주택의 독특한 특성 때문에 이런 일이 발생합니다.
신규 주택은 국내 생산을 측정하는 GDP에서는 투자재로, 국제 거래를 측정하는 국제수지에서는 직접투자로 분류하는 존재가 애매한 항목이 됩니다.
17
1,435

May 31
Here you go. The whole things is great. Enjoy :)
[CSDb] - Coma Light 13 by Oxyron (2012)
csdb.dk/release/?id=112378
1
7
134

May 30
Data 0,
L’infinita possibilità prima del tour vero e proprio.
Rimini, ho passato due notti di prove perfette
230 tende in attesa della data per Il Blasco fan club.
25.000 il 29/5
25.000 il 30/5
Ringrazio tutti voi, e ringrazio chi rende possibile questo evento passando giorni e notti davanti ai computer, montando e smontando il mio palco.
Tutti i reparti e tutte le persone che rendono possibile questo evento
Divertiamoci tutti 🤟🫵
#ilblascofanclub #rimini #csdb #vascolive026
📷 #alessandra_trucillo #gianluca_simoni #roberto_villani #chiaroscurocreative




11
18
159
6,134
New Commodore 64 Demo: ALOFT (2026) by Quiss & Genesis Project
Just released at Fjälldata 2026. Very impressive work with smooth effects and excellent design. A strong release that shows the C64 scene is still going strong after all these years. Download the demo from CSDB.
2
7
78
4,210

May 7
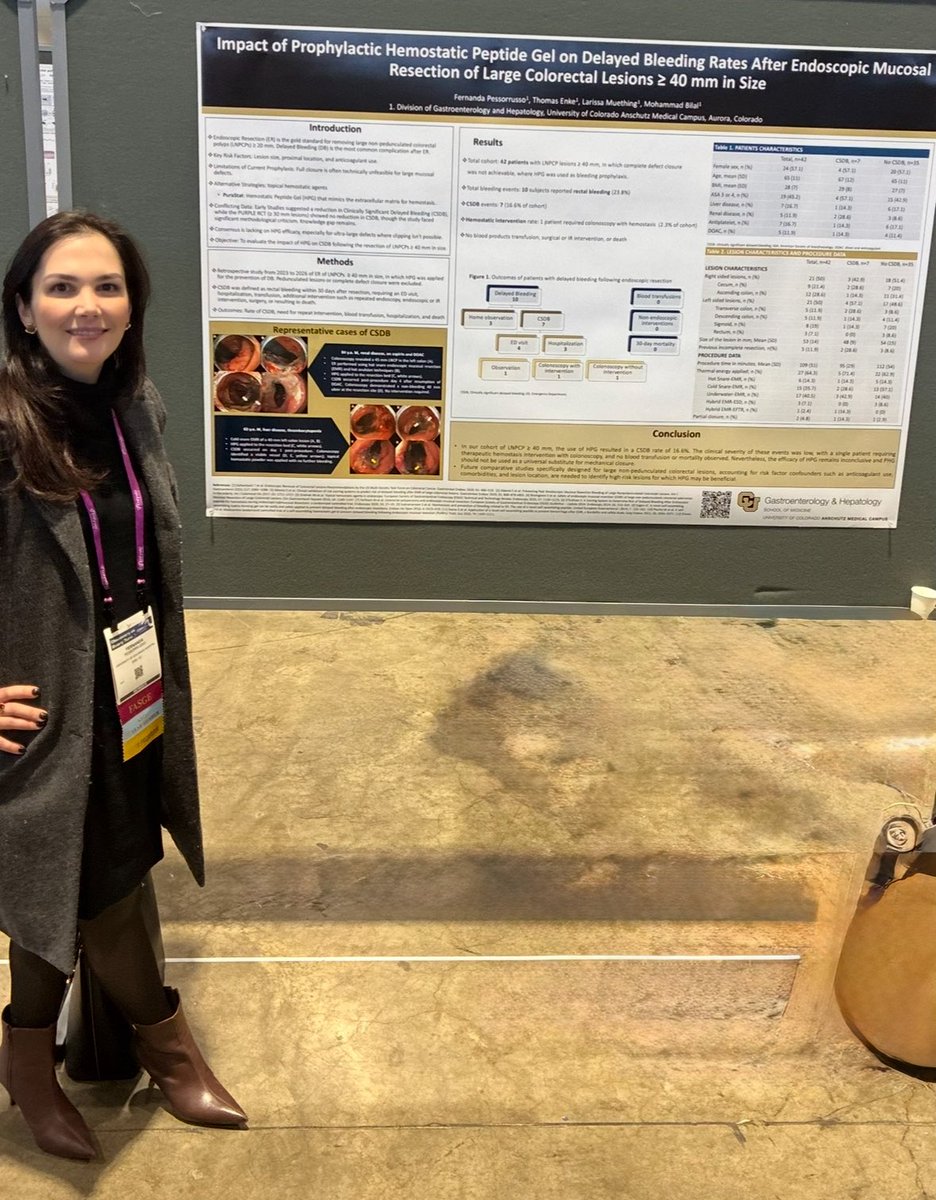
x.com/bilalmohammadmd/status…
対象:大型大腸病変のEMR(ESD)
42病変(≥40 mm)
遅発性出血(Delayed bleeding):
9/42 = 21.3%
Clinically significant delayed bleeding (CSDB):
7/42 = 16.6%
再内視鏡止血が必要:
1例
輸血・手術・死亡:
なし

So proud of @CUDeptMedicine ⭐️ resident @FPessorrussoMD for her presentation on use of “Hemostatic gel for prophylaxis of delayed bleeding after colon #EMR”
#DDW2026 @DDWMeeting
1
7
1,025
Insane Amiga like graphics on the Commodore 64? Dreamtime 2k17 by Profik!
How Demos Like "Dreamtime 2K17" Achieve Amazing Images
In this 2017 C64 demo release by Profik, the graphics uses a hires FLI interlaced mode with per-line X-shifts. Resulting in a highly detailed slideshow of images with good color mixing, though it can show flicker on some displays (common trade-off). Still amazing on a Commodore 64, right!?
I am no expert on how sceners achieve such beautiful things on the C64 - I am in awe as to what they do - so I researched this and here's a break down on the techniques Profik has mastered for this demo/slideshow.
Key techniques involved:
1. FLI (Flexible Line Interpretation):
• Normally, the VIC-II only fetches color/attribute data on "badlines" (every 8th scanline).
• By tweaking the vertical scroll register ($D011) at precise times each scanline, coders force a badline every single line. This lets the system pull fresh color data per raster line instead of every 8.
• Result: In hires FLI, you get 2 colors per 1×8 pixel strip (much finer control). In multicolor FLI variants, up to 4 colors per very narrow area.
2. Interlacing (IFLI or similar):
• Two frames are alternated at 50Hz (or 60Hz).
• One frame is often shifted by 1 pixel horizontally (via $D016 X-scroll).
• This creates the illusion of higher resolution (closer to 320px effective) and more color blending, as the eye/CRT mixes the flickering pixels. It can look stunning on a real CRT but may flicker more on emulators or modern displays.
3. Per-line X-shifts (D016 writes):
• Fine horizontal scrolling is adjusted differently on each line to minimize artifacts, optimize color placement, and reduce visible errors in the "FLI bug" area (left side of screen where the trick sometimes glitches).
4. Other enhancements:
• Sprites as underlays/overlays (in NUFLI-style modes): 8 hardware sprites cover parts of the screen for extra colors or detail without clashing with the bitmap.
• Precise raster interrupts and cycle-exact code to change registers mid-frame.
• Custom converters that map modern images to these modes, choosing colors to minimize flicker and maximize perceived quality.
These tricks require insane timing — the CPU is often busy syncing perfectly with the video beam, leaving little room for other effects. That's why these demos feel magical: they're breaking the rules of the hardware in ways Commodore engineers never intended.
Download this demo from CSDB.
3
10
60
2,772
Battlestar Galactica intro (2006) mashed up with the excellent SID music from The Fall Guys (1986). The combo of the two works well. You can download both (as seperate prgs) from CSDB.
(no offense intended to the original creators, by mashing these two together.)
1
7
81
1,974
Great Giana Sisters 5: Castles and Dungeons. First time playing this newly released (2 April 2026) GGS game. It’s faithful to the original, and it’ll take me a few runs to get the timing right.
Commodore 64 fans well know the storied history of The Great Giana Sisters, the C64’s answer to Super Mario Bros. It’s a great game—every bit as good as the Nintendo one.
GGS: Castles and Dungeons (2026), a Construction Set by Merlin from 7A3, is super challenging on the first go—maybe even harder than the OG. I just started level two, which throws in another element I’ll have to get used to. Tough stuff. I will keep at it 😆
You can download GGS: Castles and Dungeons (2026) from CSDB.
1
7
44
3,107
Bon Jovi "Livin' On A Prayer" on the Commodore 64!
Released by : Hokuto Force [web]
Release Date : 1 April 2026
Type : C64 Music 🎶
One of my favourite 80s bands, and a song that's very fitting right now — about a couple struggling through economic hardship.
I've got my Commodore 64 hooked up to Infinity speakers and a sub, and this C64 SID music sounds awesome. Turn it up!
Download available on CSDB
2
38
1,733
A brand new release has landed!
Zak Mackren returns to the C64 with fresh graphics, great music, and that classic adventure feel.📥
Download the .PRG directly from CSDB:
csdb.dk/release/?id=90364
Run it on real hardware or in your emulator and enjoy!
 Commodore Computer Museum 🕹
Commodore Computer Museum 🕹
8
78
2,201

Mar 27
☆広報誌『CSDB』71号完成☆
当局HPで広報誌を公開中!
今回の表紙は、令和7年度日米交流事業「日米交流合同コンサート」♪
その他にも防衛局の魅力がたっぷりです!
ぜひご覧ください!!
リンクはこちら👇
mod.go.jp/rdb/chushi/pr/publ…
#防衛省 #自衛隊 #技官 #事務官
13
772

Mar 18
本当にお茶割り危機一髪なことが起きたのに、砂漠をジープで爆走したわけじゃないからと言って筆を置いたリスナー
#231 ENTPとCSDB | ヤマトパンクス
#銀河巡礼概論 #GERAラジオ
link.gera.fan/episode/07lpUs…
2
195
Feb 21
日本におけるESD後の遅発性出血予防の技術的進歩とPuraStatの立ち位置
Endoscopy誌論文、editorialからの考察
以前ご紹介しましたEndoscopyの論文では、
欧州10施設3142例で大腸ESD後CSDB(臨床的に重要な遅発性出血)に対する予防的クリップ完全閉鎖は有意差なしでした。
しかし、editorial(斎藤豊先生)は「閉鎖の密度/質」を指摘。現在の日本方式は糸+多数クリップで隙間なく封じる「高密度閉鎖」に進歩しており、同じ閉鎖でも別物である点を指摘されました。全例はコスト/時間/環境負荷的に非現実→個別化とも述べられています。
ここからが私の意見ですが、確かに日本式の高密度閉鎖でPuraStatの適応は変化するかもしれませんが、PuraStatは閉鎖の代替ではなく、oozing止血/閉鎖困難例の補完/レスキュー/組織修復という実装上の価値で、すでに有用性が認識されています。
本論文
thieme-connect.de/products/e…
Editorial
doi.org//10.1055/a-2773-4370
#3Dマトリックス
#RADA16
#PuraStat

1
22
2,387

🎶Blue Monday by New Order on the Commodore 64 👍Turn it up! It will transport you back to 1983!
Just discovered this absolute gem on CSDb: "Blue Monday [2025]" – a mind-blowing C64 chiptune cover of New Order's classic!
Nordischsound (of Hokuto Force, PET SCIIENTISTS, and more) poured his SID mastery into this, hitting us 40 years late but right on time! That throbbing bass, killer drums, and synths? MAGIC!!!!
The more you listen the better it gets 10/10 from me. Download from CSDB and try it on your C64, TheC64 or Commodore 64 Ultimate today.
4
33
285
10,355
Jan 18
When good haemostatic tools fail: lessons from delayed bleeding after EMR and ESD (1/2)
The prevention of delayed bleeding after advanced colorectal endoscopic resection represents a complex clinical challenge that appears resistant to single-modality prophylactic strategies.
1. The Limits of Mechanical Closure (De Cristofaro et al.)
In the largest Western multicentre study to date, De Cristofaro et al. evaluated the impact of complete prophylactic clip closure after colorectal endoscopic submucosal dissection (ESD) using a robust propensity score–matched design based on validated Limoges Bleeding Score (LBS) risk factors. Despite analysing more than 3,000 ESD cases and 944 matched pairs, complete defect closure did not significantly reduce clinically significant delayed bleeding (CSDB), even among patients receiving antithrombotic therapy or those classified as high risk (LBS 5–8). Importantly, this lack of benefit persisted despite closure being a deep, mechanically intuitive intervention and despite meticulous adjustment for known bleeding predictors.
2. Reinterpreting the PURPLE Trial
These findings have important implications for the interpretation of subsequent prophylactic haemostasis studies. In this context, the negative results of the PURPLE trial, which evaluated prophylactic application of a self-assembling peptide hydrogel (PuraStat) after EMR, should not be viewed as evidence of failure of the agent itself. Rather, when considered alongside De Cristofaro et al., PURPLE reinforces the concept that delayed bleeding is a multifactorial, time-dependent phenomenon that is unlikely to be prevented by a single local intervention, whether mechanical (clip closure) or topical (hydrogel application). The absence of benefit observed when PuraStat was applied as a stand-alone prophylactic measure after EMR is therefore pathophysiologically coherent, rather than contradictory, given that even complete closure of large ESD defects does not confer consistent protection.
3. Caution with Retrospective Data (Barone et al.)
Similarly, the multicentre retrospective case-control study by Barone et al., which reported a higher rate of delayed bleeding associated with self-assembling peptide gel use after EMR of large non-pedunculated lesions not amenable to closure, must be interpreted with caution. This study inherently selected a highly enriched high-risk population in whom the decision to apply the gel likely reflected unmeasured intraprocedural factors such as extent of thermal injury, presence of high-risk exposed vessels, operator concern, or centre-specific haemostatic practice. In such a setting, confounding by indication is highly probable, and the observed association cannot be taken as proof of causality or harm, particularly in light of small event numbers and wide confidence intervals.
4. The Value of Multimodal Strategy (POPS Trial)
In contrast, data from the POPS trial, a large multicentre prospective observational study evaluating PuraStat during high-risk tissue resection (HRTR) across both EMR and ESD, provide important real-world context. In POPS, PuraStat was frequently used as an adjunct to conventional haemostatic techniques, including targeted coagulation and focal clipping, rather than as an isolated prophylactic intervention. Within this multimodal haemostatic strategy, high intraprocedural haemostatic efficacy and a low overall delayed bleeding rate were observed. Although the absence of a control arm precludes causal inference, POPS supports the concept that the clinical value of self-assembling peptide hydrogels lies in their complementary role within layered haemostasis, rather than in replacement of deep vessel control.
More thoughts in the next post.
#3Dmatrix
#Endoscopy
#GIbleeding
#DelayedBleeding
#PURPLEtrial
#POPStrial
#PuraStat
#EMR
#ESD
#MultimodalHaemostasis
#EvidenceBasedMedicine
1
8
539
"Knight Rider: a shadowy flight into the dangerous world of a man who does not exist.
Michael Knight, a young loner on a crusade to champion the cause of the innocent, the helpless, the powerless, in a world of criminals who operate above the law." ... Sends chills down my spine just writing this, you can hear the music in your head and Richard Basehart's deep voice narrating it... pure gold.
Knight Rider was one of my favourite TV shows growing up, and what an intro, they don't make them like that anymore. :(
FUN FACT: Richard Basehart voiced the intro but did you know he also played Wilton Knight the dying billionaire founder of FLAG in the pilot episode! How cool is that.
When I heard TREX released a brand new Commodore 64 intro recreating the whole thing this month... I was instantly excited!!
Check out this beauty from January 12th on CSDb... this is pure 80s magic on the C64. What a time to be alive in the scene, 43 years later and it is just getting better and better. The whole SID tune is awesome but the ending is another level of awesomeness.
Who else was a fan of the Knight Rider series? I rank it in my top 5
1. MacGyver
2. Knight Rider
3. The A-Team
4. Magnum Pi
5. Miami Vice
A bit of a theme there LOL!
2
31
253
9,188

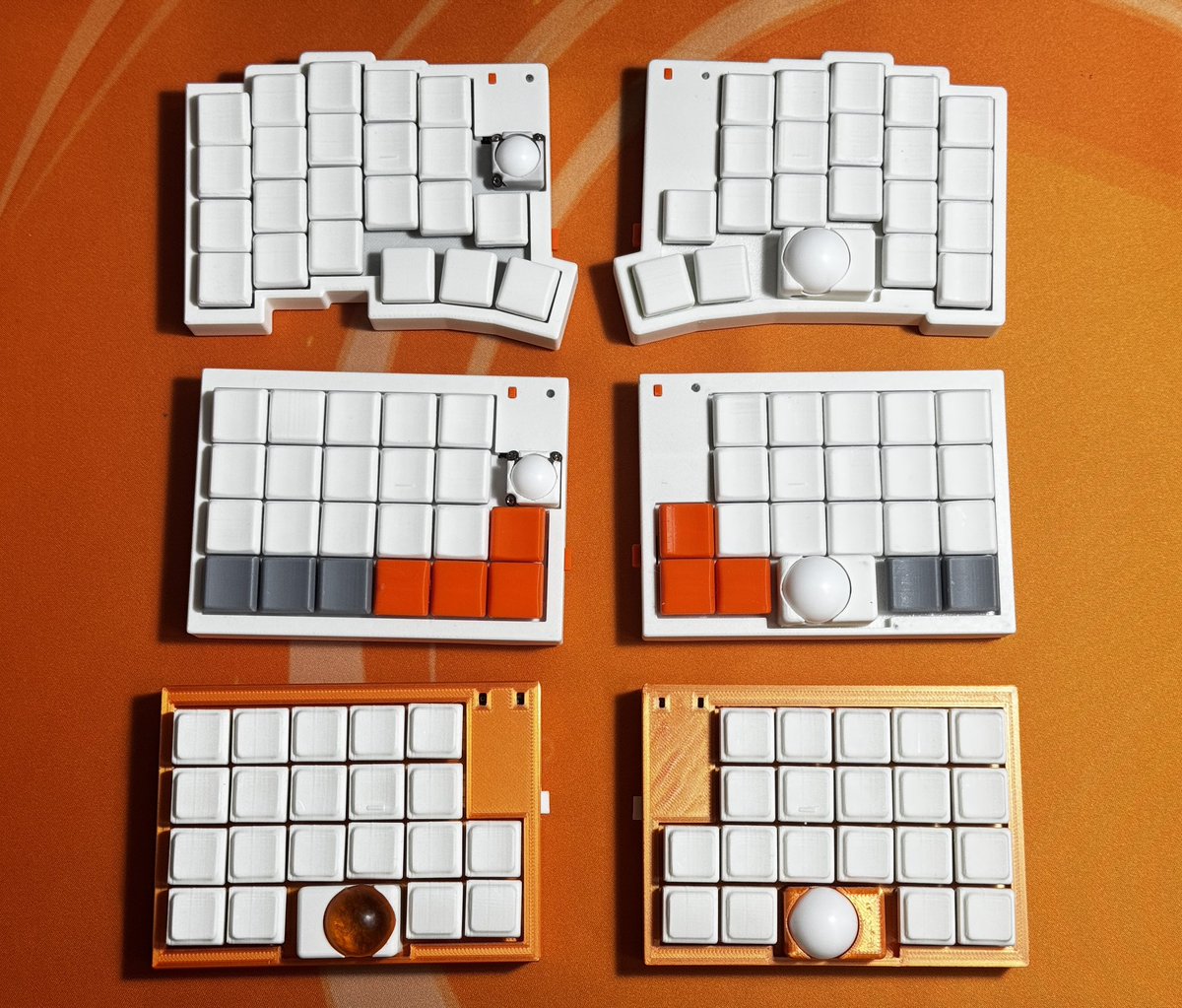
両手トラックボール党
Keyboard:
AroundForty CSDB
AroundForty DB
AroundForty TB
#KEEB_PD
#KEEB_PD_R283
#AroundForty_kbd
#自作キーボード
#トラックボール
4
71
2,766