
🎉📢 Check out our newly published systematic review and meta-analysis comparing over-the-scope clips (OTSC) versus standard endoscopic therapy as first-line treatment for bleeding peptic ulcer disease!
📄 Read the article: journals.lww.com/atm/pages/a…
@HazemAbosheaish @Eldesouki_mo
#GITwitter #Endoscopy #GIBleeding #MedTwitter
1
2
13
1,944

📢 #EditorsPick of the Month!
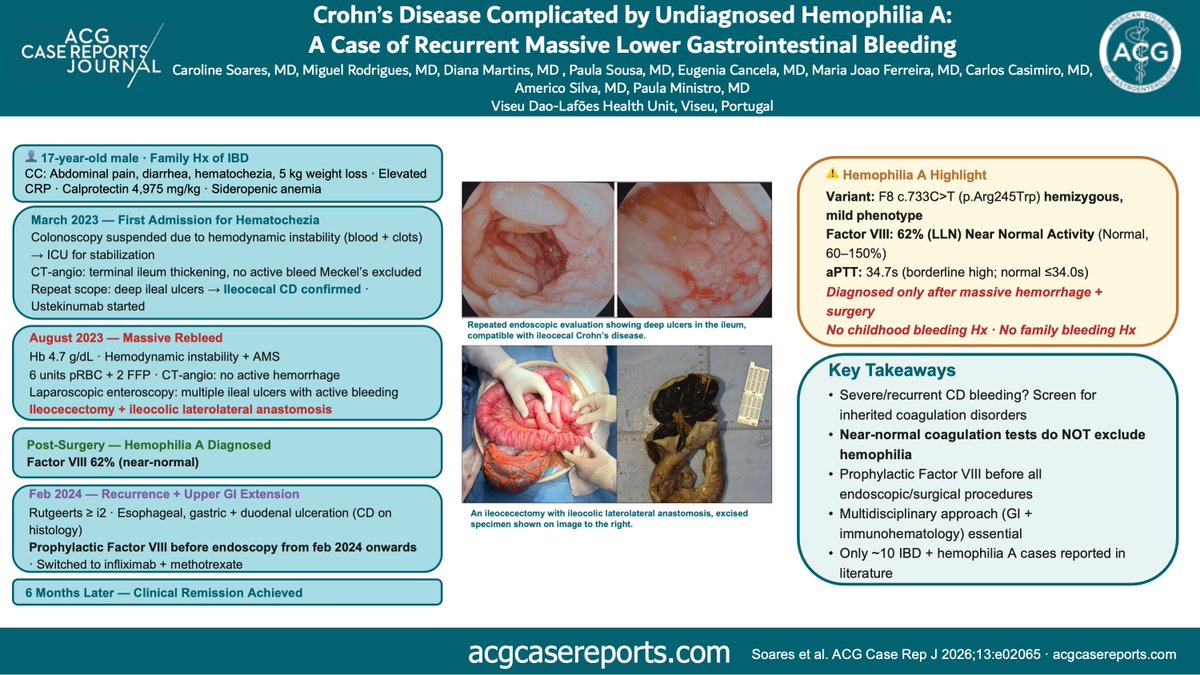
🩸A 17-year-old with ileal CD experienced 2 episodes of massive #GIBleeding requiring surgery, unveiling Hemophilia A diagnosis.
🧬Despite near-normal Factor VIII activity, the genetic variant carried real clinical impact!
🔗tinyurl.com/3h9zdzd3
1
11
15
1,404

May 27
GIE issue 5, 2026
ASGE編集委員会が選んだ10の領域 2025年の内視鏡医療
giejournal.org/article/S0016…
Nonvariceal GI bleeding
しっかり選出。
AI、ESD、GLP-1、GERDなどが話題を席巻する中で、GI内視鏡で消化管出血の管理・後出血予防・局所止血は、もう話題になりずらいのかな?なんて感じていませんか?
そんなことはありませんよ。確実に内視鏡医療の中核であり続けています。
「新しい話題」ではなく、「解決しきれていない課題」だから残り続けるんですね。 つまりPuraStatも。
それがこの領域の本質です。 PuraStatの論文も参照されていますよ。
#3Dmatrix #PuraStat #GIbleeding
12
708

May 11
Tranexamic acid in GI bleeding: useful tool, or time to rethink? 🩸💊🤔
BSG & ACPGBI position statement in @FrontGastro_BMJ sets out guidance on tranexamic acid in upper and lower gastrointestinal bleeding — a key topic for acute GI, surgical and emergency care teams. 🚑🔎
Essential reading for anyone managing GI haemorrhage.
Read more: fg.bmj.com/content/early/202…
#GIBleeding #TranexamicAcid #UpperGI #LowerGI #EmergencyMedicine #FrontlineGastro #GItwitter #Gastroenterology #Surgery #ClinicalGuidance @BritSocGastro @ACPGBI @my_UEG @AmCollegeGastro @DDWMeeting @ESGE_news @drkeithsiau @DrOmerAhmad @Dunnepdj @shraddha_gulati @CardiffGastro @DrBuHayee @poodocnisha @Sharm_Sub @PhilSmithIsBack @OTavabie @dr_aditi_kumar @TrevorTabone @eathar_s @IrenePerezMD @KGananandan @zare_benjamin @medicalreg @dtleiberman
1
21
56
4,947

Apr 30
During evaluation of obscure overt GI bleeding in an elderly lady, anterograde enteroscopy revealed a rare culprit deep in the jejunum — Jejunal Dieulafoy’s lesion.
Extremely rare, but potentially life-threatening if missed.
#Gastroenterology #GIBleeding #Dieulafoy #SmallBowel
2
105

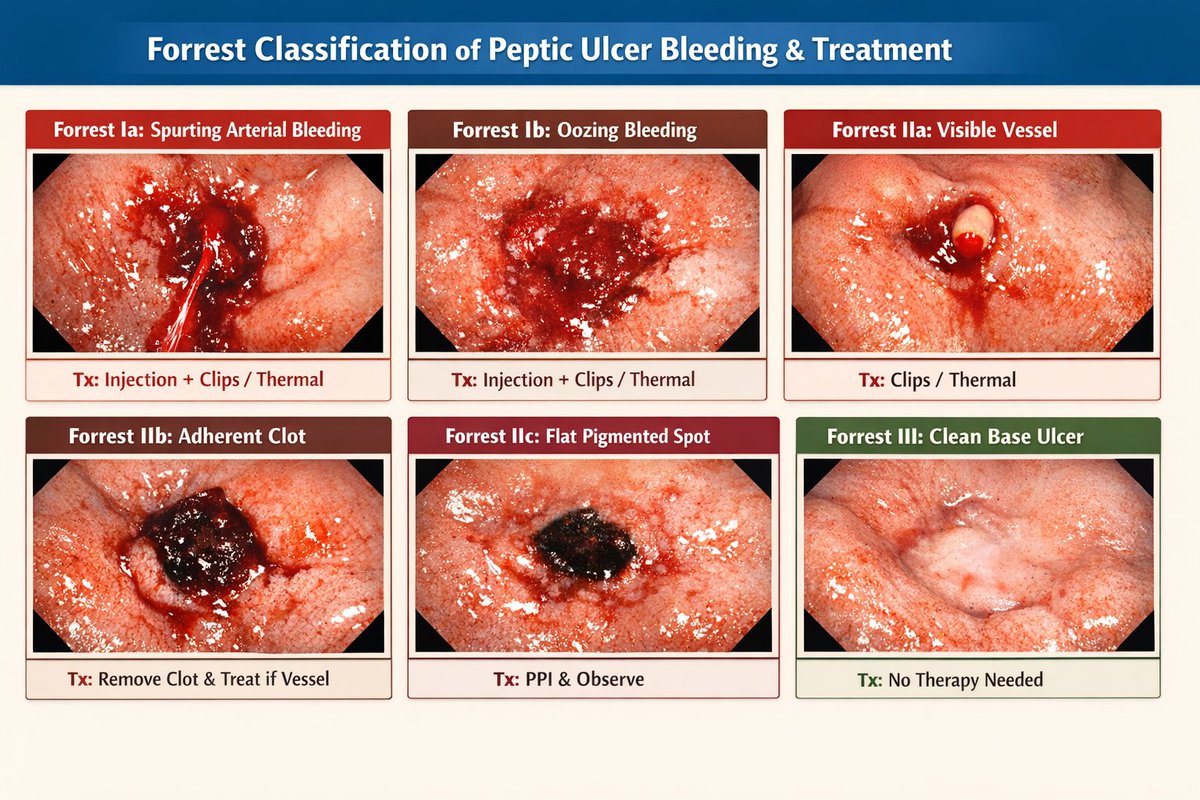
Peptic ulcer disease endoscopic appearance and the respective treatment according to forest classification.
#UpperGIBleed #GIBleeding #Gastroenterology #EmergencyMedicine #AcuteCare #CriticalCare
1
14
573

The correct answer is B. Melena ✅✅✅that classic black, tarry, foul-smelling stool from digested blood, usually signaling an upper GI bleed (think peptic ulcers, gastritis, or esophageal varices).
Quick clinical pearl for the ladies: In women, always keep heavy menstrual bleeding or endometriosis-related GI symptoms on the differential too as sometimes "blood in stool" reports can be confused with severe period flow. When in doubt then full history, heme occult test and GI referral if needed.
Thanks for the daily med ed 💙 #MedTwitter #WomensHealth #GIbleeding
432

🩸 Iron Deficiency in Males vs Females – Definition & DD 🔬✨
🧪 1️⃣ Definition (Laboratory-Based)
🟢 Low Ferritin = cornerstone
•⬇️ Ferritin <30 ng/mL → iron deficiency (ID)
•⬇️ Ferritin <15 ng/mL → diagnostic (WHO classic)
•🔥 If inflammation → ferritin <100 ng/mL TSAT <20% suggests ID
🟡 Transferrin Saturation (TSAT)
•⬇️ TSAT <20% = iron deficiency
•⬇️ TSAT <10% → severe deficiency
🔵 CBC Pattern
•⬇️ Hb
•⬇️ MCV (microcytosis)
•⬇️ MCH
•⬆️ RDW (early marker)
⸻
👩 Females (Premenopausal)
🎯 Most Common Cause:
🩸 Menstrual blood loss
DD in Females
1️⃣ Heavy menstrual bleeding (HMB)
2️⃣ Postpartum
3️⃣ Pregnancy (↑ iron demand)
4️⃣ Uterine fibroids
5️⃣ Endometriosis
6️⃣ GI loss (must not ignore!)
7️⃣ Malabsorption (celiac, bariatric)
⚠️ Always assess:
•Menstrual pattern
•Parity
•Dietary intake
⸻
👨 Males (Adult)
🚨 Iron deficiency in adult males = GI blood loss until proven otherwise
DD in Males
1️⃣ Colorectal cancer
2️⃣ Gastric cancer
3️⃣ Peptic ulcer disease
4️⃣ Angiodysplasia
5️⃣ IBD
6️⃣ Celiac disease
7️⃣ NSAID gastropathy
8️⃣ Hookworm (endemic areas)
🔴 Rule:
👉 IDA in adult male = bidirectional endoscopy unless proven otherwise
⸻
🧬 Both Sexes – Shared DD
•Chronic GI bleeding
•Blood donation
•Hematuria
•Pulmonary hemosiderosis
•Malabsorption syndromes
•Chronic kidney disease (functional ID)
⸻
⚖️ Iron Deficiency vs Iron Deficiency Anemia (IDA)
🧪 ID = low iron stores (may have normal Hb)
🩸 IDA = low iron anemia
Early stage:
✔ Ferritin ↓
✔ Hb normal
Late stage:
✔ Microcytic anemia
⸻
🔍 Key Distinction in Practice
👩 Young woman heavy menses → gynecologic first
👨 Adult male → GI malignancy exclusion mandatory
⸻
🚨 Red Flags (Any Sex)
•Weight loss
•Age >50
•Family hx CRC
•Change in bowel habits
•Refractory to oral iron
⸻
💡 Clinical Pearl
Iron deficiency is a diagnosis, not a final answer.
Always identify the source of loss.
#IronDeficiency #Anemia #Hematology #GIbleeding #MedTwitter #HemePearls
2
47
153
7,883
Jan 23
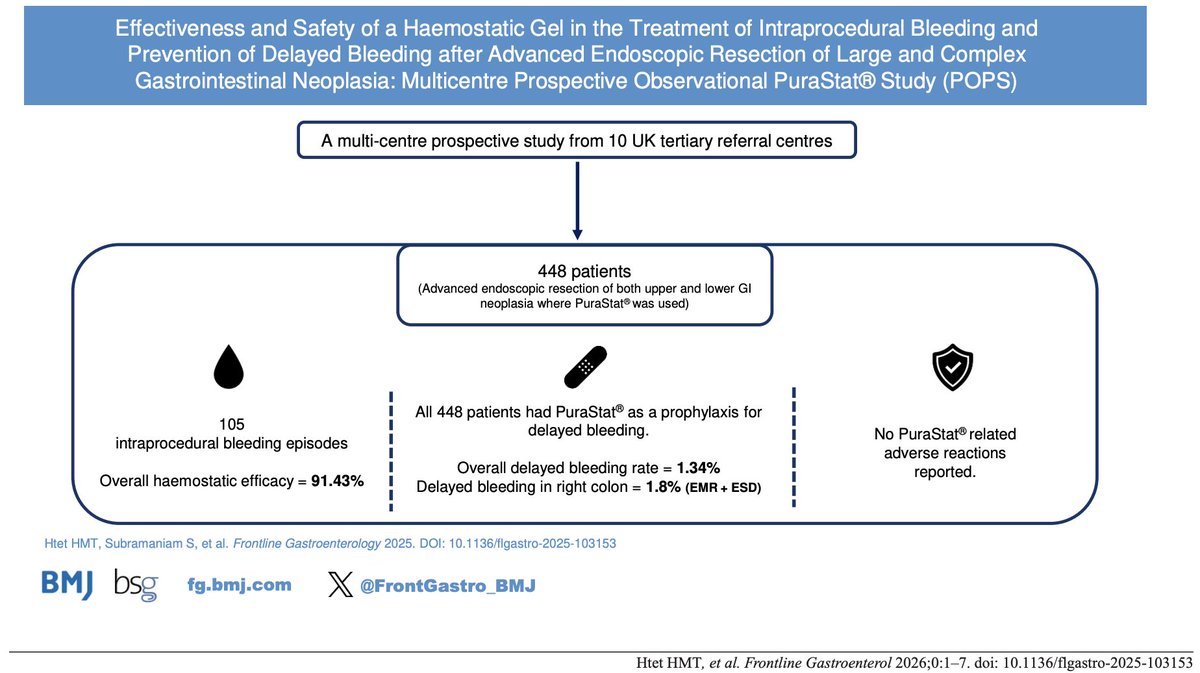
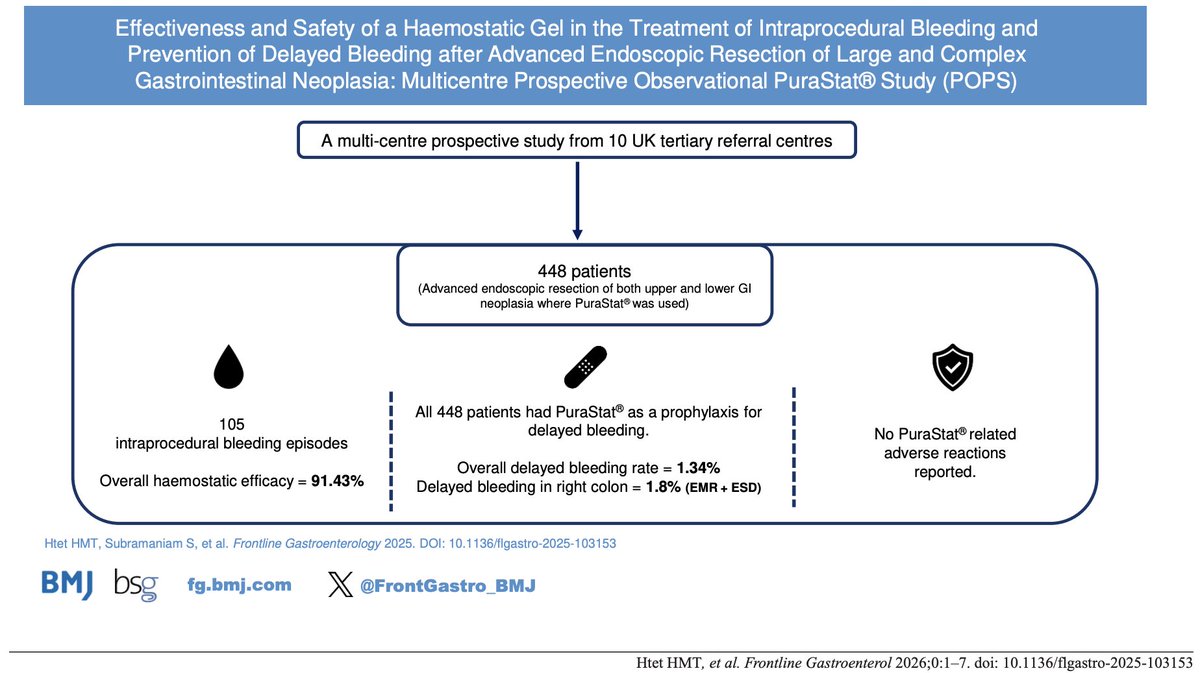
🪧 📢 We are delighted to announce that the findings of the PuraStat study have just been published in FG! 🔥
👨👨👧👧 Multi-centre prospective study
🏥 448 high-risk tissue resections (HRTR) - including EMR and ESD in the upper and lower GI tract, with all patients receiving prophylactic PuraStat to prevent delayed bleeding
⏰ The rate of delayed bleeding across the full cohort was 1.34%
🩸 Of 195 patients with intra-procedural bleeding, haemostatic efficacy was 91.43%
On subgroup analysis, the authors found that this was highest in the duodenum (8.69%) followed by 1.80% in the right colon (EMR and ESD). There were no delayed bleeds in the oesophagus, stomach and left colon.
Congratulations to Dr Hein Myat Thu Htet and co-authors!
@Hein_Gastro @Sharm_Sub @AParraBlanco @NorikoSuzuki3 @HajiAmyn @massi_dipietro @MariettaIacucci @iosifbeintaris @ayjas @TheRealFergusTP @SebastianZeki @gi_jasondunn @gastro3570
fg.bmj.com/content/early/202…
@drkeithsiau @DrOmerAhmad @Dunnepdj @shraddha_gulati @CardiffGastro @DrBuHayee @poodocnisha @Sharm_Sub @PhilSmithIsBack @OTavabie @dr_aditi_kumar @TrevorTabone @eathar_s @IrenePerezMD @KGananandan @zare_benjamin @medicalreg @dtleiberman
#Endoscopy #GIEndoscopy #DigestiveHealth #Gastroenterology #EndoscopyLife #EndoscopyEducation #EndoscopyTraining #ThirdSpaceEndoscopy #AdvancedEndoscopy #InterventionalEndoscopy #POEM #ESD #STER #EndoscopicInnovation #SubmucosalEndoscopy #GIBleeding #UpperGIBleed #LowerGIBleed #AcuteGIBleed #EndoscopicHemostasis #GIHemorrhage #BleedingControl
5
7
857
Jan 18
When good haemostatic tools fail: lessons from delayed bleeding after EMR and ESD (2/2)
Conclusion
Taken together, the collective evidence from these four studies converges on a consistent conclusion: delayed bleeding after advanced colorectal resection is unlikely to be reliably prevented by any single local measure, including complete mechanical closure. Accordingly, negative or unfavourable outcomes observed when self-assembling peptide gels are used in isolation (as in the PURPLE trial or selected high-risk retrospective EMR cohorts) should not be extrapolated to dismiss their potential utility when integrated into a multimodal haemostatic strategy. Future research should therefore prioritise risk-stratified, prospective comparative studies that evaluate adjunctive PuraStat use within predefined haemostatic protocols, reflecting contemporary endoscopic practice and the multifactorial nature of delayed bleeding.
⸻
References (all four)
1.De Cristofaro E, Jacques J, Montori S, et al.; FECCo Working Group.
Impact of prophylactic clipping on delayed bleeding after colorectal endoscopic submucosal dissection: a multicenter propensity score-matched study.
Endoscopy. 2026. doi: 10.1055/a-2723-5162.
2.Drews J, Zachäus M, Kleemann T, et al.
Multicentre randomised controlled trial of a self-assembling haemostatic gel to prevent delayed bleeding following endoscopic mucosal resection (PURPLE trial).
Gut. 2025;74:1103–1111.
3.Barone VR, Ma M, Inamdar S, et al.
Use of a novel self-assembling peptide gel for prevention of bleeding after endoscopic mucosal resection of large non-pedunculated sessile colorectal polyps: a case-control study.
Journal Pre-proof.
4.Htet HMT, Subramaniam S, Parra-Blanco A, et al.; POPS Trial Investigators.
Effectiveness and safety of a haemostatic gel in the treatment of intraprocedural bleeding and prevention of delayed bleeding after advanced endoscopic resection of large and complex gastrointestinal neoplasia : a multicentre prospective observational PuraStat study(POPS trial).
Frontline Gastroenterology. 2025. doi: 10.1136/flgastro-2025-103153.
#3Dmatrix
#Endoscopy
#GIbleeding
#DelayedBleeding
#PURPLEtrial
#POPStrial
#PuraStat
#EMR
#ESD
#MultimodalHaemostasis
#EvidenceBasedMedicine
9
489
Jan 18
When good haemostatic tools fail: lessons from delayed bleeding after EMR and ESD (1/2)
The prevention of delayed bleeding after advanced colorectal endoscopic resection represents a complex clinical challenge that appears resistant to single-modality prophylactic strategies.
1. The Limits of Mechanical Closure (De Cristofaro et al.)
In the largest Western multicentre study to date, De Cristofaro et al. evaluated the impact of complete prophylactic clip closure after colorectal endoscopic submucosal dissection (ESD) using a robust propensity score–matched design based on validated Limoges Bleeding Score (LBS) risk factors. Despite analysing more than 3,000 ESD cases and 944 matched pairs, complete defect closure did not significantly reduce clinically significant delayed bleeding (CSDB), even among patients receiving antithrombotic therapy or those classified as high risk (LBS 5–8). Importantly, this lack of benefit persisted despite closure being a deep, mechanically intuitive intervention and despite meticulous adjustment for known bleeding predictors.
2. Reinterpreting the PURPLE Trial
These findings have important implications for the interpretation of subsequent prophylactic haemostasis studies. In this context, the negative results of the PURPLE trial, which evaluated prophylactic application of a self-assembling peptide hydrogel (PuraStat) after EMR, should not be viewed as evidence of failure of the agent itself. Rather, when considered alongside De Cristofaro et al., PURPLE reinforces the concept that delayed bleeding is a multifactorial, time-dependent phenomenon that is unlikely to be prevented by a single local intervention, whether mechanical (clip closure) or topical (hydrogel application). The absence of benefit observed when PuraStat was applied as a stand-alone prophylactic measure after EMR is therefore pathophysiologically coherent, rather than contradictory, given that even complete closure of large ESD defects does not confer consistent protection.
3. Caution with Retrospective Data (Barone et al.)
Similarly, the multicentre retrospective case-control study by Barone et al., which reported a higher rate of delayed bleeding associated with self-assembling peptide gel use after EMR of large non-pedunculated lesions not amenable to closure, must be interpreted with caution. This study inherently selected a highly enriched high-risk population in whom the decision to apply the gel likely reflected unmeasured intraprocedural factors such as extent of thermal injury, presence of high-risk exposed vessels, operator concern, or centre-specific haemostatic practice. In such a setting, confounding by indication is highly probable, and the observed association cannot be taken as proof of causality or harm, particularly in light of small event numbers and wide confidence intervals.
4. The Value of Multimodal Strategy (POPS Trial)
In contrast, data from the POPS trial, a large multicentre prospective observational study evaluating PuraStat during high-risk tissue resection (HRTR) across both EMR and ESD, provide important real-world context. In POPS, PuraStat was frequently used as an adjunct to conventional haemostatic techniques, including targeted coagulation and focal clipping, rather than as an isolated prophylactic intervention. Within this multimodal haemostatic strategy, high intraprocedural haemostatic efficacy and a low overall delayed bleeding rate were observed. Although the absence of a control arm precludes causal inference, POPS supports the concept that the clinical value of self-assembling peptide hydrogels lies in their complementary role within layered haemostasis, rather than in replacement of deep vessel control.
More thoughts in the next post.
#3Dmatrix
#Endoscopy
#GIbleeding
#DelayedBleeding
#PURPLEtrial
#POPStrial
#PuraStat
#EMR
#ESD
#MultimodalHaemostasis
#EvidenceBasedMedicine
1
8
539
Jan 18
🪧 📢 We are delighted to announce that the findings of the PuraStat study have just been published in FG! 🔥
👨👨👧👧 Multi-centre prospective study
🏥 448 high-risk tissue resections (HRTR) - including EMR and ESD in the upper and lower GI tract, with all patients receiving prophylactic PuraStat to prevent delayed bleeding
⏰ The rate of delayed bleeding across the full cohort was 1.34%
🩸 Of 195 patients with intra-procedural bleeding, haemostatic efficacy was 91.43%
Congratulations to Dr Hein Myat Thu Htet and co-authors! @Hein_Gastro @Sharm_Sub @AParraBlanco @NorikoSuzuki3 @HajiAmyn @massi_dipietro @MariettaIacucci @iosifbeintaris @ayjas @TheRealFergusTP @SebastianZeki @gi_jasondunn @gastro3570
fg.bmj.com/content/early/202…
@drkeithsiau @DrOmerAhmad @Dunnepdj @shraddha_gulati @CardiffGastro @DrBuHayee @poodocnisha @Sharm_Sub @PhilSmithIsBack @OTavabie @dr_aditi_kumar @TrevorTabone @eathar_s @IrenePerezMD @KGananandan @zare_benjamin @medicalreg @dtleiberman
#Endoscopy #GIEndoscopy #DigestiveHealth #Gastroenterology #EndoscopyLife #EndoscopyEducation #EndoscopyTraining #ThirdSpaceEndoscopy #AdvancedEndoscopy #InterventionalEndoscopy #POEM #ESD #STER #EndoscopicInnovation #SubmucosalEndoscopy #GIBleeding #UpperGIBleed #LowerGIBleed #AcuteGIBleed #EndoscopicHemostasis #GIHemorrhage #BleedingControl
2
14
29
2,555

24 Dec 2025
What is your go-to technique for inflation of a Minnesota or Blakemore Tube? In this latest EM:RAP procedure video, Jess Mason adds two more options to your toolbox and shares a pitfall you might have run into in the past as well.
Solution-oriented and always learning are the hallmarks of an incredible ER physician. Join EM:RAP today and be part of the greatest community in emergency medicine. We’ve got a great year of learning planned for 2026, and we don’t want you to miss a minute.
Check out the full video on the EM:RAP app today: emrap.org/episode/twowaysto/…
#minnesotatube #GIbleeding #emergencymedicine #MedED #blakemoretube #EMRAP
1
2
164

28 Nov 2025
💉 When should we scope — and when can we feed?
Congrats to @mmns_obeidat on his PhD on instability & refeeding in GI bleeding.
▶️ youtube.com/watch?v=gbY-7r6A…
#GIBleeding #Endoscopy #TranslationalMedicine #PhDDefence
1
2
194

19 Nov 2025
పొట్టకి క్లిప్స్ పెడతారా 😳😳..!
👨⚕️⚕️ Meet Dr. Vikranth Chunduri – Expert Gastroenterologist & Hepatologist
#hemoclips #endoscopy #endoscopysurgeon #gastroenterology #endoscopyskills #gibleeding #DRVikranthChunduri #Mithramedicarehospital
1
4
224
6 Nov 2025
悲報
出ました。GIE誌
Best of Esophagogastroduodenoscopy 2025
Edward Villa, MD
(Elsevier / ASGE)
giejournal.org/article/S0016…
(アブストラクトなし、リファレンスのみ)
---
止血に関する要旨
2025年も「内視鏡止血治療の進化」が注目。(ですよね。)
非静脈瘤性上部消化管出血(NVUGIB)では、従来の止血法(クリップ・熱凝固・注入)の限界を補う新ツールとしてhemostatic powder(止血パウダー) が急速に普及。(パウダー?)
---
紹介された製剤
(1) Hemospray (TC-325, Cook Medical, USA)
(2) CEGP-003 (CG Gel, CGBio, Korea)
あれ? マジパウダーだけですか??
しかも CGBio(韓国承認のみ)って初耳。
PuraStat(3-D Matrix) は記載なし。🥺🤦
---
PuraStatが掲載されなかった理由 (推測)
① 著者が“止血剤=パウダー”と分類している
② 2025年時点で RADA16 の大規模RCTやメタ解析が存在しない
---
憤慨しても仕方ありませんが、
「 POPS 論文どうなってるの?」って言いましたよね。岡田社長。
#3Dマトリックス
#Endoscopy #Hemostasis #GIbleeding #GIEjournal
#Hemospray #CGBio #PuraStat #RADA16 #Gastroenterology
#ClinicalResearch #BestOfEGD2025
12
440
29 Oct 2025
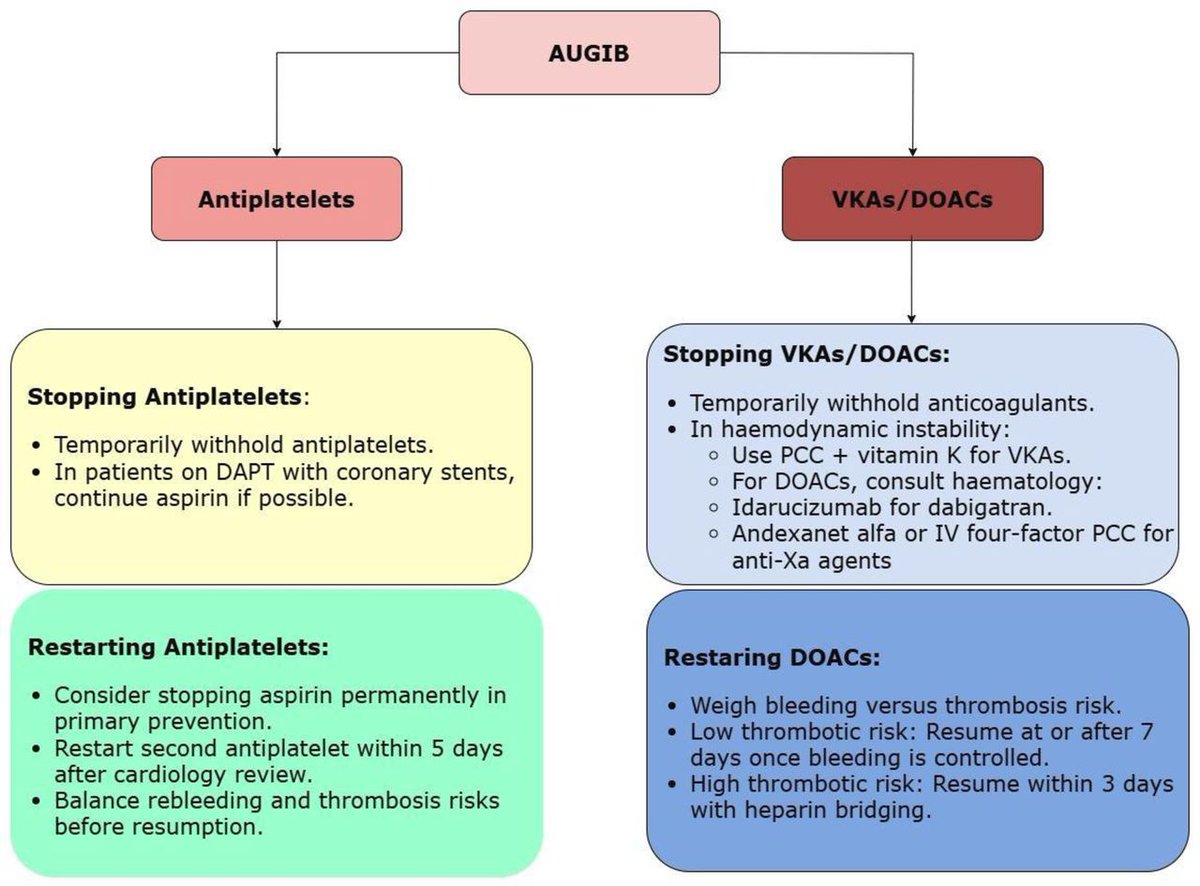
Are you confident your UGIB pathway reflects the latest evidence?
This concise FG review highlights what’s changed — and what must change.
🔓 fg.bmj.com/content/early/202…
@iangralnek @@drkeithsiau amongst co-authors!
@PhilSmithIsBack @OTavabie @dr_aditi_kumar @TrevorTabone @eathar_s @IrenePerezMD @KGananandan @zare_benjamin @medicalreg @dtleiberman @BASLedu @BSGtrainees @WorldGastroOrg @ulstergastro @SEEDendoscopia @EASLedu @AmCollegeGastro @Aegastro @SAGES_updates @UHSEndoscopy @WAGE_media @ESGE_news @EndoCollabcom @AmerGastroAssn @ASGEendoscopy @my_ueg
#UGIB #GIbleeding #Endoscopy #GastroTwitter #MedTwitter #FGJournal
#AcuteCare #GIemergency #Haemostasis #EvidenceBasedMedicine
2
13
34
3,089

4 Oct 2025
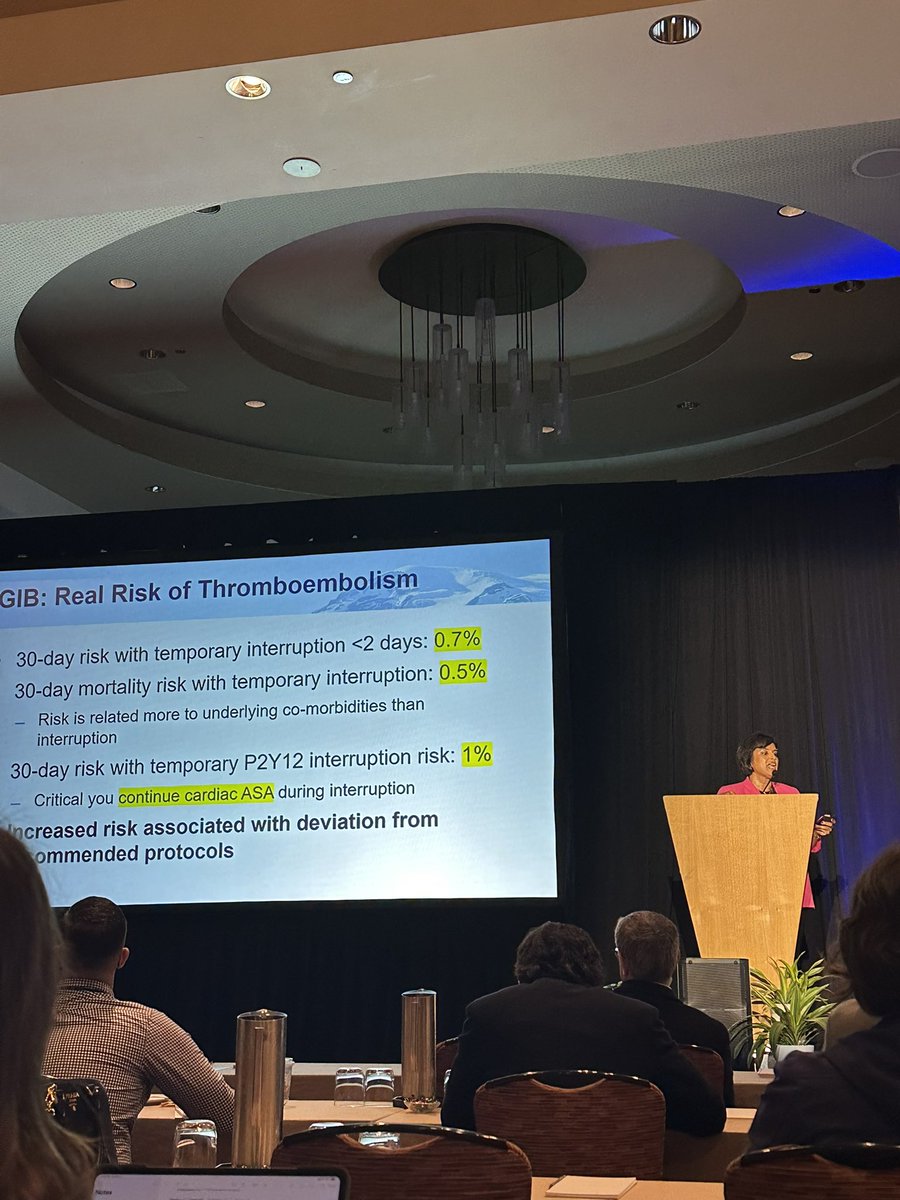
All you need to know about #CardioGI ❤️💩🩸
Amazing talk by @NeenaSAbrahamMD !
✅ Dont stop #ASA for any procedures
✅ Use reversal in very select cases
✅ TEG is not helpful in #GIBleeding
✅ PCC >>> FFP
#PacificNWGIUpdates

2
12
53
4,133

"Blood, Blood and More Blood" - Dr. @alan_barkun talk on GI bleeding in 2025 is not for the faint-hearted! 🩸 Game-changing tips incoming. #GIBleeding #RMIE2025

5
9
731

Portal Hypertension and GI Bleeding in Children can be life-threatening and complex to manage. How do we approach it with confidence?
Join Dr. Ashraf Alshafi at the Saudi Liver Meeting 2025 for an evidence-based, case-driven talk tailored to Pediatric Hepatology Board Review.
📅 Thursday | 16th October 2025
⏰ 13:20 – 13:50
📍 VOCO Hotel, Riyadh - Abha Meeting Room
📚 Pediatric Hepatology Board Review Course
🎓 8 CME Hours accredited
🔗 Register now: saslt.vax.solutions/
#SLM2025 #SASLT #GIbleeding #PortalHypertension #PediatricHepatology #CME

4
7
2,742