
PPFE終末期の医療 grok が盛んに 在宅療法での NPPV を勧めてくるのですが PEEP ≒ EPAP の設定自分でやるのでしょうか?
それともドクターが全部設定してくれるのでしょうか?
荷が重いです。
46

📖🇭🇳 Como parte de nuestro compromiso con la mejora continua, se llevó a cabo la capacitación “Atención al Ciudadano con Valor Público”, impartida por la EPAP, fortaleciendo las capacidades de los servidores públicos para brindar una atención más cercana, eficiente y de calidad a la ciudadanía.
#ANSEC #EPAP #Capacitación #ServicioCivil #AtenciónCiudadana #Honduras




4
10
65
R retweeted
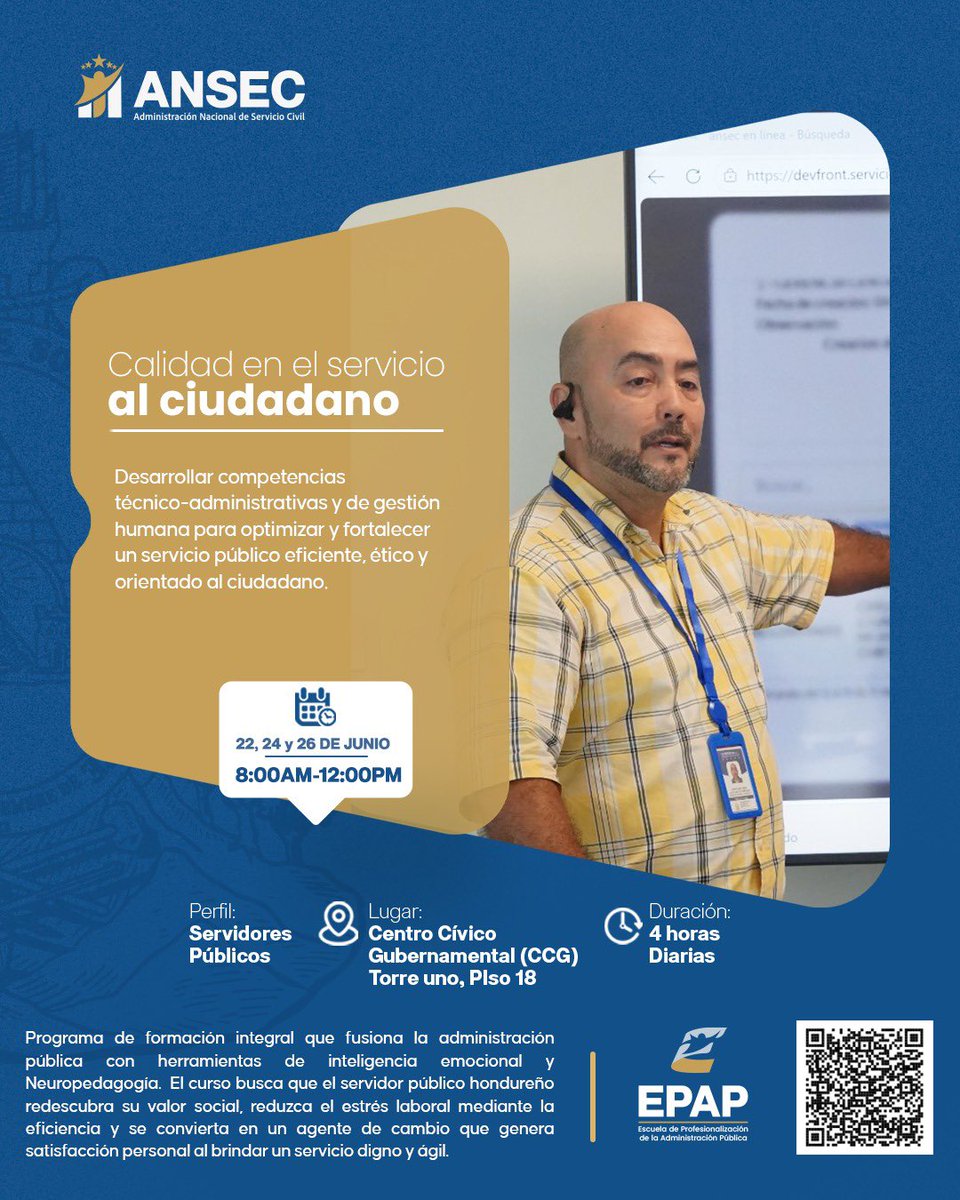
⭐ Servir mejor es construir un mejor Estado.
ANSEC (Administración nacional de Servicio Civil) y EPAP (Escuela de profesionalización de la Administración Publica) desarrollan la capacitación “Calidad en el Servicio al Ciudadano”, un espacio de formación que integra herramientas de inteligencia emocional y para fortalecer el desempeño de los servidores públicos hondureños.
#ANSEC #EPAP #CalidadEnElServicio #ServidoresPúblicos #FormaciónContinua
6
8
35
R retweeted
🎓 La profesionalización del servicio público sigue avanzando.
En conjunto con EPAP, ANSEC impulsa la capacitación “Modelos de Inducción Institucional”, una iniciativa que fortalece los procesos de incorporación y desarrollo de los servidores públicos para una gestión más efectiva y orientada a resultados.
#ANSEC #EPAP #Capacitación #GestiónPública #DesarrolloProfesional

5
12
72

Jun 16
Hi Ariel! That screen looks like a Servo-U to me, one of the ventilators we use in our ICU. The waveform display appears to show two manoeuvres used to assess inspiratory effort:
— End-inspiratory occlusion: Pplat close to 40 cmH₂O and an estimated PMI of approximately 4 cmH₂O.
— End-expiratory occlusion: ΔPocc close to 8 cmH₂O, corresponding to an estimated Pmus of approximately 6 cmH₂O, with the usual limitations of this method.
Taken together, these findings neither establish nor rule out readiness for extubation. The estimated Pmus suggests a moderate inspiratory effort under the current level of support. Neither finding would, by itself, preclude carefully monitored extubation if all other clinical criteria were met, but neither would be sufficient to justify proceeding.
An SBT performed while maintaining a PEEP of 28 cmH₂O would not be a conventional liberation trial and would not tell us how much effort the patient would generate without positive pressure. It would only show that the patient can breathe spontaneously while remaining substantially unloaded. However, if the plan were to extubate directly to NIV, I would not necessarily require the patient to tolerate complete withdrawal of positive pressure for a prolonged period.
I would assess respiratory rate, tidal volume expressed relative to predicted body weight, thoracoabdominal breathing pattern, accessory muscle use, dyspnoea, blood gases, haemodynamics, cough strength, secretion burden, and the ability to protect the airway. The fact that the patient can communicate in writing indicates that they are awake and cooperative, but it does not exclude increased work of breathing. I do not see enough information in the screenshot to conclude that the patient has overt respiratory distress; moreover, the effort shown here was assessed while the patient was receiving PEEP 28 cmH₂O and pressure support 6 cmH₂O.
If the patient otherwise met extubation criteria, I would favour extubation directly to NIV, given the morbid obesity and the high level of positive pressure currently required. Before extubation, I would briefly assess the response to substantially lower support and progressively reduce invasive PEEP to identify a level at which the patient maintains adequate oxygenation and ventilation without a clinically relevant increase in inspiratory effort or evidence of derecruitment. I would not necessarily require a prolonged zero-support or T-piece trial.
For post-extubation NIV, if previous effective home settings were available, I would use them as a reference rather than as a fixed prescription. If no previous settings were available, I would individualise EPAP according to the response observed during invasive PEEP reduction and after extubation, rather than automatically transferring the invasive PEEP level to the mask. I would increase EPAP if desaturation, evidence of derecruitment, upper-airway obstruction, or increased respiratory effort developed, and subsequently reduce it as the acute component resolved.
I would titrate pressure support according to inspiratory effort, respiratory rate, tidal volume, PaCO₂, pH, and patient–ventilator synchrony. If the patient genuinely required an expiratory pressure close to 28 cmH₂O to remain clinically stable, and this could not be delivered safely and effectively through NIV, I would reconsider whether the patient was ready for extubation.
57

Jun 16
PEEP for SBT : unsettled in obesity,28 avoids derectuitment,5/5 mimics post extubation load.
NIV ,HFNC ; can’t replicate PEEP 28.
EPAP : titrate to comfort likely ~10-12.
WOB unclear from waveform ; since he can write, his report beats it.
1
127
Cristian Vasquez retweeted

Jun 15
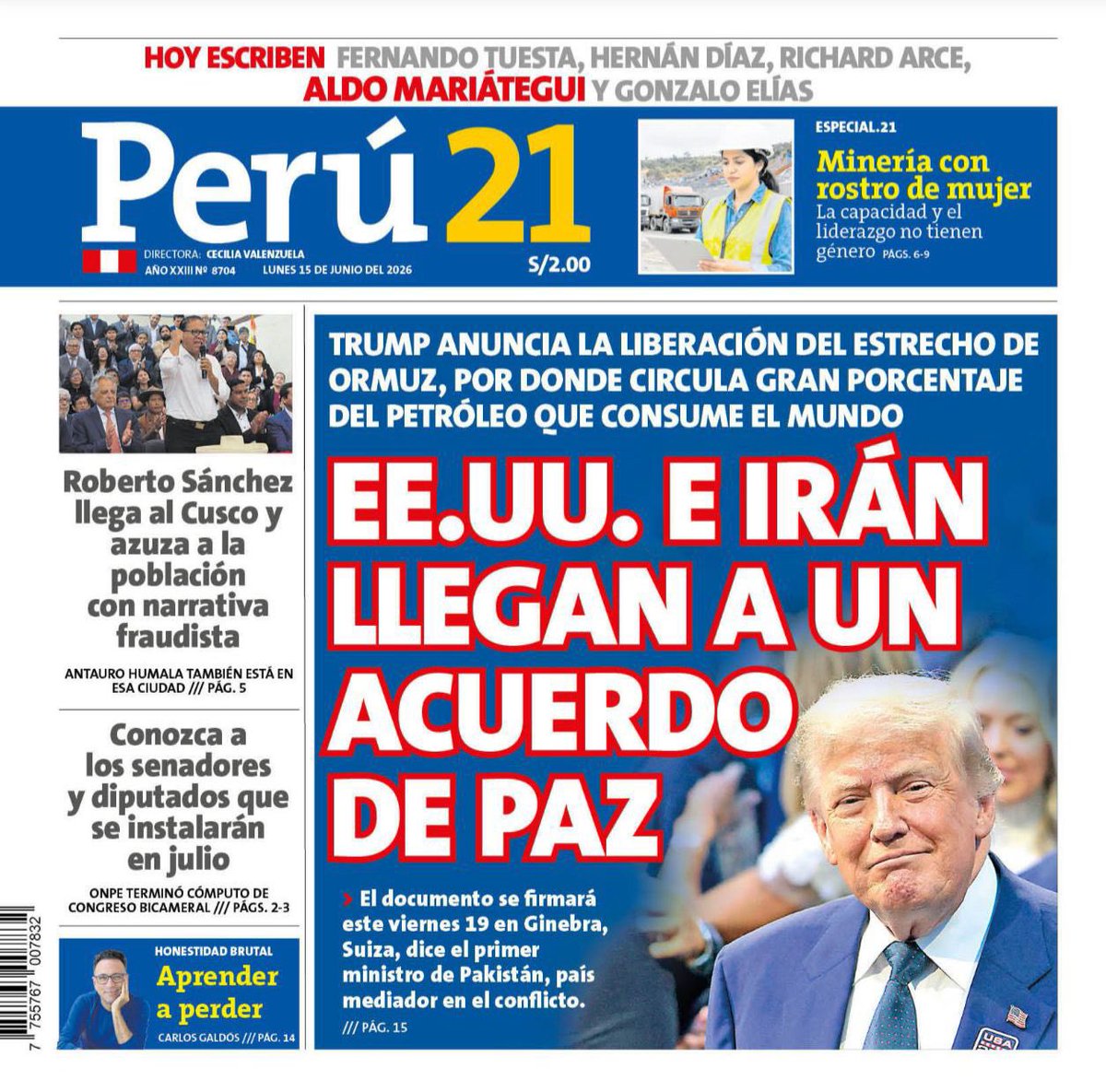
🗞 EE.UU. E IRÁN LLEGAN A UN ACUERDO DE PAZ
📲 Esta es la edición de hoy. Toda la información completa en nuestro ePaper: epaper.peru21.pe/promociones…
4
12
27
1,449

King’s jobs retweeted

We're inviting Expressions of Interest for senior postdoc and advanced fellowship applications to the EPAP group: inspirehep.net/jobs/3167731
1
1
202

Jun 15
The most common bilevel mistake: raising EPAP for oxygenation and leaving IPAP alone. IPAP − EPAP is the breath. Shrink the delta, shrink the ventilation. Full breakdown: @kindrespiratorycare stan.store/YirgiGeb
4