
Mar 8
🩺#EchoTips 11 principios básicos para hacer mejor un ultrasonido
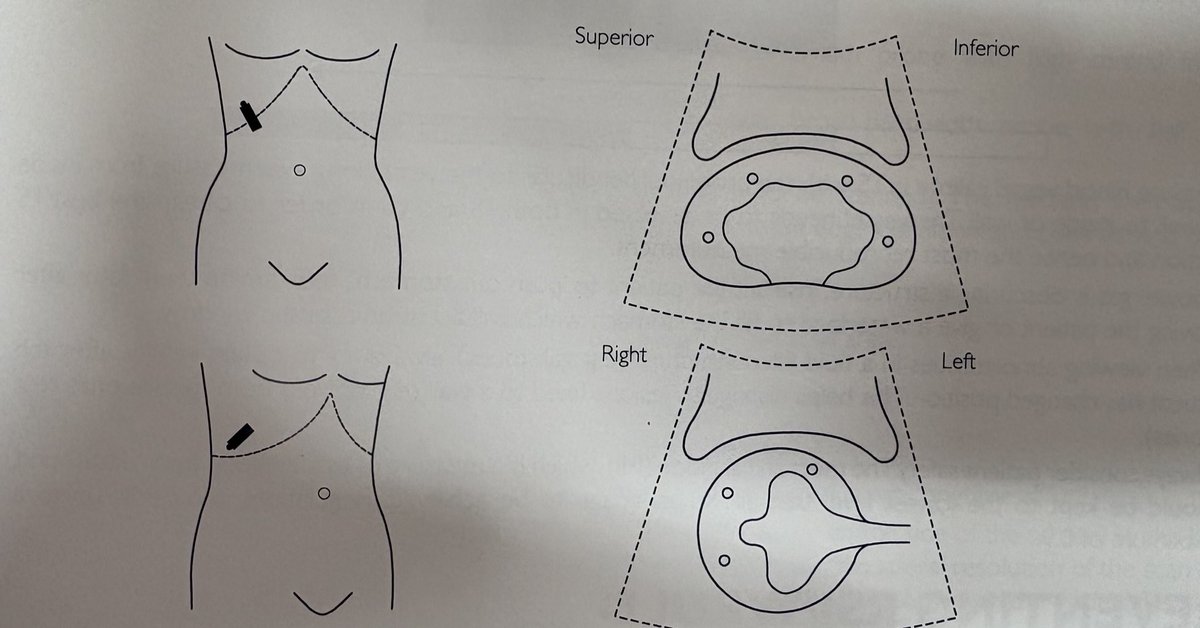
📍 1. Orientación correcta del transductor
• Plano longitudinal → marcador hacia la cabeza
• Plano transversal → marcador hacia la derecha del paciente
📌 Si la orientación es incorrecta, la anatomía se interpreta mal.
📍 2. Escanea completamente el órgano
No te quedes en un solo corte.
Explora a través y más allá del órgano para no perder patología periférica.
📍 3. Usa ventanas acústicas
Siempre que sea posible.
Ejemplos:
• Vejiga llena para pelvis
📍 4. Caracteriza lesiones quísticas
🟢 Benignas
• Bordes lisos
• Pared delgada
• Contenido anecoico
• Refuerzo acústico posterior
🔴 Sospecha de malignidad
• Bordes irregulares
• Pared gruesa
• ecos internos o septos
• mala transmisión acústica
• flujo Doppler interno
📍 5. Busca efecto de masa
Las lesiones malignas suelen distorsionar la arquitectura normal del órgano.
📍 6. Usa Doppler cuando tengas duda
Ayuda a diferenciar:
• vasos sanguíneos
• conductos
• estructuras sólidas
📍 7. Usa la mnemotecnia PLiSK
Para recordar la ecogenicidad normal:
Páncreas > Hígado > Bazo > Riñón
📍 8. Mide vasos correctamente
• Coloca el transductor perpendicular al eje largo
• Mide de pared interna a pared interna
• Evalúa en transversal y longitudinal
📍 9. Si el gas intestinal no deja ver…
Puedes:
• Cambiar la posición del paciente
• Repetir el estudio después
• Usar líquidos como ventana acústica
📍 10. Cambia la posición del paciente
Especialmente al evaluar estructuras con líquido (ej. vesícula).
Esto ayuda a distinguir:
• cálculos móviles
• pólipos
📍 11. Seguridad del paciente
Mantén el Mechanical Index (MI) lo más bajo posible que permita buena imagen.
📌 Regla general: ≤ 0.9
#POCUS #Ultrasonido #Ecografía #MedicinaDeUrgencias
1
40
165
5,321

📢 New cardiology research! 🫀✨
Check out this study exploring how echocardiographic measurement of inferior vena cava (IVC) diameter can help estimate central venous pressure in adult Fontan patients — a key step toward better monitoring and care in this complex congenital heart population.
📌 Highlights:
• Single-centre retrospective study of adult Fontan patients using transthoracic echo to measure IVC size.
• IVC diameter may serve as a non-invasive estimate of central venous pressure, with potential clinical utility in follow-up.
• Insights like this help improve hemodynamic assessment without invasive procedures. 🩺💡
💡 Important read for clinicians & imagers caring for Fontan patients and anyone interested in echo-based hemodynamic assessment! 📖❤️
#Cardiology #Echocardiography #Fontan #CentralVenousPressure #EchoTips #CardioTwitter #CongenitalHeartDisease #ClinicalResearch
doi.org/10.1093/ehjimp/qyaf0…

10
28
2,178

1 Oct 2025
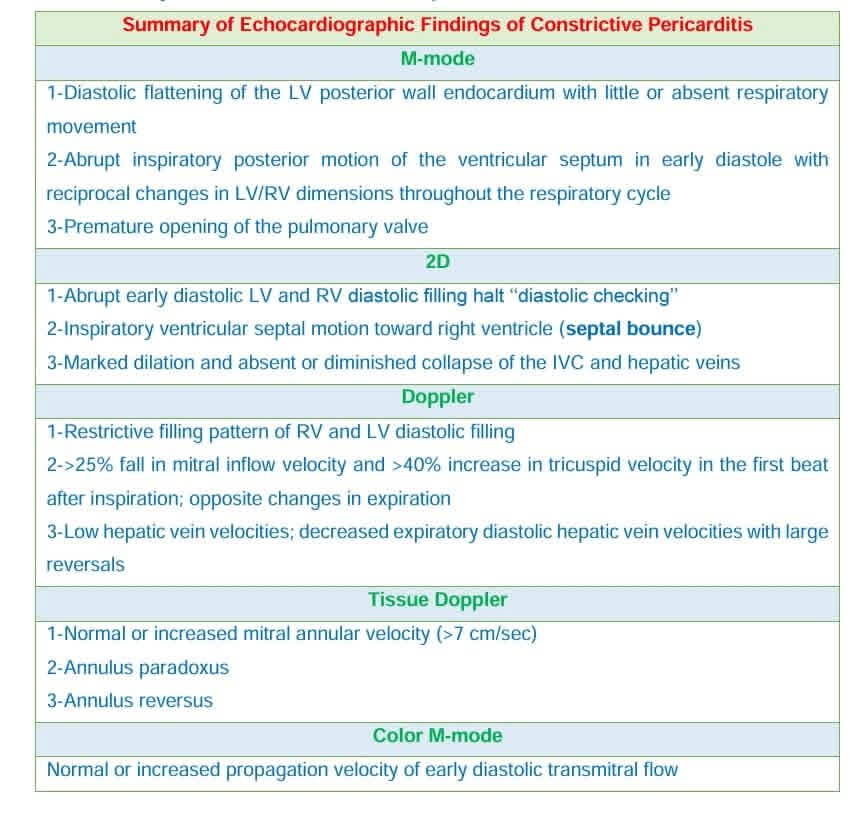
🚨 Echocardiographers! 🚨
Quick pearls on Constrictive Pericarditis from my book Tips & Tricks in Echocardiography 📚❤️
💡 Save time at bedside & exams.
✍️ Share your echo tips.
DM for your copy 🌍 (International shipping is available).
#Echocardiography #EchoTips #MedEd
20
73
6,532
8 Sep 2025
🫀 Echo Pearl
Non-coronary cusp Aortic Valve Prolapse ➡️ Moderate AR
🔎 Jet clue: Vertical, anteriorly directed, eccentric AR jet
👉 Always think cusp prolapse!
#Cardiology #EchoTips #AorticValve #AR
4
6
47
2,915
23 Aug 2025
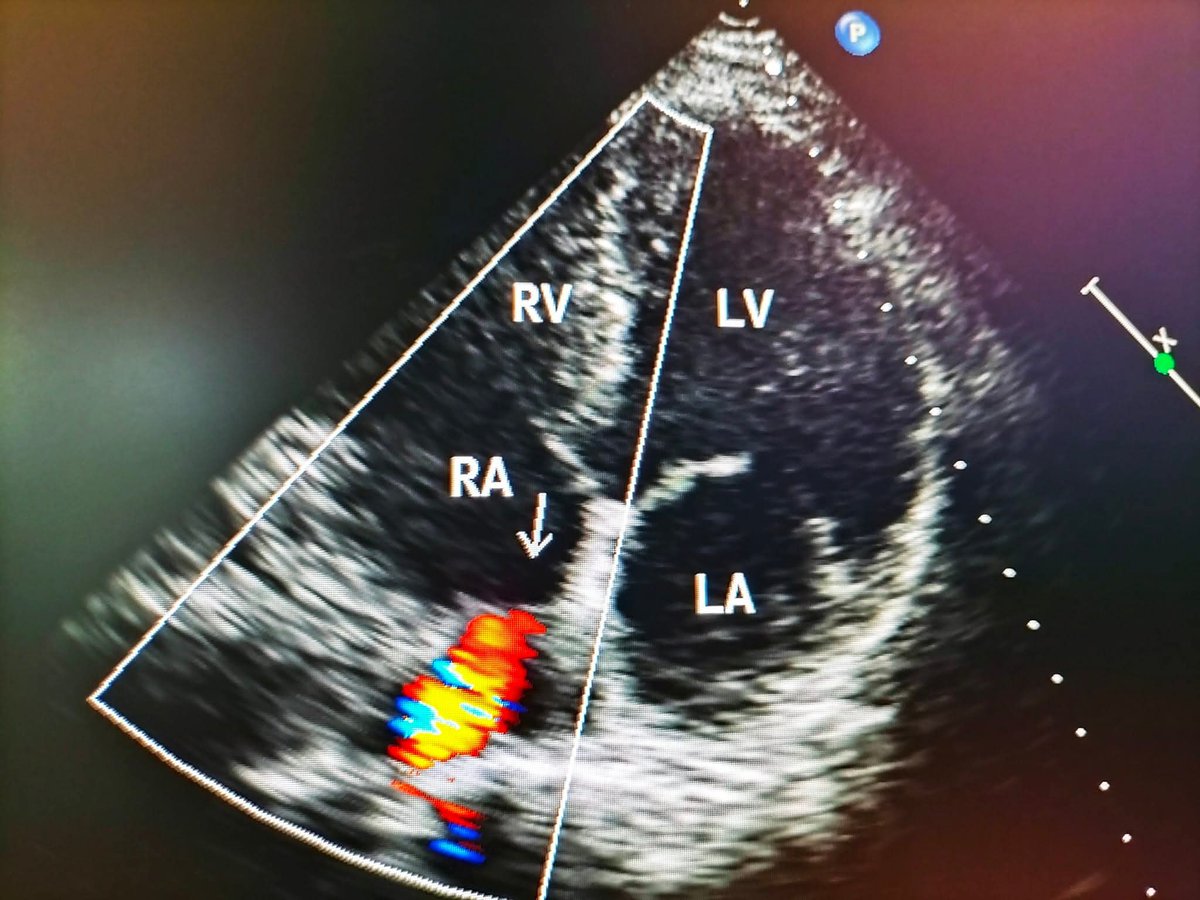
🫀 Echo Pearl
Not every RA jet = shunt 👀
This color flow is just exaggerated IVC inflow ➡️ a normal variant, not ASD/PFO ❌
#Cardiology #Echocardiography #EchoTips
1
4
469
29 Jul 2025
🧠 ¿Qué es la Fracción de Acortamiento (FS)?
Vamos a explicarlo paso a paso con 🍎🍏 👇
Es una forma rápida y sencilla de estimar la función sistólica del ventrículo izquierdo 🫀.
Mide qué tanto se contrae el VI durante la sístole, comparando el tamaño del ventrículo entre la diástole y la sístole.
📐 Fórmula:
FS%= (LVIDd - LVIDs) / LVIDd x 100
🍏 LVIDd: Diámetro interno del VI en diástole
🍎 LVIDs: Diámetro interno del VI en sístole
FS = (🍏 - 🍎) / 🍏 x100
🧪 Ejemplo práctico
Supongamos que mides:
•LVIDd = 50 mm
•LVIDs = 30 mm
Entonces:
FS% = (LVIDd - LVIDs) / LVIDd
FS% = [(50 - 30) / 50] X 100
FS% = 40%
📊 ¿Qué valores se consideran normales?
•✅ Normal: 25% – 45%
•⚠️ Disminuida: < 25%
•🔺 Alta (hiperdinámico): > 45% (por ejemplo, en sepsis temprana)
📌 Nota importante:
La FS solo evalúa el eje corto del VI, así que es útil pero no reemplaza a la fracción de eyección por métodos volumétricos.
Aun así, es muy práctica y rápida en POCUS 🧏🏽♂️
💬 Si estás en urgencias o en UCI y necesitas una estimación funcional del VI, la FS es rápida.
#FracciónDeAcortamiento #EchoTips #POCUS #Ecocardio #FunciónSistólica #MedicinaCrítica #Urgencias
1
31
99
5,005
28 Jul 2025
🧠 ¿Qué es la Fracción de Acortamiento (FS)?
Vamos a explicarlo paso a paso 🧮👇
Es una forma rápida y sencilla de estimar la función sistólica del ventrículo izquierdo 🫀.
Mide qué tanto se contrae el VI durante la sístole, comparando el tamaño del ventrículo entre la diástole y la sístole.
📐 Fórmula:
FS%= (LVIDd - LVIDs) / LVIDd x 100
🍏 LVIDd: Diámetro interno del VI en diástole
🍎 LVIDs: Diámetro interno del VI en sístole
FS = (🍏 - 🍎) / 🍏 x100
🧪 Ejemplo práctico
Supongamos que mides:
•LVIDd = 50 mm
•LVIDs = 30 mm
Entonces:
FS% = (LVIDd - LVIDs) / LVIDd
FS% = [(50 - 30) / 50] X 100
FS% = 40%
📊 ¿Qué valores se consideran normales?
•✅ Normal: 25% – 45%
•⚠️ Disminuida: < 25%
•🔺 Alta (hiperdinámico): > 45% (por ejemplo, en sepsis temprana)
📌 Nota importante:
La FS solo evalúa el eje corto del VI, así que es útil pero no reemplaza a la fracción de eyección por métodos volumétricos.
Aun así, es muy práctica y rápida en POCUS 🧏🏽♂️
💬 Si estás en urgencias o en UCI y necesitas una estimación funcional del VI, la FS es rápida.
#FracciónDeAcortamiento #EchoTips #POCUS #Ecocardio #FunciónSistólica #MedicinaCrítica #Urgencias
3
3
781
28 Jul 2025
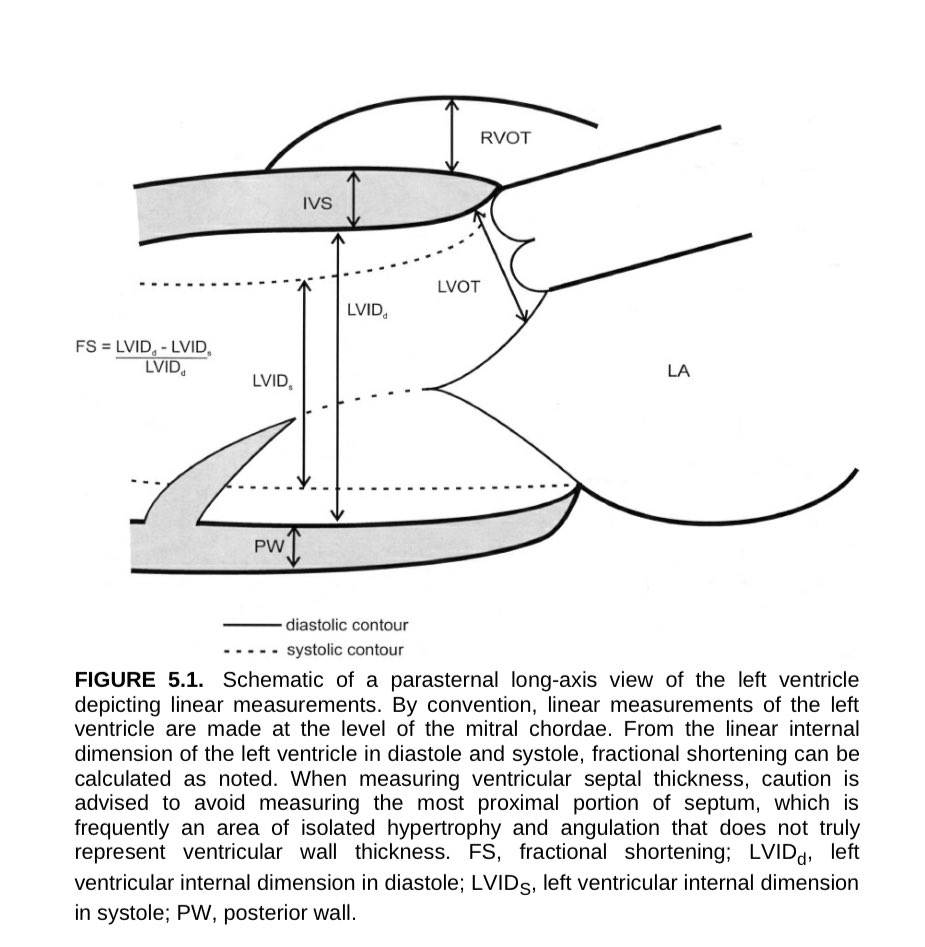
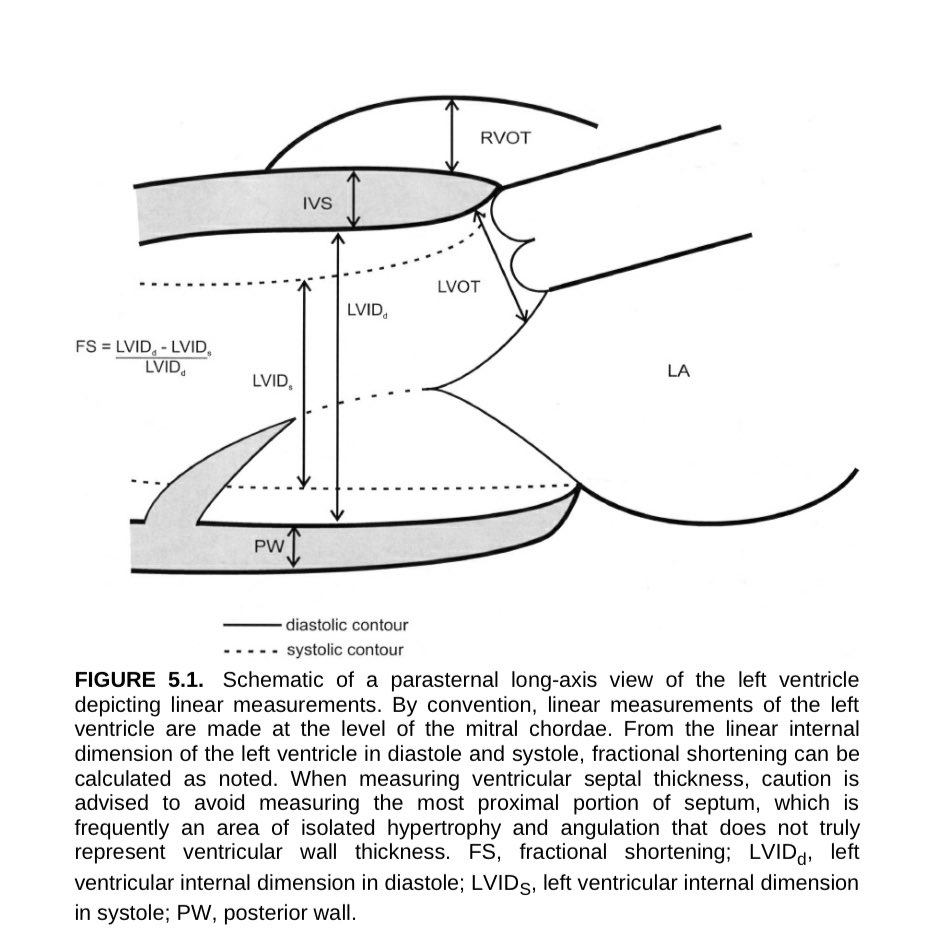
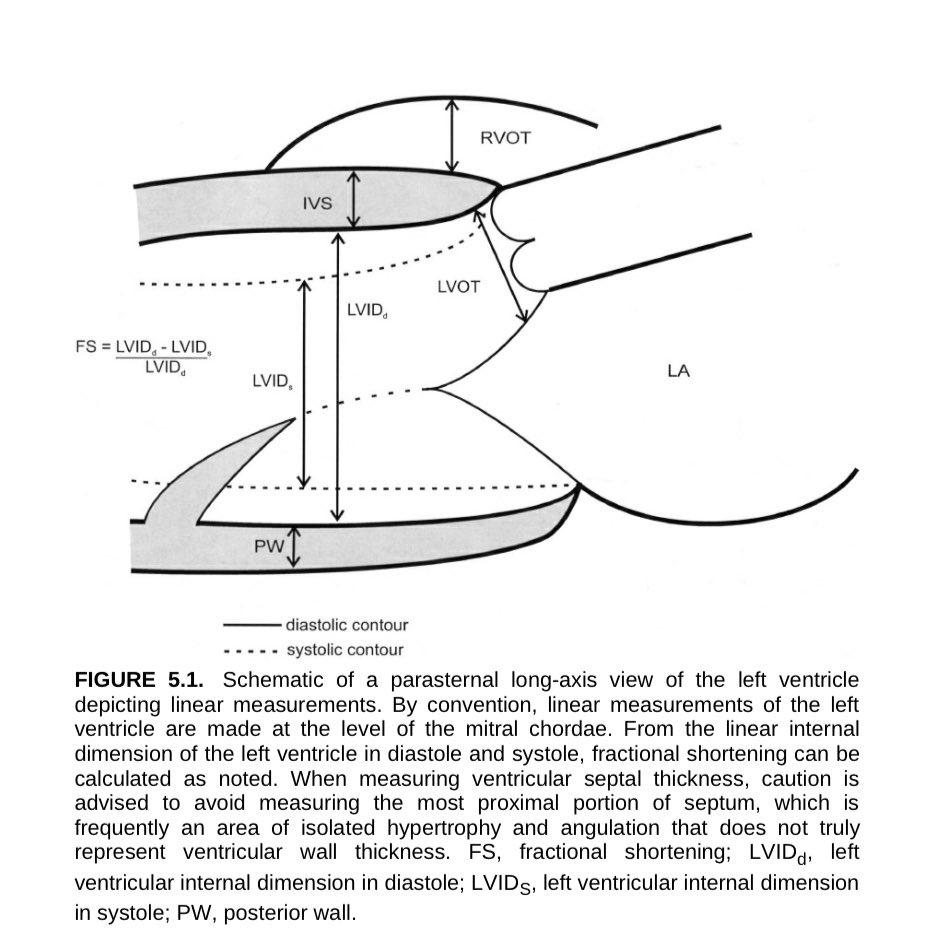
🫀 Hoy revisamos uno de los planos clásicos del #ecocardiograma el eje largo parasternal! La clave para medir bien 🧪 tu ventrículo izquierdo
📐 ¿Qué se mide aquí? 🤷🏽♂️
📏 En el eje largo parasternal, las mediciones #lineales del VI se hacen a nivel de las cuerdas tendinosas mitrales.
🔍 Estas son las estructuras y mediciones principales:
•💆🏽♂️ LVIDd: Diámetro interno del VI en diástole
•💪🏽 LVIDs: Diámetro interno del VI en sístole
•➗ FS: Fracción de acortamiento
FS% = (LVIDd - LVIDs) / LVIDd x 100
•🧱 IVS: Tabique interventricular
•🧱 PW: Pared posterior
•🫁 RVOT: Tracto de salida del ventrículo derecho
•🫀 LVOT: Tracto de salida del VI
⚠️ ¡pero ojo!
📌 No midas la porción más proximal del tabique 🧱, ya que suele haber hipertrofia aislada y angulaciones que no reflejan el grosor real de la pared.
🧙🏼 Este plano es básico para estimar función sistólica, valorar hipertrofias y obtener medidas confiables.🫀
#Ecocardio #POCUS #EjeLargo #UltrasonidoC #EchoTips #EchoBasics #FractionalShortening #LVfunction
1
43
136
7,493
14 Jul 2025
🎯 Echo Tip
🖼️ Modified Apical 3-Chamber View
🔄 Achieved by cranial angulation of the probe
🔁 Similar to RV inflow view
👁️ Clearly shows the coronary sinus
✅ Useful for assessing:
• Tricuspid Regurgitation
• PASP
#EchoTips #Cardiology #TR #PASP #Echocardiography
3
13
48
3,763

25 May 2025
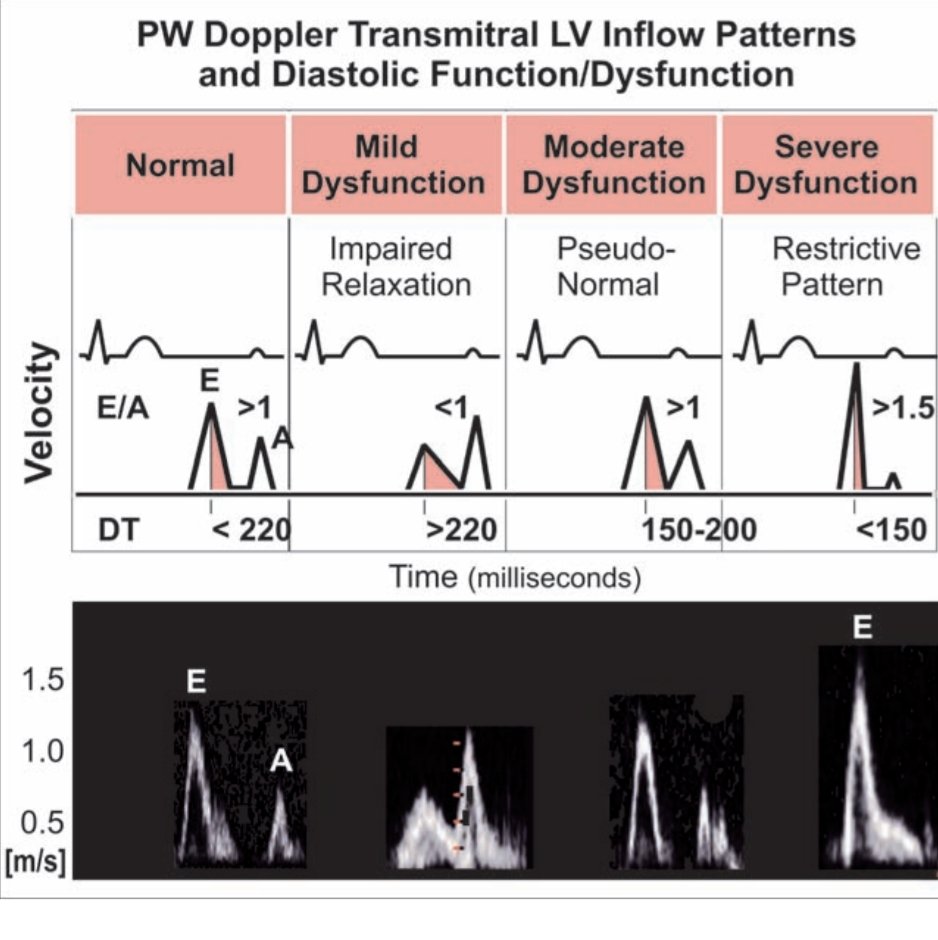
Normal & Abnormal Transmitral LV Inflow Patterns
Understanding Doppler signs of LV diastolic dysfunction is key for diagnosis & prognosis.
1️⃣ Normal Diastolic Function
- E/A >1, DT <220 ms
- Mechanism: Normal LV relaxation & compliance → early diastolic filling dominates (E wave).
🔵Clinical: Normal filling pressures. Seen in healthy individuals.
2️⃣ Mild Dysfunction (Impaired Relaxation)
- E/A <1, DT >220 ms
- Mechanism: LV relaxation is delayed → ↓E wave, compensatory ↑A wave.
🔵Clinical: Often asymptomatic; seen with aging, HTN. May progress if underlying cause persists.
Treatment: Control BP, optimize comorbidities to prevent worsening.
3️⃣ Moderate Dysfunction (Pseudonormal Pattern)
- E/A >1, DT 150–200 ms
- Mechanism: ↑LA pressure masks impaired LV relaxation, making E wave appear normal.
🔵Clinical: Filling pressures are elevated. Patients may have exertional dyspnea.
Trick: Use Tissue Doppler (e') or Valsalva to unmask.
Prognosis: Worsening diastolic dysfunction; requires intervention.
4️⃣ Severe Dysfunction ( Restrictive Filling)
- E/A >1.5, DT <150 ms
- Mechanism: Severely non-compliant LV; very high LA pressure → rapid, short early filling (↑↑E), minimal atrial contribution.
🔵Clinical: Seen in advanced heart failure, restrictive cardiomyopathy.
LV diastolic dysfunction is progressive. Doppler patterns evolve from impaired relaxation → pseudonormal → restrictive.
Recognizing these stages helps in early intervention and improving outcomes.
#EchoTips #MedEd #DiastolicHeartFailure #CardioTwitter
1
82
329
25,965
24 May 2025
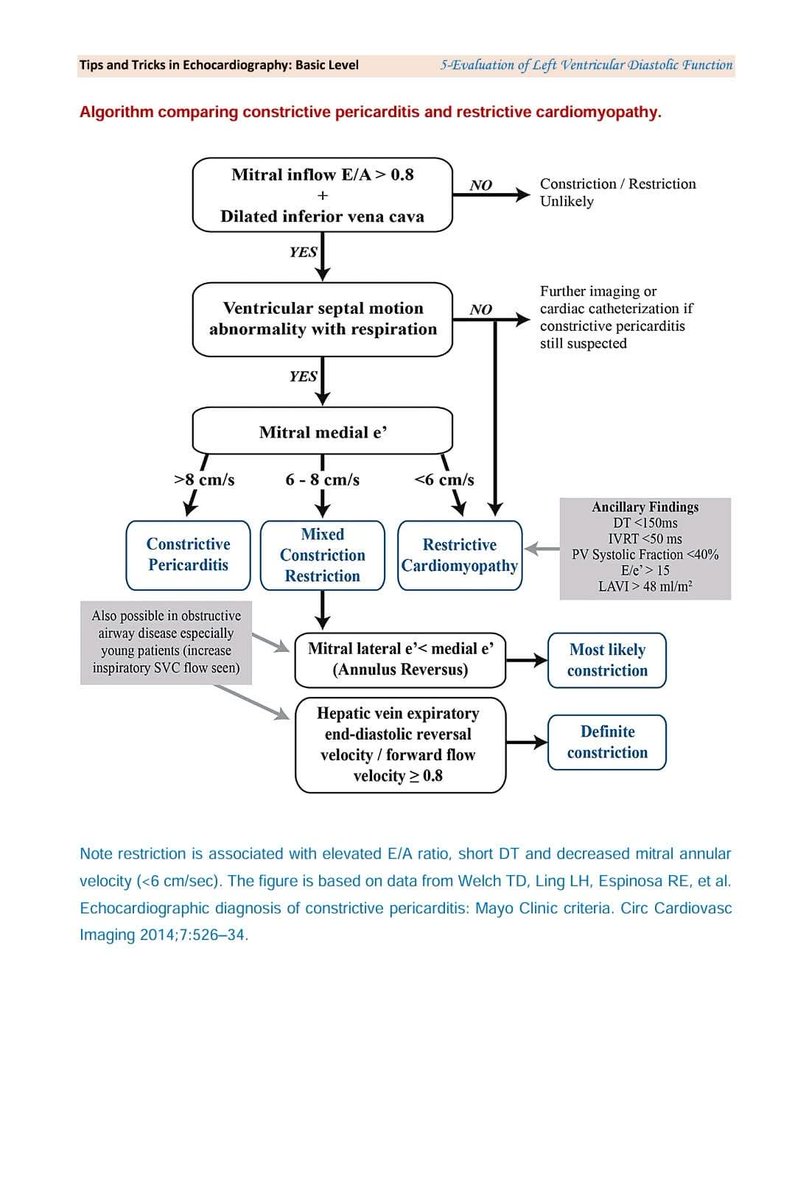
Struggling with CP vs. RCM?
Check out this high-yield algorithm from my book Tips and Tricks in Echocardiography!
Quick. Visual. Practical.
One post can save your echo day.
Don’t miss it!
#EchoTips #CardioPearls #EchoMadeEasy
1
18
55
12,147
17 May 2025
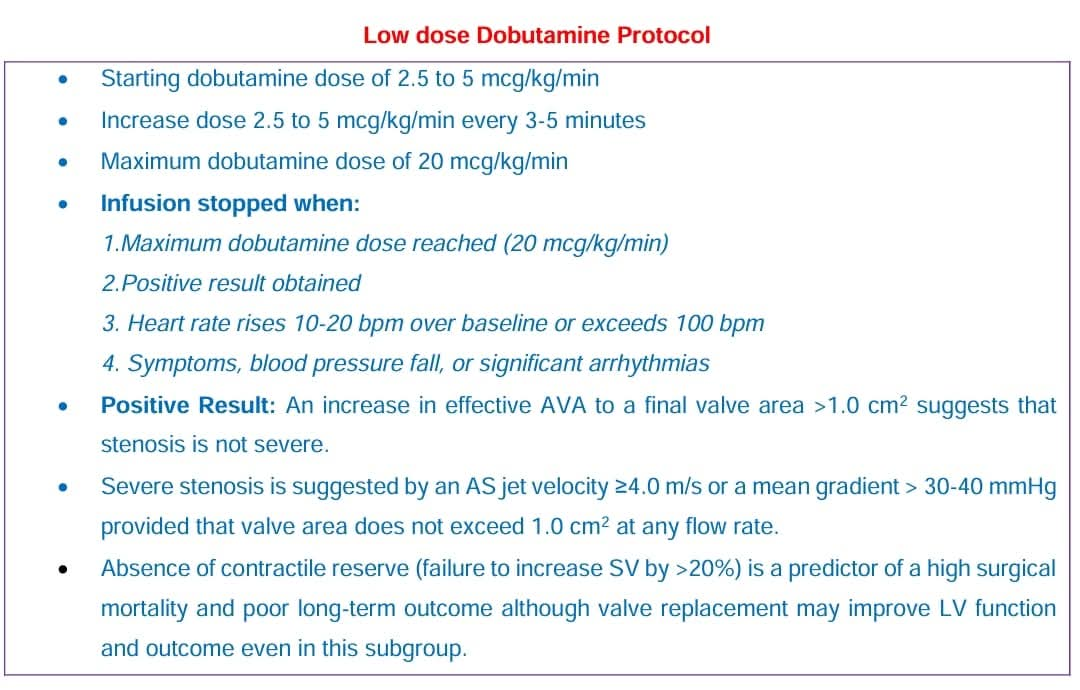
Low-Flow, Low-Gradient AS?
Use Low-Dose Dobutamine Echo to:
✅Confirm severity (AVA >1 cm² = pseudo-severe)
✅Check for contractile reserve
✅Guide surgery decisions
Details in my book "Tips and Tricks in Echocardiography"
#CardioTwitter #EchoTips #LFLGAS #DobutamineEcho
1
8
23
2,184

8 May 2025
What is the D Sign? 📈 Echo Example Showing D Sign in Systole & Diastole!
Watch Now: youtube.com/shorts/JMvGYqm_N…
#Echocardiography #DSign #CardiologyEducation #EchoTips #diagnosis #echosingh #prime
2
20

20 Jan 2025
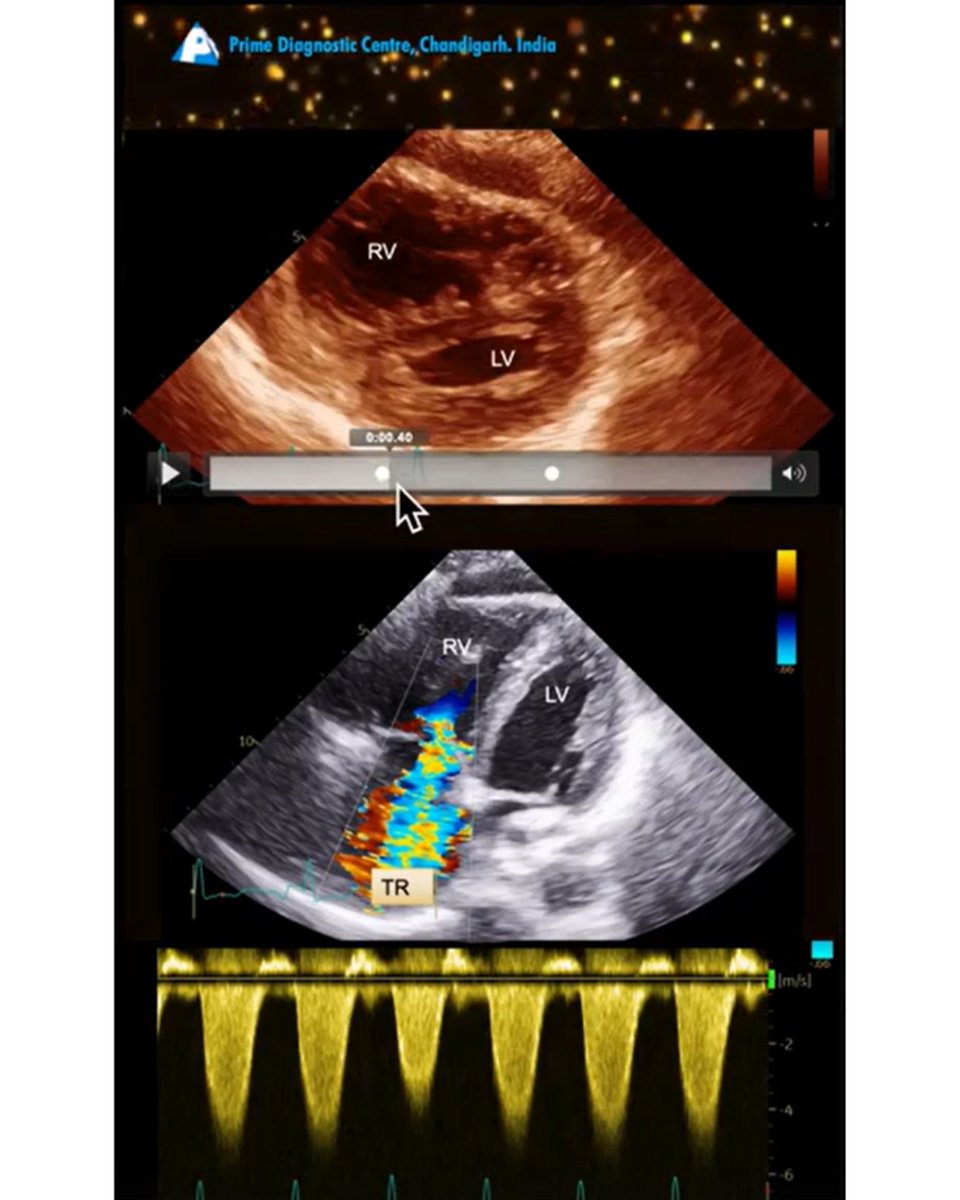
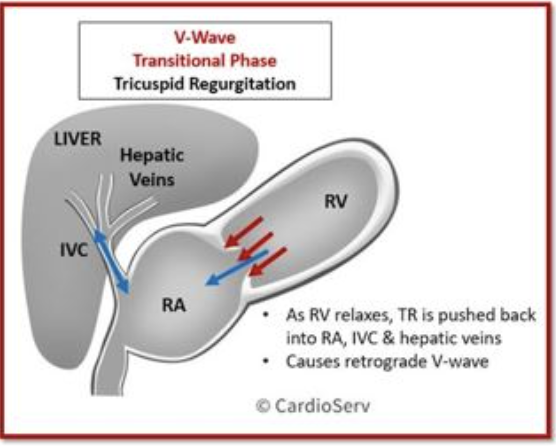
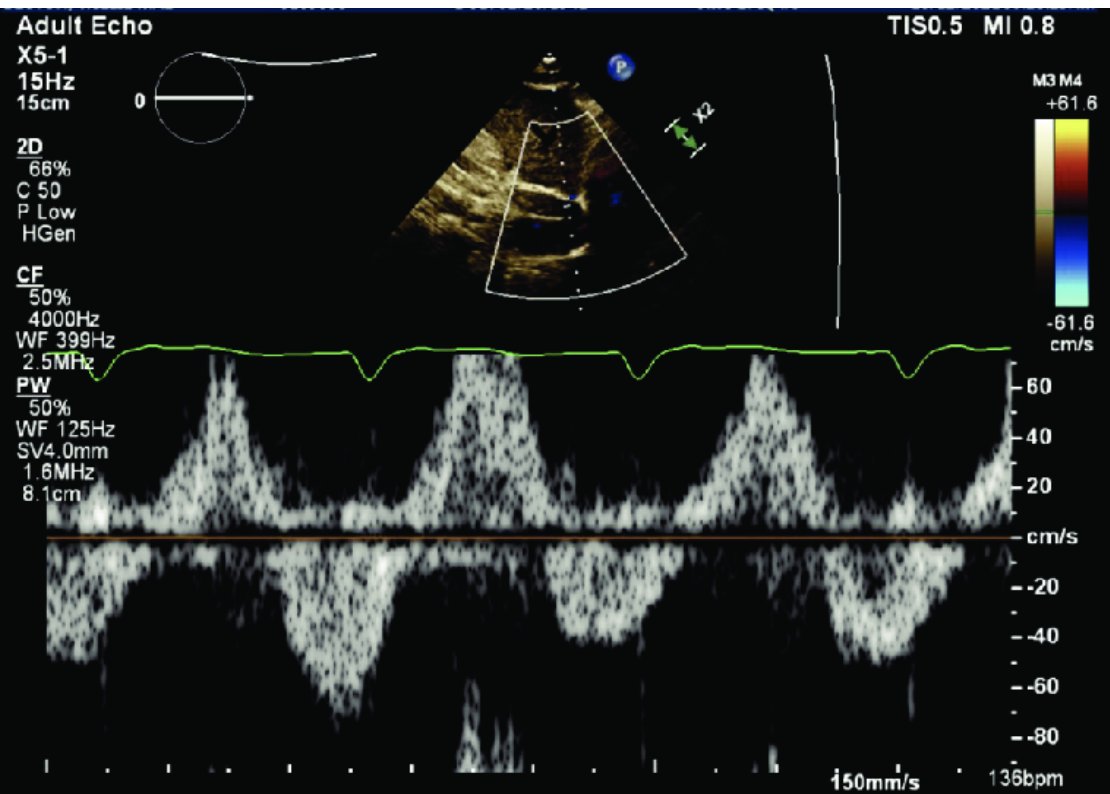
#CardioNugget 20/365
Severe TR?
Look for hepatic vein systolic flow reversal on Doppler!
Technique:
1. Use subcostal view
2. Sample 2–3 cm from IVC entry 📏
3. Pulsed-wave Doppler (PWD) 🎯
#CardioNuggets #EchoTips #CardioTwitter
researchgate.net/publication…
4
21
116
6,737

13 Jan 2025
From classical parasternal PLAX to right parasternal view: simply cross the sternum, staying in the same imaging plane. This maneuver optimizes Doppler alignment for AS assessment. A small move, big impact! 🫀✨ #EchoTips #Cardiology
3
28
97
5,267

13 Jan 2025
#Scanuary Day 13 Alert!
Ready to take your echo skills to the next level? 🚀 Today, we're diving DEEP into some slightly more advanced techniques than 2D echo in the emergency setting. Think extended views, Colour Doppler mastery, M-mode secrets, and more! #Scanuary #POCUS #Echotips
@casualtysrus @davemaca1yahoo1 @Katita1981 @salmannaeem217
3
9
26
6,344

12 Jan 2025
I usually say “sit the probe on the edge of the lower rib and stretch the skin so u can look between”- all the teachers have same idea just different ways to explain:) #POCUS #echoPearls #echoTips
3
30
12 Jan 2025
The great IVC mimic!
Pitfall: Mistaking the descending aorta for the IVC is common pitfall, but the right hepatic vein can mimic the IVC too. Trace back to the RA, visualise the IVC-RA junction and the hepatic vein coming off the IVC.
Remember: IVC size & collapsibility are influenced by many factors (anatomical and physiological). It's NOT a direct measure of fluid status, it reflects right atrial pressure and to some extent TV competency.
Assess BOTH short & long axis! Don't forget the short axis – the IVC isn't a perfect cylinder. #echotips #cardiotwitter #Scanuary
1
2
8
341
12 Jan 2025
A4C view looking off?
Foreshortening: Ventricles look rounded? Try moving your probe an intercostal space lower or more laterally.
Septum leaning left? Tilt the probe tail more laterally.
RV too small? Turn the probe clockwise.
Can't see the atria? Tilt the probe tail towards the bed. #echotips #cardiotwitter #Scanuary
1
3
8
378
12 Jan 2025
How do you know you're on axis? The LV looks like a bullet, the apex stays put, and you can visualise the pulmonary vein.
Here are 3 apical views from ED patients all having slightly different pathology. Aim for this in all your patients.
#echotips #cardiotwitter #Scanuary
1
2
8
499