
EDIT: other anti-IL33 mAbs didn't do this during their screening campaigns and subsequently didn't have the same tight binding to the active form of IL33. However, I expect the in silico engineering tools of today would easily and quickly resolve this
IL33 rapidly oxidizes, and inactivates when released. When Medimmune developed this mAb a lot of work went into screening campaign to ensure the reduced (active) version of IL33. At the time, other IL33 didn't do this. This is a story of very careful engineering
1
1
Bilal Ramez retweeted

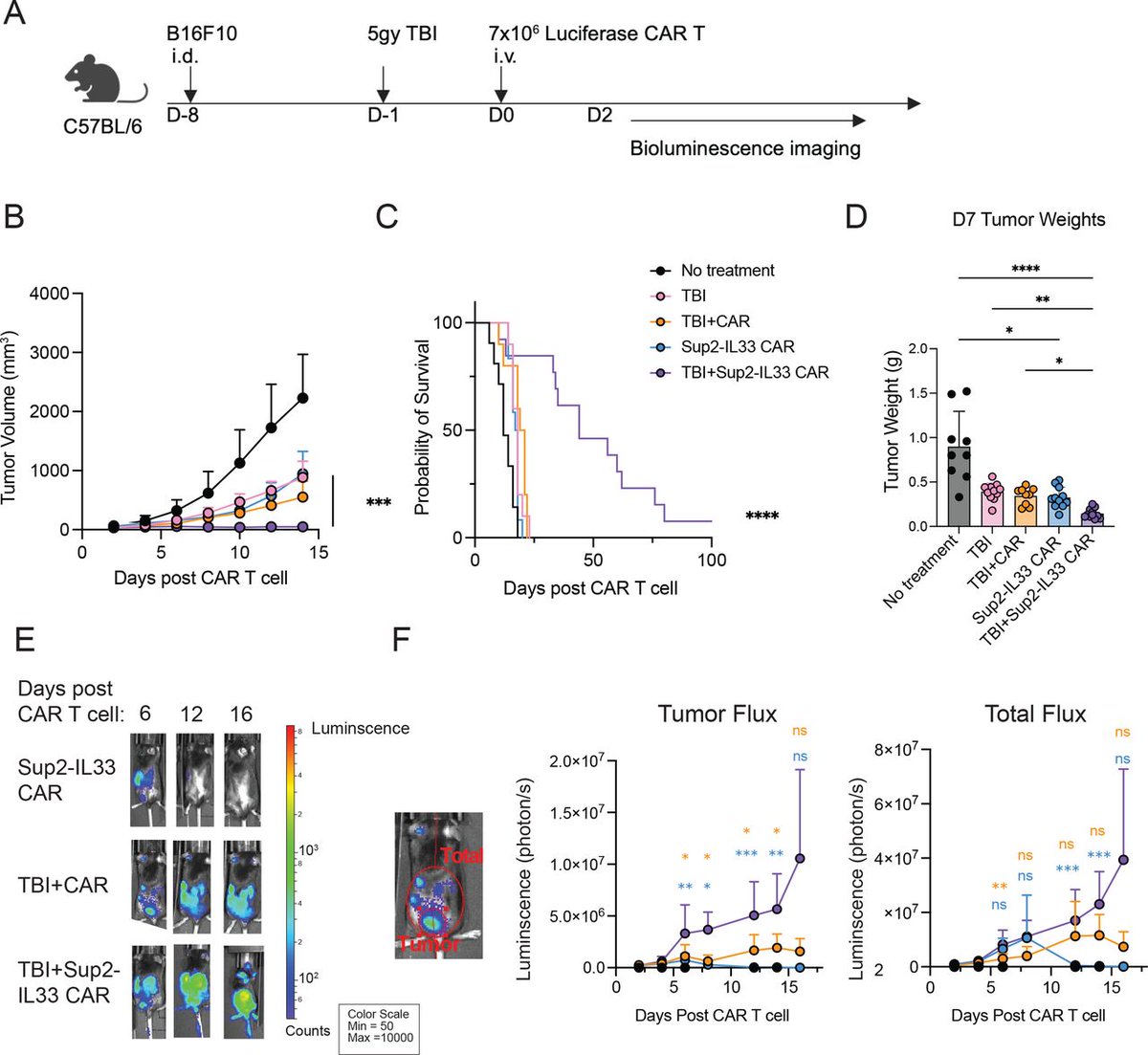
New #JITC article: "Systemic pre-conditioning favors effector over exhausted CD8 T-cell subsets following Sup2-IL33 armored CAR T-cell therapy" jitc.bmj.com/content/14/6/e0…
@SundrudL @GeiselMed
1
5
15
941

Jun 12
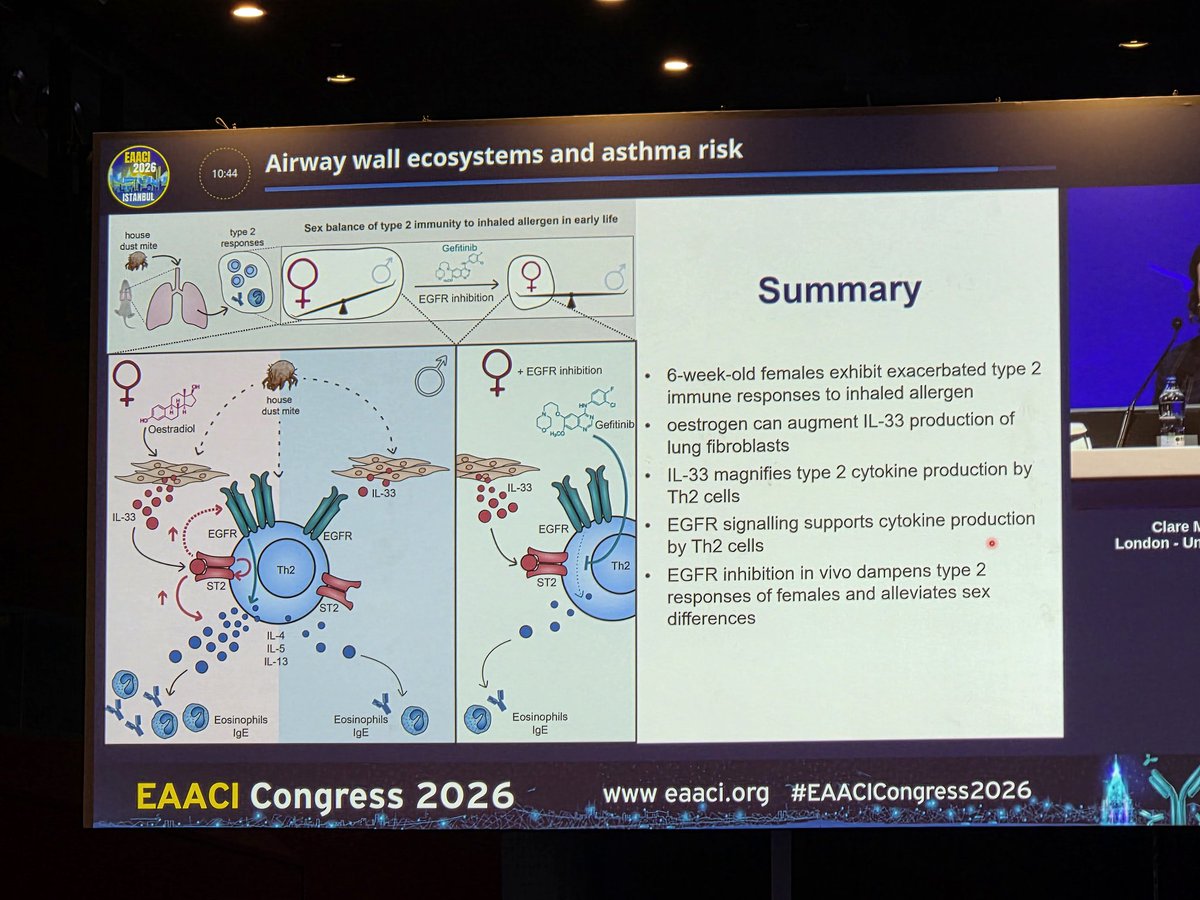
IL33 and augumentation effect of estrogen on IL 33 and collagen production in female mice..linking severe asthma and effect of estrogen #Asthma
#EAACICongress2026
1
1
59
Jun 12
Increased IL33 is associated with deposition of collagen and EGFR in a dysregulated manner in children with severe asthma #EAACIcongress2026
1
45

A lot of Step backs for $SNY recently in I&I, The expectation from them were very high because they really have a strong diversified I&I but they faced three step-backs in the last couple of months in C1, IL33 and OX40...etc. Small Pharma continue to cook the big pharma with better molecules. Time to shop for $SNY, you have $IMVT, $DNTH, $NKTR, $CRVS, $ORKA, you can pick two. My recommendation will go for IMVT because it's more safer bet for your stupidity in DD.

Riliprubart was one a few Ph3 trials for $SNY and was expected to one of the €2-€5 Billion peak sale drugs

2
5
2,107


No offense bro, but the market never, ever bought these comments.
Irony here is they are in the commercial position they are in because of their R&D capabilities.
Market doubts they can repeat successes.
Fianlimab outcome (& il33 COPD trial during Covid) seems bad luck to me.
2
4
155

$CRVS $NKTR
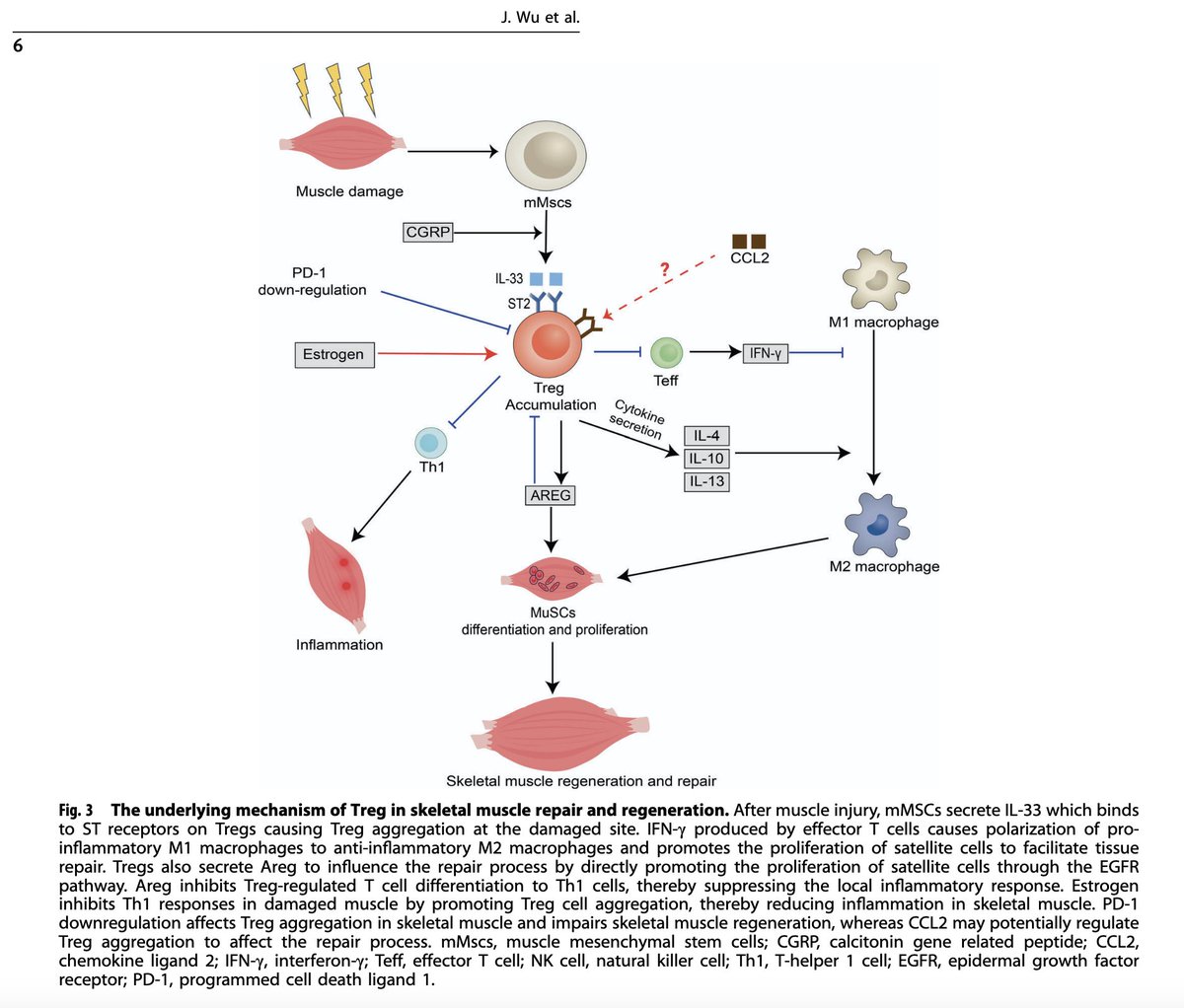
Increasing #Tregs may be effective reducing inflammatory damage in Duchenne muscular dystrophy, retarding progression of disease and regenerating lost skeletal muscle
nature.com/articles/s41419-0…
Therapies that increase Tregs could be beneficial in this terrible disease and would be exciting to see this indication pursued
The Treg IL33/ST2/AREG axis in a non-immune role for Tregs that can increase muscle growth reduce atherosclerosis. Two major indications to also pursue.
* Tregs stimulate muscle stem cell differentiation and muscle repair and regeneration by promoting the polarization of #M1 pro-inflammatory phenotype macrophages to #M2 anti-inflammatory phenotype macrophages and the release of the specific growth factor dual regulator #Areg
31 Jan 2025
#FOXP3 #Tregs concentrate in skeletal muscle, promote tissue regeneration post-injury
Therapeutic potential for Tregs to treat #Duchenne muscular #dystrophy, improvement shown
$CRVS #soquelitinib blocks ITK, increases ⬆️Tregs, new potential indication?
pnas.org/doi/10.1073/pnas.19…

2
5
53
5,799

May 15
113 model combinations extracted diagnostic markers and therapeutic target candidates from multimodal data
This study analyzed the gut–immune–lung axis in idiopathic pulmonary fibrosis (IPF) by integrating bulk lung transcriptomes, single-cell RNA-seq, spatial transcriptomics, GWAS/Mendelian randomization, drug-signature prediction, and experimental validation.
1) Data used for machine learning
- training: merged bulk lung transcriptomes from GSE32537 GSE110147
- features: gut–immune–IPF candidate genes after DEG / WGCNA / gut-gene / immune-gene filtering
- label: IPF vs control
2) Analysis flow
bulk transcriptome discovery ->-> DEG WGCNA-based candidate extraction ->-> intersection with gut microbiota-related and immune genes ->-> 23 gut–immune–IPF candidate genes ->-> PPI hub prioritization 113 feature-selection/classification pipelines ->-> four core genes: CXCL13, IL33, TLR4, IGF1
3) Top machine-learning pipelines
- Lasso GBM:
LASSO-based sparse gene selection -> nonlinear classification by GBM
- Stepglm[both] NaiveBayes:
bidirectional stepwise GLM selection -> Naive Bayes classification
- Lasso NaiveBayes:
LASSO-based reduction to a small gene set -> probabilistic classification
- RF NaiveBayes:
random-forest-derived feature importance -> Naive Bayes classification
- Stepglm[backward] NaiveBayes:
backward elimination of predictors -> Naive Bayes classification
- glmBoost NaiveBayes:
boosted GLM-based feature selection -> Naive Bayes classification
- NaiveBayes:
probabilistic classification without strong upstream feature-selection preprocessing
- glmBoost GBM:
boosted GLM-based feature selection -> tree-boosting classification
- Stepglm[both] GBM:
stepwise variable selection -> GBM classification
- RF GBM:
random-forest-based feature candidate evaluation -> GBM classification
My scientific thought:
The results suggest that LASSO-based preprocessing was particularly effective. LASSO has strong ability to reduce predictors to a small explanatory set, which is useful in transcriptomic analyses where the number of genes exceeds the number of samples.
The fact that Lasso GBM appeared as the top-performing pipeline suggests a good match between sparse gene selection and nonlinear boosting-based classification. GBM can capture nonlinear gene relationships and threshold-like separation, but it may overfit when too many input genes are included.
#Bioinformatics #ComputationalBiology
2
2
5
529

Now online: DDR1 Promotes Immune Evasion in Colorectal Cancer by Orchestrating IL33-Mediated M2-like Polarization of Tumor-Associated Macrophages doi.org/10.1158/2326-6066.CI…

3
165

May 12
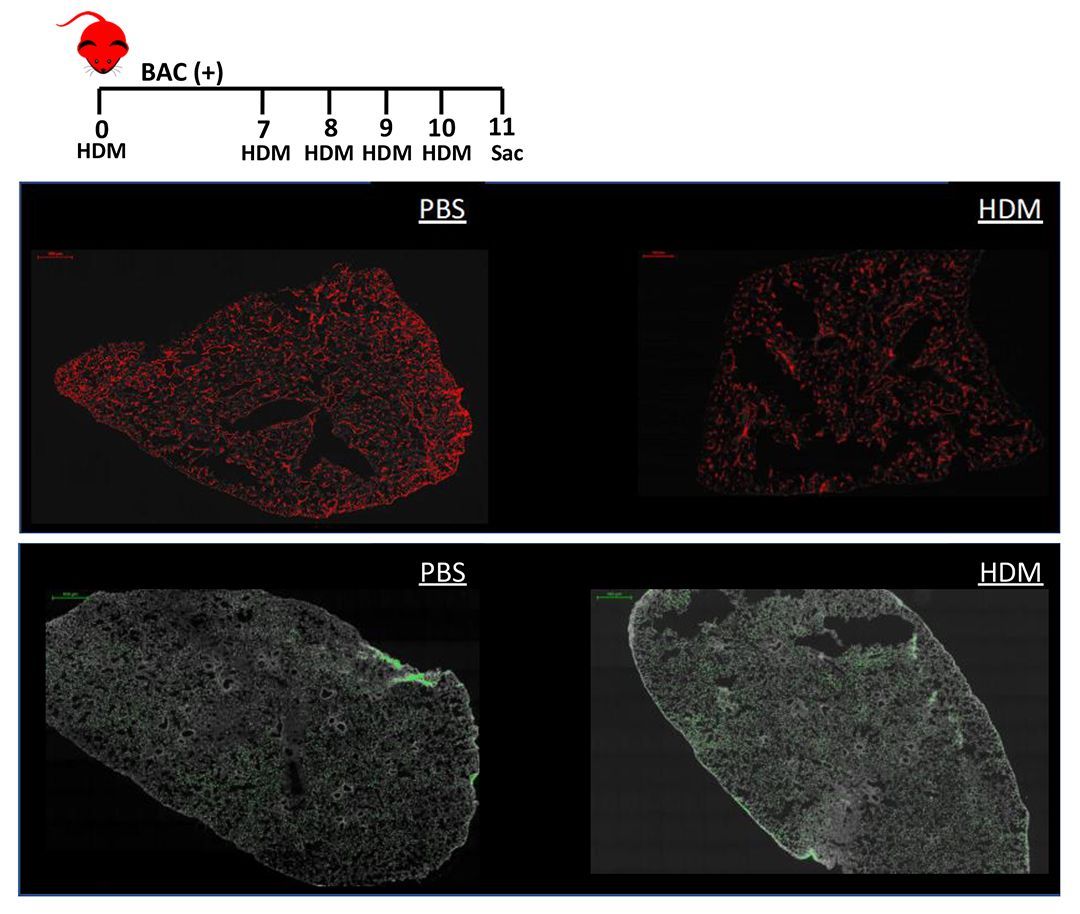
IL-33 is involved in #AllergicAsthma but is differentially regulated in mice and humans.
doi.org/10.1172/jci.insight.…
Here, Anne I. Sperling & team @UVA employ an elegant genetic tool to identify a negative feedback loop for endothelial #IL33 expression in response to either allergen or exogenous IL-33.
The figure shows downregulation of the hIL33 reporter in the lung following intratracheal administration of house dust mite (HDM) extract.
1
3
12
893

I don’t think the second is not being discussed. I think epithelial alarmins could definitely be relevant. We collect RNA levels of epithelial alarmins in our research and I’d like to do more research into it.
The question for the epithelial alarmin however is what’s driving it.
Possibly covid induced vascular damage through red blood cell issues and NETs.
Or mast cells themselves can release epithelial alarmins, hence the reactivity not stemming from the epithelial themselves, but from reactive priming now furthering priming.
I’d love to see some clinical trials into mast cell depletion, TSLP inhibition, and IL33 inhibition
Mainly because I’m unsure you can actually escape all triggers. I have triggers to airborne particles that cause narcolepsy, but, when I go to a HEPA filtered room for days, the narcolepsy disappears, but I remain extremely ill still. So either part of the illness is not a reaction to environment, or there’s something in all environments (or in the body) that you can’t escape and have to biological tackle the increased alarm signals
3
1
8
341

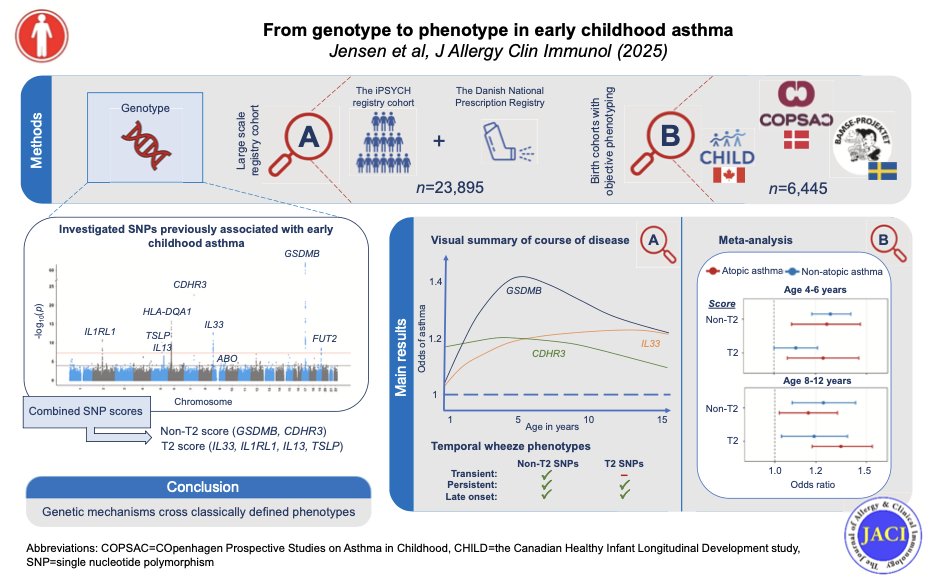
小児喘息の「一過性喘鳴か、持続型か」という臨床分類、実は遺伝子の側から見ると境界が曖昧かもしれない。23,000人超の小児を出生から15歳まで追跡した本研究では、GSDMB・CDHR3が生後早期から最も強いリスク遺伝子座として働き(1歳時のCDHR3: OR 1.17)、学齢期に効果が減弱する。
一方、IL33・TSLP等のT2関連遺伝子座は2〜3歳から効果が現れ、15歳まで増大し続ける。
興味深いのは、どちらのスコアもアトピー型・非アトピー型の両方に関連していた点だ。
つまり「アトピーか否か」という従来の二分法では、背景にある疾患メカニズムを十分に捉えきれない可能性がある。
日常診療では「喘鳴の時期」と「感作の有無」で予後を語りがちだが、遺伝的メカニズムはその枠を横断している。
エンドタイプに基づく層別化が、将来の予防・治療戦略を変えうるのかもしれない。
J Allergy Clin Immunol 2026;157:833-42.
2
185

Apr 21
What about the tissue injury surrounding those infected epithelial cells with OSM, IL33, IL25 getting secreted and mast cells coming in to check out what's going on?
3
1,348