
This photo was sent in from Iowa showing a competitor mix (left) vs. Physagro products (right) on corn. 🌽
Mix includes: 16oz #BioGreen, 16oz #MicroBoost, 6oz #AcceleratePro, and some CetaiN.
Nice work!

7

Jun 10
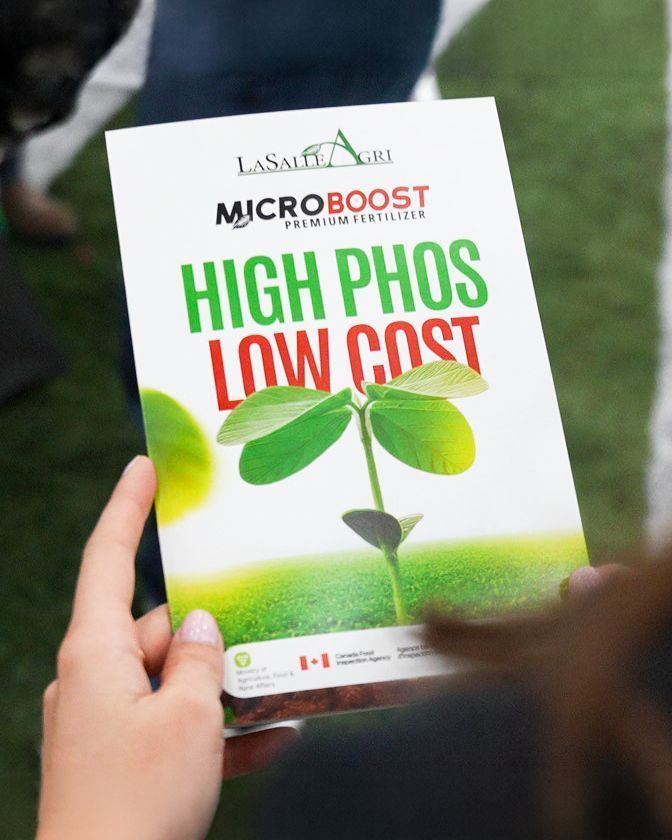
💡 Why settle for MAP when MicroBoost delivers more? With naturally high P₂O₅ levels, MicroBoost outperforms conventional phosphorus sources fueling stronger yields and healthier soils where it counts. More phosphorus. More results. Made for Ontario farmers. 🌾
To get more results at an affordable price call 226-799-7330
#MicroBoost #LaSalleAgri #SoilHealth #CropYields #FarmerOwned
24

Under the #MGMG programme, ICAR-CIFT organized an awareness-cum-training programme on CIFT Microboost & Organic Fertilizer Production from Waste on 26 May 2026.
35 participants attended
Waste-to-wealth approaches
Organic farming technologies
Logo launch of Anvaya Farms




2
41

[商願2025-95786]
商標: [画像] (標準文字)
OCR: MICROBOOST
出願人: 株式会社komham (北海道)
出願日: 2025年8月20日
区分: 第40類(廃棄物の破砕処理,廃棄物の再生,廃棄物の焼却処理,アップサイクリング,土壌処理,廃棄物の変形処理), 第42類(電子計算機のプログラムの設計・作成又は保守,技術的課題の研究,科学技術に関する研究,生物に関する研究,細菌に関する研究,科学に関する研究,…)
385

Jun 3
Agree with that interpretation! I think a good potential use case could be UIR with goal of avoiding ADT but would need to see how it compares to some form of dose escalation likely microboost
1
2
99
Jun 3
Very interesting work. Biopsy aside, not sure what to make of the DFS benefit as it largely disappeared in the ADT group, or if you'll still see it if you dose escalate, e.g. microboost
1
2
317

Jun 1
Would be fantastic to see if 1y ADT may be adequate in context of high risk receiving EBRT microboost (similar to BT data). Conceptually though, especially given decreased nodal recurrences per FLAME, seems plausible. Just not sure there are any ongoing trials looking at this...
1
4
296

May 21
Don’t worry much re urethra at 37.5 Gy/5. It’s critical when I microboost/SIB and in reirradiation.
When learning MRI contouring, I did internal comparisons by contouring the same images 3-4x to see if I was even consistent. Consistency≠accuracy, but it sets foundation for PI
2
194

May 1
Also, real benefit of ADT considering all changes:
- better imaging, higher sensitivity staging
- Higher RT dose, maybe microboost?
- Better positioning, more precise treatments. How many more men are being cured just because we got better at firing photons?
1
2
49
ICAR-CIFT & ICAR-KVK Kottayam conducted a National Campaign on Balanced Fertilizer Use at Ullala village(28 Apr 2026).Farmers trained in natural farming & reduced chemical use
Showcased CIFT MicroBoost for organic manure from fish waste
Strong interest in field trials & training



2
8
176
Awareness Programme on Balanced Use of Fertilizers & CIFT Microboost held at North Paravoor (27 Apr 2026) by ICAR-Central Institute of Fisheries Technology & Agricultural Technology Management Agency.



3
6
108
Mar 23
Agree with this - but after conversation with @alison_tree, I have had pause to escalate DIL in context of whole gland 40/5, although my baseline preference is often 64-67/20 microboosts, not SABR microboost (though I favor microboost in context of SABR when enrolling on GU013)
Take DELINATE SABR cohort E for example (30-36.25-40-45/5). Late (2-3y) RTOG GU G3 toxicity of 12% which is higher than cohort B (67/20) at 2.5% - but RTOG GU toxicity reporting is rare so it's hard to cross-compare (I know, cross comparison is a cardinal sin) with other microboost trials.
As for DELINEATE SABR cohort E results indicating feasibility, recruitment never continued further than n=51 cohort E because of evolving evidence, suggesting that dose escalation may not be necessary in this cohort. sciencedirect.com/science/ar…
2
1
691
Mar 22
I, too, microboost >90% of patients but often 64-67/20.
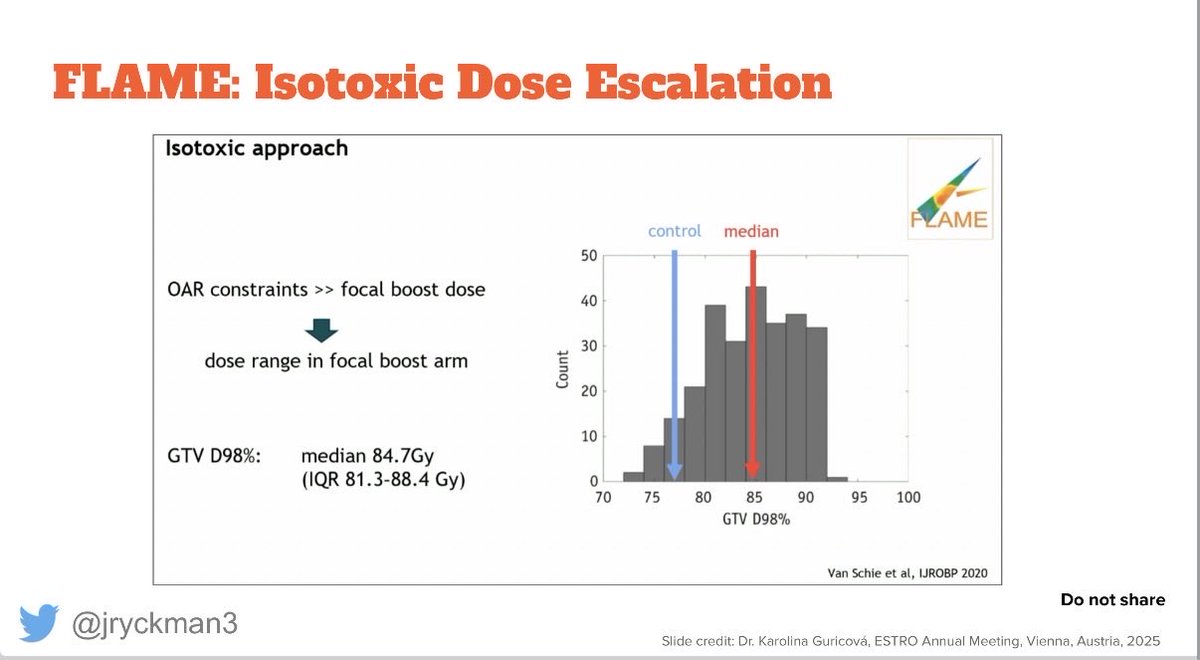
What are your thoughts on microboosting in context of 40/5 to CTV? That’s already > 100 Gy EQD2 assuming a/b of 1.5 (not that I believe the clinical validity of BED/EQD2 conversions esp in context of SBRT, nor the a/b of 1.5 for PrCa), but not sure there is additive benefit for 45/5 considering median D98 to DIL was 85 Gy on FLAME and also fantastic results without DIL boost on PACE @alison_tree
Personally I’m only offering it on trial in context of SBRT otherwise I stick with 40/5 to CTV. Ofc we know 45/5 to DIL, when done appropriately, is well tolerated. Just curious if your thoughts differ in context of SBRT and 40/5 to CTV.
2
1
6
992

Mar 21
Lindsey Buckingham...Dreams...Fleetwood Mac guitar cover. Such a talented and original songwriter and player!! This preset took a lot of research and took a while to build. You are only hearing what my phone mic is picking up. The preset is enourmous with lots of panning.
Follow me I follow back!!
for guitarists: (Fractal Axe FX 3) First block is a very much used volume block..I am swelling almost every note and chord, a drive block (microboost at just .66 boost for a little bite) plexi 50w jumped amp block (lindsey used a marshall for this song), VCA trem block 7.700 rate 80% depth traingle lfo, I also have a parallelblock above this for dry signal, my special sauce chorus block analog stereo at just 10% mix for body, a rotary block 2.281 rate, dual delay block (left) 375ms 26% fb (right) 500ms 26% fb 16.3 mix, reverb sun plate 2.40 ms 5.1% mix
(in) (vol) (drive) (amp)-(pan trem)-(cab)(chorus)(rotary)
\(empty) /
(dly)(rvb)(out 1 and 2) 1 for stage monitor 2 for front of house
#lindseybuckingham #keithwhite #fleetwoodmac #dreams #stevienicks #guitarcover
1
18
377

Mar 18
Wow this is like the old school studies that informed CTV margins in almost every disease site that were done in the 1980s-2000s. Now that prostate microboost becoming more accepted, maybe CTV margins are needed too. #radonc

How well does the size of the dominant intraprostatic lesions (DIL) correlate between #pcsm imaging and surgical pathology?
In this institutional cohort (n=48), DIL size on surgical pathology was compared to DIL size on PSMA-PET (PSMA) and multiparametric MRI (mpMRI)
🔘 Median difference in max diameter between surgical DIL and PSMA DIL was 3.4mm (IQR 16.3-24.8)
🔘 Median difference in max diameter between surgical DIL and mpMRI was 4mm (IQR 3-9)
🔘 PSMA and mpMRI, underestimated DIL size in 59% and 64% of cases, respectively
🔘 On MVA, discrepancy in size🔼 w/ 🔼PSA (PSMA, mpMRI) and 🔽 group grade (PSMA)
🔘 Further understanding of DIL size discrepancy could better inform #radoc microboosting volumes
🔗 - tinyurl.com/5n85f9az
@ASTRO_org @KamravaMD @l_ballas @AnthonyNguyenMD
3
5
17
3,156

Very cool. I’ve had some wild dream activity over the past few years. Noticeable more when I sleep on my back, accompanied by a sense that time moves slower. I think this may be because of increased REM.
I’ve had a few dreams within dreams. Where I’m lucid, and the realization either wakes me up or kicks me into another dream. Just like inception.
Once when I first injected some bpc into my shoulder, upper trap area near my neck, I went into a sleep paralysis half dream half wake state.
I also have 1 recurring dream.
Interestingly, microboost capsules from Beam Minerals before bed reliably increase my dream activity.
2
173
1 Nov 2025
I still struggle on how to apply this data, since I treat >90% of my patients as per Allison Tree's amazing DELINEATE study. I microboost nearly everyone. The realist in me feels we can extrapolate these results to microboosts regardless of technique (BT, MHFX, SBRT, CFx). I'm sure many people do in practice omit regional nodes in context of microboosts, even for high risk. Both approaches are coherent and defensible imho
2
11
804
1 Nov 2025
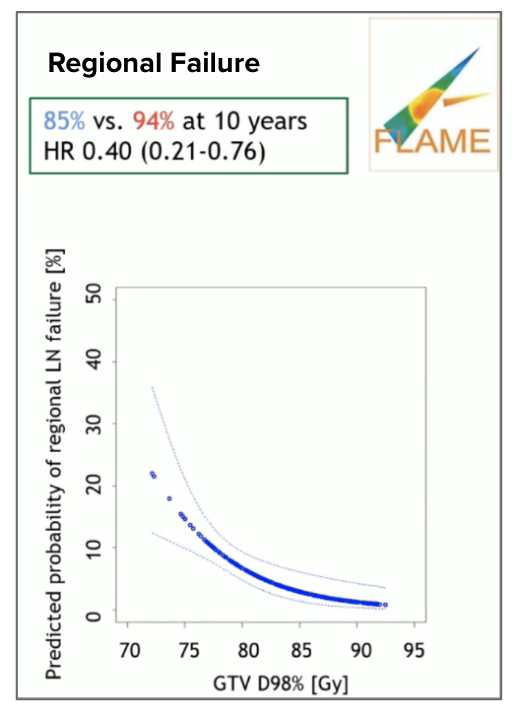
A more constructive angle on the nuance of this topic might be to discuss implications of microboosts on nodal coverage—FLAME showed 10-yr regional failure dropping from 15% → 6% (HR 0.30 [0.21-0.76]) for prostate-only RT ± microboost, with 84% of patients high-risk.
3
4
12
2,054

29 Sep 2025
🔬 Big studies being presented at the Plenary at #ASTRO25!
📌 Shannon MacDonald's presentation of "Phase III Randomized Trial of Proton vs. Photon Therapy for Patients with Non-Metastatic Breast Cancer Receiving Comprehensive Nodal Radiation: A Radiotherapy Comparative Effectiveness (RadComp) Consortium Trial: Health-Related Quality Of Life Outcomes" started out the session strong. This is the first randomized study comparing proton to photon radiation for breast cancer and its first reporting, HRQOL at 6 months was excellent and largely equivalent between treatment arms (with some FACIT items favoring protons). We look forward to future results for disease control and major cardiac events, the primary endpoints of the trial, which will be reported in about 3-5 years.
📌 David Thomson's presentation of "Primary results for the phase III trial of Toxicity Reduction using Proton Beam Therapy for Oropharyngeal Cancer (TORPEdO; CRUK/18/010)". For locally advanced OPSCC, IMPT does not reduce longterm gastrostomy dependence or severe weight loss and does not improve long-term patient reported physical quality of life or swallow function compared with IMRT. How do you reconcile these findings with the MDACC RCT?
📌 It was great to watch the "Primary Results from NRG-GU005: A Phase III Trial of SBRT vs. Hypofractionated IMRT for Localized Intermediate Risk Prostate Cancer" presentation from Dr. Ellis. SBRT to a dose of 36.25 Gy resulted in favorable bowel HRQOL compared to IMRT. Urinary HRQOL was not significantly different. There was a lack of improvement in DFS for SBRT over IMRT (biochemical failure at 3yrs was actually worse for SBRT 8% v 4%, p=0.037). Therefore, 36.25 Gy in 5 fractions may be inadequate dose and the PACE B dose of 40 Gy (to prostate) should be the foundation with the consideration of a microboost as per Hypo-FLAME.
📌 "Bladder Adjuvant Radiotherapy (BART): Clinical Outcomes from a Phase III Multicenter Randomized Controlled Trial" presented by Vedang Murthy was another key study from this session. Adjuvant RT improved LRFS and DFS without increased severe late toxicity in patients with LA-MIBC post cystectomy and chemotherapy. Potential benefit in OS is being explored in a planned individual patient data meta-analysis of randomized trials. As the discussant Brian Baumann argued, should adjuvant RT be a new standard of care along with adjuvant immunotherapy for patients with LA-MIBC?
These important studies evaluate treatment approaches to cancer and the long-term outcomes that shape how we care for patients.
@ASTRO_org @NRGonc @jmmrad @DrHowardSandler @NehaVapiwala @Doug_Radonc @ChelseaPinnix @DrChrisCorso @CurtilandD @DrMalikaSiker @catherynyashar @IBCradiation @A_CT_SimMDJD @ZacharyBWhiteII @Ggreen1986 @MorganSLevy @Hysr_Ly @NataliyaMedPhys @MustafaBasree @RadOncDoc_Niema @TheMedNet @ShannonMacDonMD @SFShaitelmanMD @VinitaTakiar @VedangMurthy @BrianCBaumann @vinaigondi @ken4englewood
#ASTRO25 #ProstateCancer #RadOnc #OncologyResearch




8
13
1,439
24 Aug 2025
Yes, I agree. I rarely face ureter as dose-limiting OAR for SBRT. Prostatic urethra, however, commonly DL OAR, esp given my practice to microboost. I would imagine urethra is similarly impacted by RT exposure as ureter. In such cases, I plan w/ urethra PRV02 avoidance regions.
2
5
540