G retweeted

Jun 13
NEW - Laser Multi Region DVD Player
ow.ly/iY1u50Oju9f
#New #HecticGifts #Laser #MultiRegion #DVDPlayer #RegionFree #Australian #HecticGifts #Freeshipping #AustraliaWide #FastShipping

1
1
2
8

Deseamos....pero será "multiregion" hace tiempo compré la película de Daft Punk versión japonesa y nunca la pude ver😭😭
1
6
G retweeted
Jun 9
NEW - Laser Multi Region DVD Player
ow.ly/iY1u50Oju9f
#New #HecticGifts #Laser #MultiRegion #DVDPlayer #RegionFree #Australian #HecticGifts #Freeshipping #AustraliaWide #FastShipping

1
1
19

is there really creativity? any story lines anymore...or 1 thats lasted 3 years we are bored to death with... Its just not the same as 80s multiregion 90s same and wwf dominance that had us tuning in for next chapters on multi stories every week. when dream match is.. no build
14
G retweeted
Jun 7
NEW - Laser Multi Region DVD Player
ow.ly/iY1u50Oju9f
#New #HecticGifts #Laser #MultiRegion #DVDPlayer #RegionFree #Australian #HecticGifts #Freeshipping #AustraliaWide #FastShipping

1
1
6

May 25
Meet the YugabyteDB team at the @awscloud Summit in Los Angeles and discover #AI-native, distributed #YugabyteDB - built for global #scalability, #multiregion #consistency, and ultra-low #latency! 🚀
📆AWS Los Angeles - 10 June📆
Stop by the booth to win cool prizes and chat with database experts. Schedule a personalized meeting to discover how you can build fast, run anywhere, and survive anything!💡
na2.hubs.ly/H05GkXX0

2
161

May 20
Cross-Region構成の本当の難しさは「動く構成」と「説明できる構成」の乖離です。
山崎行政書士事務所は、技術者と共同で以下を支援:
Storage GRS / RA-GRS / ZRS とデータ境界の関係
SQL Geo-Replication のPrimary/Secondaryで発生する越境
AIサービス使用時のデータ保持ポリシー分析
リージョン間転送ログと監査証跡(Activity / Diagnostic)
GDPR Art.44–49 / SCC / TIA との整合性評価
取引先監査に提出できるデータフローマップ作成
“構成が国境を越える前に、リスクが越境していないか”をチェックします。
#AzureArchitecture #MultiRegion #GDPR #DataFlow #監査対応

5
91

May 20
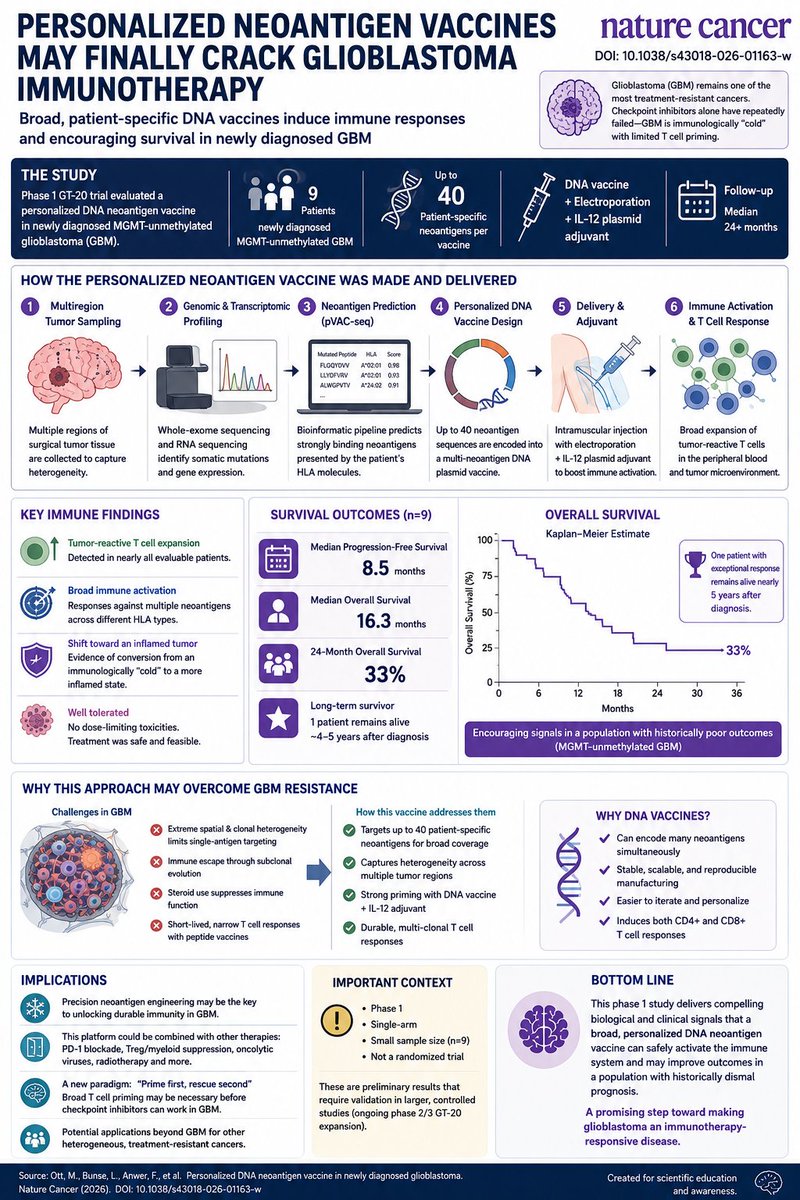
🧠 Personalized Neoantigen Vaccines May Finally Crack Glioblastoma Immunotherapy
For decades, glioblastoma (GBM) has remained one of oncology’s greatest failures for immunotherapy.
Checkpoint inhibitors revolutionized melanoma and lung cancer.
CAR-T showed flashes of promise.
Peptide vaccines generated excitement.
But GBM kept winning.
Now a new Nature Cancer study may point toward a fundamentally different strategy: ➡️ highly personalized, broad-spectrum neoantigen vaccination.
In the GT-20 phase 1 trial, researchers developed individualized DNA vaccines encoding up to 40 patient-specific tumor neoantigens for newly diagnosed MGMT-unmethylated GBM — among the most treatment-resistant brain tumors.
This was not a “one antigen fits all” approach.
Each patient underwent: • multiregion tumor sequencing
• neoantigen prediction using pVAC-seq
• custom plasmid vaccine manufacturing
• intramuscular electroporation delivery
• IL-12 adjuvant stimulation
The goal was simple but ambitious:
Generate a sufficiently broad T cell response to overcome GBM heterogeneity and immune escape.
And remarkably, it worked biologically.
The vaccine induced: 🔥 expansion of tumor-reactive T cell clones
🔥 broad peripheral immune activation
🔥 durable antigen-specific responses
Most importantly, the therapy appeared capable of shifting GBM from an immunologically “cold” tumor toward a more inflamed immune state.
That matters enormously.
Many believe GBM immunotherapy failed not because checkpoints are irrelevant, but because there are too few pre-existing antitumor T cells for checkpoint blockade to rescue.
In other words: No priming → no checkpoint efficacy.
This platform may solve the priming problem first.
Clinical outcomes remain preliminary: • Median PFS: 8.5 months
• Median OS: 16.3 months
• 24-month survival: 33%
• One patient survived nearly 5 years
Importantly, this was:
Phase 1
Single-arm
n=9
So this is NOT proof of efficacy.
But mechanistically, these signals are unusually compelling for GBM.
Another critical point: the platform used DNA vaccines rather than peptide vaccines.
That enables: • larger neoantigen payloads
• scalable manufacturing
• iterative redesign
• broader epitope coverage
This could become especially powerful when combined with:
PD-1 blockade
Treg/myeloid suppression
oncolytic viruses
radiotherapy-induced antigen spreading
The broader implication extends beyond GBM.
This study reinforces an emerging principle in cancer immunotherapy:
The future may belong not to generic immune activation — but to precise, patient-specific neoantigen engineering.
In highly heterogeneous tumors, breadth may matter as much as intensity.
DOI: 10.1038/s43018-026-01163-w
4
208


May 8
Kube-native AI-first Enterprise-ready RBAC-supporting multiregion Vibe-coded self-rolled auth system
6
1
20
790


Apr 19
From a single market to multi-region collaboration,BAF is bringing trading into a new stage.
#GlobalExpansion #MultiRegion #TradingInnovation

3
289
10,575

Apr 14
Contabo offers 11 data center worldwide - and for a limited time, lower location fees.
EU, US, UK and more - move your infrastructure closer to your users for lower latency and snappier sites 👉 ow.ly/7afE50YzAG6
#DataCenters #MultiRegion #VPSHosting #VDSHosting

1
5
422

ah males ada vibe coder hasil asal asalan, jadi sampah internet
1. Scalability udh dipikir blm, flashsale diakses 2 milyar orang kuat?
2. Multiregion failover? aws uae kena rudal apa ada DR? bisa jamin SLA gak
3. Arsitektur microservice atau monolith?
3. Rust/go? jgn2 cuma php?
3
2
755

Venta de sega naomi con marvel vs capcom 2 con bios multiregion con esta le puedes cambiar la region al juego incluye cables naomi y io board el precio es de 10 mil pesos mando fotos y videos


2
6
65
2,828

This is concerning
I might have to end up grabbing a Multiregion blu ray player and start importing anime I want
2
354

Mar 14
Lo que dices no tienen ningún sentido, solo están atacando a una región, podrías tener todo en multiregion sin tener que usar multiplataforma…
Pero claro eso no vende servidores locales…
1
33
4,552