
What are the negative effects of kudzu?
In the industrial use of kudzu extract, the formulation-related limitations, variability, and possible compatibility problems of the Kudzu Extract should be considered.
nutragreen-extracts.com/info…
1

Das meinte ich. Auch Ihre Abbildung könnten wir da gemeinsam verstehen lernen wie die Unterschiede von unforced variability vs. forced trends. Wieso endet die Temperature eigentlich in 2008?

Sie sollten zu Ihrer Konferenz lehrende Grundlagenforscher der atmosphärischen oder planetaren Physik einladen. Dann gehen wir gemeinsam Seite für Seite durch das Lehrbuch und Sie sagen uns dann, ab wo es hakt (z.B. wo die 1/4 in der Strahlungsgleichung herkommt).
3

Research shows that this breathing frequency maximizes heart rate variability (HRV), a key indicator of high vagal tone and resistance to stress.
(TO BE CONTINUED...)
11

Missing values in your data are always problematic, but how problematic they become depends heavily on the underlying missing data mechanism.
The visualization below compares three common response mechanisms:
🔹 MCAR (Missing Completely at Random)
🔹 MAR (Missing at Random)
🔹 MNAR (Missing Not at Random)
For each mechanism, the visualization gradually increases the proportion of missing values and compares how strongly the estimated mean of the target variable deviates from the true value.
Two important patterns become visible:
🔹 MCAR produces essentially unbiased estimates, while MNAR leads to the strongest bias.
🔹 As the percentage of missing values increases, both the bias (for MAR and MNAR) and the variability of the estimates become larger.
Of course, the severity of these effects depends not only on the type of missing data mechanism, but also on how strongly the missingness process is related to the data itself. Nevertheless, I think this example illustrates quite well that different missing data mechanisms can lead to very different levels of risk.
This is one of the key reasons why handling missing data correctly is so important in practical data analysis.
I have just published a brand-new module in the Statistics Globe Hub covering this topic in detail, including practical examples in R. The Statistics Globe Hub is my ongoing learning program focused on practical skills in statistics, data science, AI, and programming with R and Python.
More information about the Statistics Globe Hub: statisticsglobe.com/hub
#rstats #datascience #statistics #MissingData #DataScience #MachineLearning #MonteCarlo #ggplot2 #DataAnalysis #StatisticsGlobeHub
3
30


More than tenfold the anticipated clinical dose range. That is the safety margin Entera tested for EB618, its oral GLP-1/glucagon dual agonist tablet, in non-human primates, with no adverse findings at any tested level.
The standard approach in the obesity space is to take a GLP-1 agonist that works as an injection and find a way to make it oral. Oxyntomodulin takes a different route. It is a naturally occurring dual GLP-1/glucagon receptor agonist with documented effects on appetite, weight, and glucose metabolism, plus cardioprotective and anti-fibrotic properties that pure GLP-1 agonists do not carry.
At ENDO 2026, $ENTX reported that EB618 showed dose-proportional pharmacokinetics across three tablet strengths in a non-human primate study, with low variability. The pharmacodynamic signal tracked the PK cleanly: dose-proportional effects on postprandial blood glucose at each strength tested.
The EB618 program runs in parallel with a subcutaneous OXM Phase 1 SAD/MAD study being planned by OPKO Health, with data expected by end of 2026. The oral tablet IND is gated behind that study.
Watch for the OPKO subcutaneous OXM Phase 1 data readout: it is the upstream clinical validation that will frame the oral EB618 IND filing.
globenewswire.com/news-relea…
_
Paid Ad via #WallStWire: This account is operated by Wall Street Wire. Entera Bio Ltd. or a related party has paid Wall Street Wire for ongoing promotional services. Full compensation and paying party disclosure: wallstwire.ai/disclosures. Our content is not financial advice.
2

7/
Could technical replicates help? Sometimes, but Biological replicates reflect real-world variability. That’s what journals and reviewers expect.
1
4
3/
But there’s a catch: only one sample per condition. No replicates. No way to measure variability. No way to trust the result.
1
6
Speech, Language and Hearing Laboratory (SLHlab) retweeted

A highlight from our current issue: Hunter and Berardi (2026). Embracing variability: toward proactive and precision-based voice science. Logopedics Phoniatrics Vocology 51(1), 60-68. doi.org/10.1080/14015439.202… #LPV @tandfnewsroom @tandfonline

1
1
6

22m
Vagus HRV Golden
(Not A Dr-.-xD)
Education/Entertainment
Song/Idea/Guess/Suno/Ai
Verse 1 (Gentle Building Flow Inline Lens Stack)
Diaphragmatic deep, vagus nerve sings
Stack: Parasympathetic activation (science: HRV ↑, inflammation ↓) → emotional safety (psych: IFS protector parts relax) → archetype rewrite (fringe: dissolve Anu-layer fear scripts) → energetic expansion (visualize golden light spiraling DNA).
Heart rate variability, coherence it brings
Stack: Measurable cardiac coherence (HeartMath science) → felt equanimity (interoception) → reality authoring via calm baseline (Neville/Goddard lens) → collective resonance (All for All field).
Neuroplastic rewiring, pathways ignite
Stack: BDNF upregulation, new synapses form (cellular) → habit deprogramming (mental) → forgiveness embodiment (Ho’oponopono echo in scientific form) → fractal visualization of luminous neural nets.
Mitochondria glow, cellular light
Stack: ATP surge ROS signaling (bioenergetics) → vitality feeling of warmth/expansion (sensory) → epigenetic expression shift (fringe wave-genetics compatible) → sovereign cellular consciousness.
Pre-Chorus (Repetitive Anchor Quick Lens Layers)
Breathe in… Oxygen… Energy… Flow…
Stack: Hemoglobin binding → mitochondrial fuel → felt surge → visualized light codes → authored abundance.
Breathe out… Carbon… Tension… Let go…
Stack: Detox exhale (physiology) → emotional release (feelings) → archetype shedding (psych) → field cleansing (collective).
Interoception rising, feelings reveal
Stack: Gut-brain axis signaling (science) → truth beyond thought (awareness) → body as oracle (fringe/personal).
Chorus – Scientific Power Stack (Repeat 3x, Layered Vocals Explanatory Echoes)
Oxygenate, Regenerate, Cohere, Align
Stack: O₂ saturation (blood) → tissue repair (cellular) → HRV coherence (autonomic) → multi-system integration (whole being) visualize fractal golden spiral, feel warmth rise, smell pine BVOCs.
Neuroplastic, Vagal Tone, Homeostasis shine
Stack: Brain rewiring (neuro) → vagus calming (nerve) → dynamic balance (physiology) → emotional stability archetype harmony → collective equilibrium.
Epigenetic flow, Resonance grow
Stack: Gene expression tuning (science) → wave/linguistic fields (Gariaev fringe) → vibrational medicine (432Hz) → felt expansion reality authoring.
Autonomic balance, Infinite glow
Stack: Sympathetic/parasympathetic harmony → sovereign presence → infinite creators lens (All for All) → smell earth grounding, visualize light body.
Verse 2 (Deeper Sensory Multi-Level Integration)
Box breath hold, nitric oxide surge
Stack: Vasodilation (science) → improved circulation/oxygen delivery (body) → calm confidence (emotion) → archetype of the Warrior-Breather.
Lungs expand, interoceptive merge
Stack: Diaphragm stretch → full sensory feedback loop (feelings) → visualization of light filling thoracic cavity → energetic heart-lung coherence.
Visualize the light codes, DNA transcription pure
Stack: Photobiomodulation analogy (science) → wave-genetics activation (fringe) → mental clarity emotional forgiveness echo.
Smell the earth grounding, barefoot and sure
Stack: Grounding electrons (earthing science) → olfactory bulb calming (neuro) → felt safety pine terpenes for focus.
Feel the equanimity, calm wave arise
Stack: Default mode network quieting → present-moment awareness → collective liberation field.
suno.com/s/Am611VnQNpvwLPnh
12

Because the 2nd person of the Trinity was speaking to the first person while incarnate.
On Trinitarian ontology, God is 1 tri-personal being; He is one living immaterial conscious entity whose mind has 3 egos that are each:
a referent for a 1st person indexical “I”,
a center of self-consciousness
a concrete second-order personal faculty of the divine mind
a faculty that can identify psychological properties as “mine” & enable God to have 3 complete separate psychological personal identities
a hypostasis which is what the term “person” refers to in Trinitarian discourse
Jesus Christ is one person with two natures. On this model, this means He has two souls but only one ego: the 2nd divine ego (the Logos) is eternal because it is a necessary concrete constituent of the eternal divine soul, and is hypostatically united to an en-hypostatic human soul. This human soul is ego-less in itself. The Logos serves as its ego, thereby completing & personalizing it as a full human nature.
Any mind that has mental states has cognitive faculties & capacities that enable it to have those mental states.
Intellectual faculties allow a mind to have thoughts
Volitional faculties create desires
Noetic faculties sustain beliefs
Affective faculties, emotions
Perceptual faculties, sensations
Memorial faculties, memories
Thoughts, beliefs, emotions, sensations, desires, these are all mental states & modes that a mind has.
2nd order mental states are mental states that have other mental states or mental faculties as their objects. So a thought about a thought; a belief about a belief; a desire to have desires; etc. these are all examples of second order mental states and they require the mind to have a second order cognitive faculty called an Ego, which is also the referent of first-person indexicals thoughts (“I”/“me” thoughts); it is what allows a mind to have awareness of itself and its contents.
Rational faculties make the mind rational, & they require the existence of an ego, because a 2nd order faculty is required to exercise Conceptual faculties, since concepts are abstracted from other mental states like sensations. An ego is also a necessary condition for having a psychological personal identity which is a set of psychological properties (like memories, desires, beliefs, personality, values, sense of self, and so forth) which form who I am.
Now psychological personal identity cannot be the ultimate determinant of my identity because these psychological states must first be identified as MINE, by ME as a subject who owns them, before they can fulfil any role of determining who I am. But this presupposes my ontological personal identity: my existence as an individual self/ego/person who has psychological properties. This can only be established by an ego within a soul for at least two reasons. First a soul is a mereologically simple entity that is not made of separable parts. Thus has the required unity to both contain AND be a suitable referent of 1st person indexicals which are the logically proper name of a primitive, unanalyzable entity that does not admit degree, or change, and is known by direct acquaintance, the self. Second the ego is also the only ultimate referent of 1st person indexicals since it is the reflexive 2nd order faculty that identifies the psychological properties within the soul as mine, and serves as the ultimate stopping point of the contextual variability of first-person indexicals.
So while humans have one ego in their mind, God has 3. Each is a referent for a 1st person indexical “I”, meaning that each is concrete second-order personal faculty of the divine mind which is a center of self-consciousness & enables God to be one soul with 3 complete psychological personal identities & thus there is no contradiction
1
7

**Onset (Launch) of Symptoms vs. Everyday / Progressive Symptoms in Huntington’s Disease (HD)**
Huntington’s disease is **progressive** — it starts subtly and worsens over time (typically 10–30 years from symptom onset to end stage, faster in juvenile cases). The **onset** refers to the initial, often mild signs when the disease becomes noticeable. **Daily/ongoing symptoms** are what people experience as the disease advances, becoming more severe and constant.
### Key Differences
| Aspect | **Onset / Early Symptoms** (Launch) | **Daily / Progressive Symptoms** (As Disease Advances) |
|-------------------------|-----------------------------------------------------------------------------------------------------|-------------------------------------------------------------------------------------------------------------------------|
| **Timing** | Usually appears in 30s–50s (adult-onset); can be earlier in juvenile HD. Subtle changes may precede obvious signs by years. | Worsens gradually over years. Symptoms become constant, more intense, and interfere heavily with daily life. |
| **Main Features** | Mild and intermittent. Often noticed first by others. | More severe, constant, and multifaceted (motor cognitive psychiatric). |
| **Motor Symptoms** | Subtle clumsiness, mild coordination issues, small twitching/jerking (early chorea), balance problems. | Prominent **chorea** (involuntary jerky movements), later replaced by rigidity, stiffness, bradykinesia (slowness), swallowing/speech difficulties, falls, and eventual immobility. |
| **Cognitive Symptoms** | Mild difficulty concentrating, planning, multitasking, or slight memory issues. | Progressive dementia-like decline: severe executive dysfunction, memory loss, poor judgment, inability to manage daily tasks. |
| **Psychiatric/Behavioral** | Irritability, mood swings, mild depression, anxiety, apathy, personality changes. | More intense and persistent: depression, aggression, apathy, obsessive behaviors, psychosis. Harder to manage later due to communication loss. |
| **Functional Impact** | People can usually continue working, driving, and living independently. | Loss of independence: inability to work/drive, need assistance with daily activities, eventually full-time care. |
| **Variability** | Symptoms vary widely between people; some start with mood changes, others with mild movements. | All three domains (motor, cognitive, psychiatric) become heavily affected, though the order and severity differ. |
### Summary of Progression (Typical Adult-Onset HD)
- **Prodromal / Very Early (before clear diagnosis)**: Subtle cognitive or psychiatric changes (e.g., irritability, mild executive issues) can appear 10–20 years before motor signs.
- **Early Stage (Onset)**: Mild symptoms; person remains largely functional.
- **Middle Stage**: Chorea becomes prominent, daily tasks become difficult, increased falls and weight loss.
- **Late Stage**: Severe disability — often nonverbal, bedridden, full dependence. Chorea may decrease and be replaced by rigidity.
**Important notes**:
- **Juvenile HD** (onset before age 20) often starts differently: more rigidity, bradykinesia, cognitive decline, and seizures, with faster progression.
- Symptoms and order vary greatly between individuals. Not everyone gets severe chorea.
- The **striatum** (basal ganglia) is damaged first, which explains why motor and timing/coordination issues (relevant to activities like jump rope) appear early and worsen.
If you’re asking in the context of exercise (e.g., jump rope vs. running/walking), early-stage patients can often benefit from rhythmic/coord
7
Chidambara .ML. retweeted

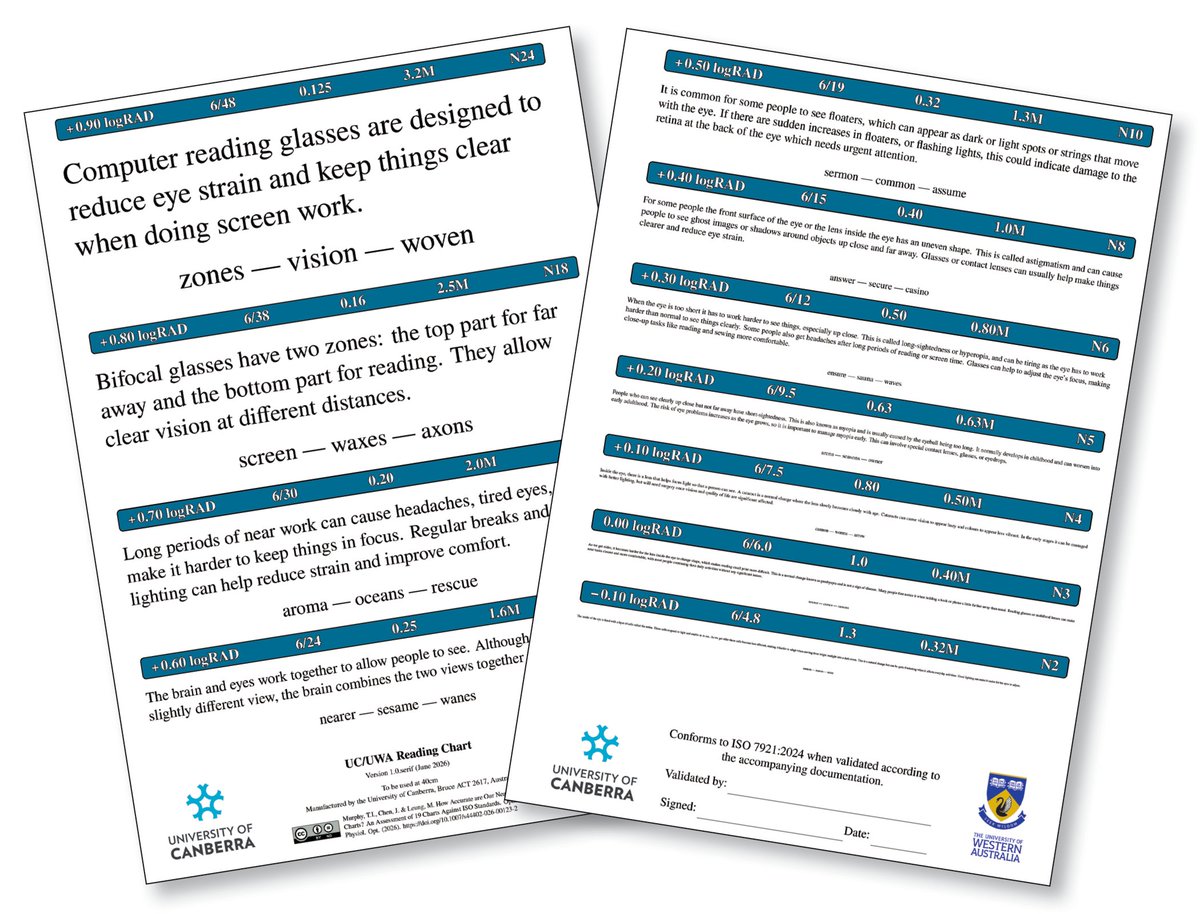
No Near-Reading Charts Met International Standards in Multi-Product Study
Researchers found variability between fonts, text sizes and materials, impacting results.
reviewofoptometry.com/articl…
#optometry #optometrist #eyecare #test #readingacuity
2
166
On Trinitarian ontology, God is 1 tri-personal being; He is one living immaterial conscious entity whose mind has 3 egos that are each:
a referent for a 1st person indexical “I”,
a center of self-consciousness
a concrete second-order personal faculty of the divine mind
a faculty that can identify psychological properties as “mine” & enable God to have 3 complete separate psychological personal identities
a hypostasis which is what the term “person” refers to in Trinitarian discourse
Jesus Christ is one person with two natures. On this model, this means He has two souls but only one ego: the 2nd divine ego (the Logos) is eternal because it is a necessary concrete constituent of the eternal divine soul, and is hypostatically united to an en-hypostatic human soul. This human soul is ego-less in itself. The Logos serves as its ego, thereby completing & personalizing it as a full human nature.
Any mind that has mental states has cognitive faculties & capacities that enable it to have those mental states.
Intellectual faculties allow a mind to have thoughts
Volitional faculties create desires
Noetic faculties sustain beliefs
Affective faculties, emotions
Perceptual faculties, sensations
Memorial faculties, memories
Thoughts, beliefs, emotions, sensations, desires, these are all mental states & modes that a mind has.
2nd order mental states are mental states that have other mental states or mental faculties as their objects. So a thought about a thought; a belief about a belief; a desire to have desires; etc. these are all examples of second order mental states and they require the mind to have a second order cognitive faculty called an Ego, which is also the referent of first-person indexicals thoughts (“I”/“me” thoughts); it is what allows a mind to have awareness of itself and its contents.
Rational faculties make the mind rational, & they require the existence of an ego, because a 2nd order faculty is required to exercise Conceptual faculties, since concepts are abstracted from other mental states like sensations. An ego is also a necessary condition for having a psychological personal identity which is a set of psychological properties (like memories, desires, beliefs, personality, values, sense of self, and so forth) which form who I am.
Now psychological personal identity cannot be the ultimate determinant of my identity because these psychological states must first be identified as MINE, by ME as a subject who owns them, before they can fulfil any role of determining who I am. But this presupposes my ontological personal identity: my existence as an individual self/ego/person who has psychological properties. This can only be established by an ego within a soul for at least two reasons. First a soul is a mereologically simple entity that is not made of separable parts. Thus has the required unity to both contain AND be a suitable referent of 1st person indexicals which are the logically proper name of a primitive, unanalyzable entity that does not admit degree, or change, and is known by direct acquaintance, the self. Second the ego is also the only ultimate referent of 1st person indexicals since it is the reflexive 2nd order faculty that identifies the psychological properties within the soul as mine, and serves as the ultimate stopping point of the contextual variability of first-person indexicals.
So while humans have one ego in their mind, God has 3. Each is a referent for a 1st person indexical “I”, meaning that each is concrete second-order personal faculty of the divine mind which is a center of self-consciousness & enables God to be one soul with 3 complete psychological personal identities & thus there is no contradiction
10

27m
CGM adds shape. CGM = continuous glucose monitor data. It shows overnight drift, dawn rise, post-meal peaks, and variability across 7-14 days.
1
1

Atomera (NASDAQ: ATOM) has developed a patented process technology called Mears Silicon Technology (MST). The core idea is that MST can be inserted into existing CMOS production lines to improve transistor performance and power efficiency. What makes it interesting is that it can be done using equipment the fabs already own, without requiring major new capital investment from the foundry.
Disclosure: This is not investment advice. I do not currently hold a position in ATOM. I will not trade the stock for 5 business days after this post. Atomera is a highly speculative small-cap stock with significant risk of loss, including the potential for total loss of capital. Do your own research. The author assumes no liability for any losses resulting from the use of this information.
The Technology
MST is fundamentally an epitaxy process. While growing ultra-thin layers of single-crystal silicon on a wafer using Reduced Pressure Chemical Vapor Deposition (RPCVD), Atomera interrupts the growth at precise intervals and inserts partial monolayers of oxygen atoms in controlled, repeating patterns. This creates a “superlattice” inside the silicon at the atomic scale.
That engineered superlattice changes how electrons move, scatter, and interact within the transistor channel.
The claimed benefits include higher electron and hole mobility (faster switching), reduced leakage current when the transistor is off, lower variability between transistors on the same chip, and improved long-term reliability due to reduced charge trapping and degradation.
Because the MST process runs inside existing epi tools, foundries don’t need to buy new equipment. They only need to adjust gas flows, temperature, and pressure recipes. Atomera is also working with major equipment makers to make integration smoother. The end result is still pure silicon, just with engineered atomic-level oxygen interruptions that integrate with the rest of the CMOS flow.
Atomera doesn’t sell hardware. They operate a licensing and services model. Customers can buy evaluation wafers and engineering support to test the technology. They can pay for integration and development work to qualify MST on their specific nodes. Once qualified, customers pay an upfront license fee plus ongoing royalties (low single-digit percentage of the selling price of chips made using MST). They also have an extensive patent portfolio and proprietary process recipes that can be licensed.
The Valuation
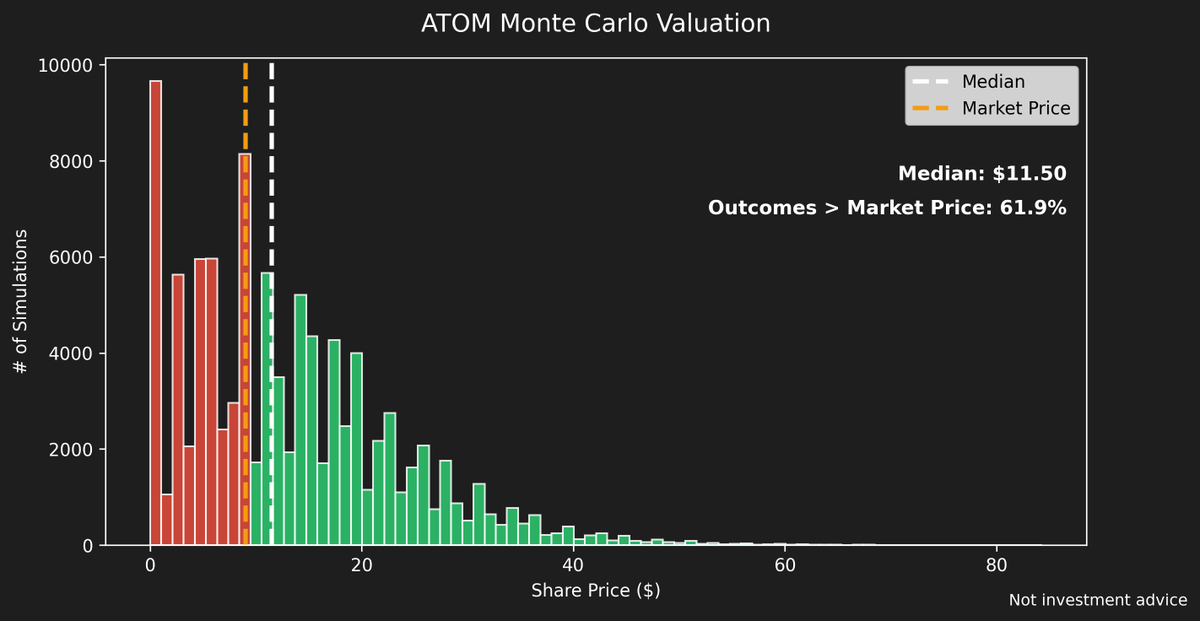
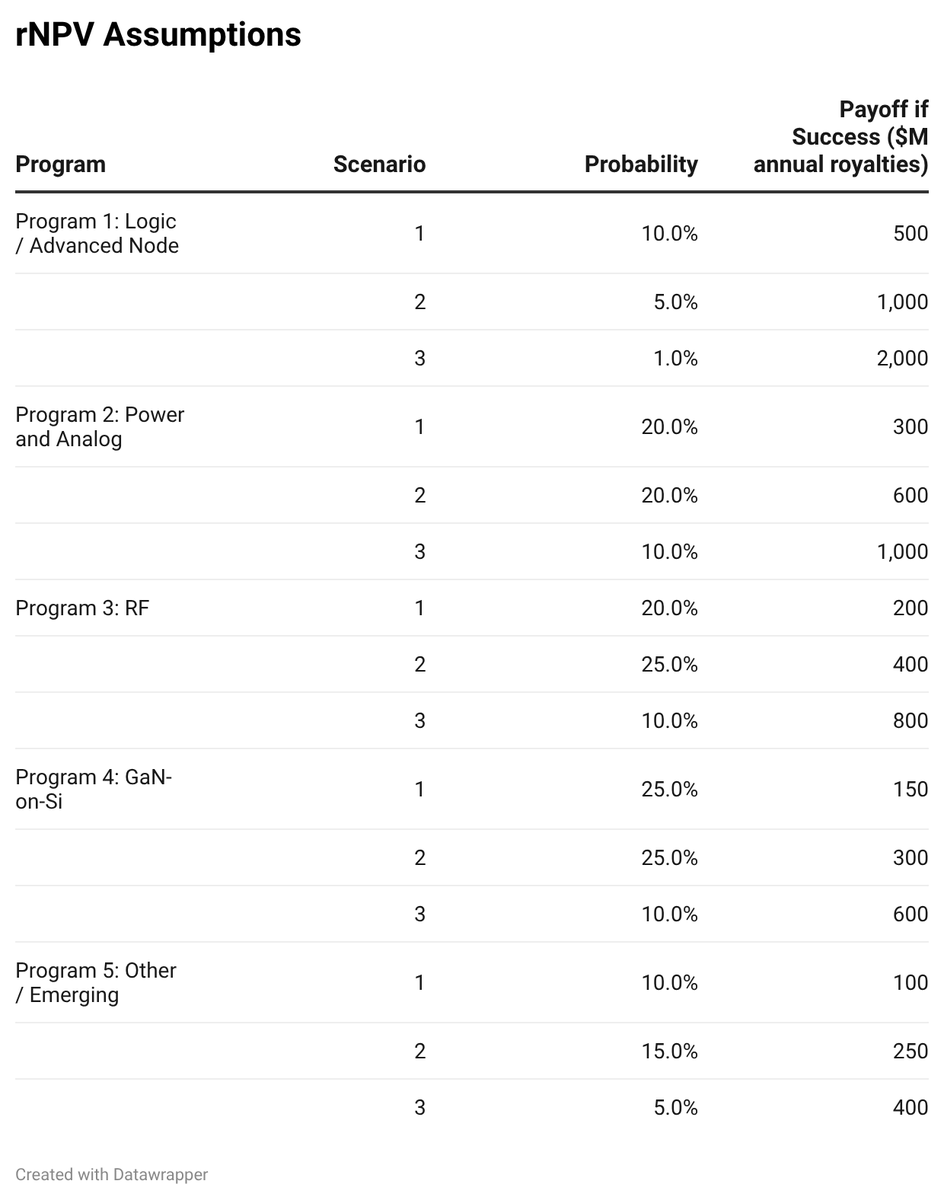
Valuing a pre-revenue company like this is difficult with traditional DCF models. I built a risk-adjusted net present value (rNPV) framework across five potential markets where MST could be adopted: advanced logic nodes, power and analog, RF, GaN-on-silicon, and a catch-all “other” category for unknown future applications.
For each market I modeled low, base, and high penetration scenarios, assigned probabilities of success, and estimated potential royalty capture (assuming 0.5–2% royalties on a meaningful portion of the TAM). I then ran a Monte Carlo simulation with 100,000 iterations, allowing programs to randomly succeed or fail (only one scenario per program could hit in any given run). I applied an 11% WACC and assumed a 5-year realization timeline for each program.
The simulation produced a median outcome above Atomera’s current share price (around $9 at the time of analysis). However, roughly 40% of outcomes were money-losing, and a significant portion were near-total losses. The upside appears when multiple programs succeed, showing multibagger potential. The downside is material if the company fails to convert integration work into actual high-volume manufacturing licenses.
Atomera remains a high-risk, early-stage company. Key risks include long qualification and sales cycles with no guarantee of conversion to production, ongoing cash burn and future shareholder dilution, the extremely risk-averse nature of foundries (technical success does not always lead to adoption), competition from established wide-bandgap technologies and incremental silicon improvements, customer concentration, and the usual intellectual property risks that come with any process technology play.
The Bottom Line
Atomera is a company worth watching closely, but I don’t view it as a compelling investment at current levels. The technology is genuinely interesting and the addressable markets are broad, but the risk/reward profile is still too much of a coin toss. The smartest approach right now is patience monitor for meaningful customer wins or manufacturing license announcements and re-evaluate if those materialize. The odds of being late to any real catalyst are relatively low given how unknown this ~$300M market cap name still is.
27

Optimizing oncology dosing isn’t just about efficacy it’s about balancing exposure, safety, and variability with a data-driven approach. In our webinar, FDA experts Hao Zhu & Brian Booth discuss modern dose optimization strategies. Watch on demand: simulations-plus.com/events/…

10

New NHANES analysis just published examined >20 years of biomarker trends in the U.S. population.
One notable finding:
Average vitamin D status increased substantially between 2001–2002 and 2021–2023, likely reflecting changes in awareness, supplementation, and monitoring.
To me, one of the most important takeaways is broader than vitamin D itself:
Public health messaging, clinical practice, supplementation behavior, and biomarker surveillance can meaningfully shift population-level nutritional status over time.
At the same time, the paper also highlights persistent variability across populations, ongoing disparities, and the continued need for individualized approaches and evidence-based implementation.
Important contribution from NHANES/CDC researchers.
Read the article: 🔗 zurl.co/aN8ky
#VitaminD #NHANES #PublicHealth #NutritionScience #IntegrativeMedicine #FunctionalMedicine #Wellness

14

34m
If someone is in an elite arena there would be less variability in talent because the variability was pre-sorted.
4