
29 May 2025
Happy to share our editorial discussing how to prevent future AT by overcoming residual conduction 🫀⚡️ ATs need more attention 🫵🏼 @C_Meyer_MD @shivkumarmd @JACCJournals @AGEP_DGK @EHRAPresident @th3k4ty @AlkenMD #ablateAT
📎authors.elsevier.com/a/1lAVP…
3
16
43
10,086

5 Oct 2024
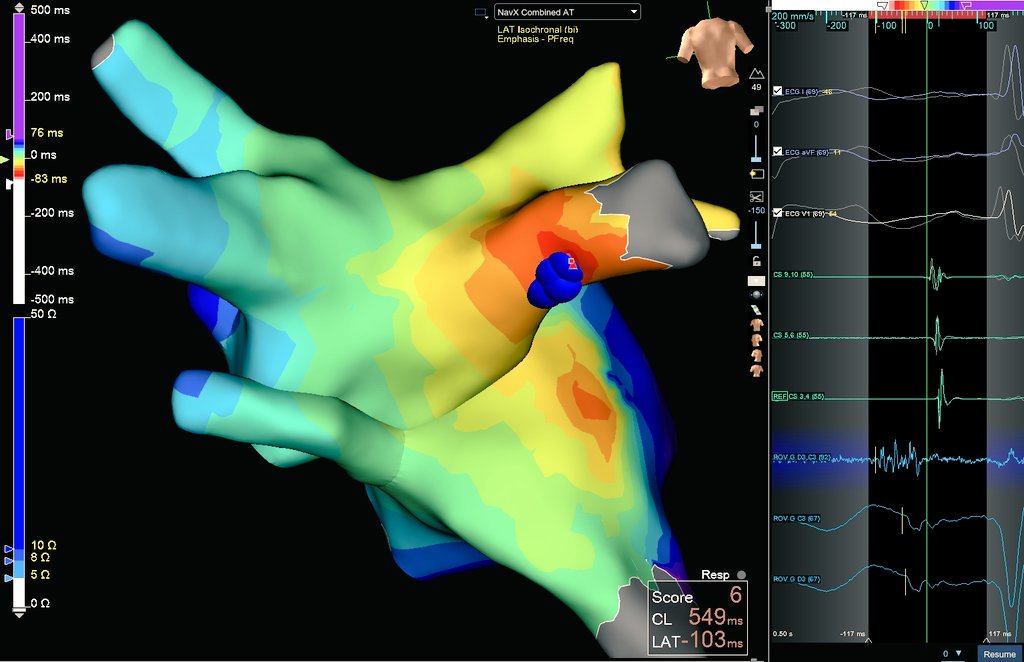
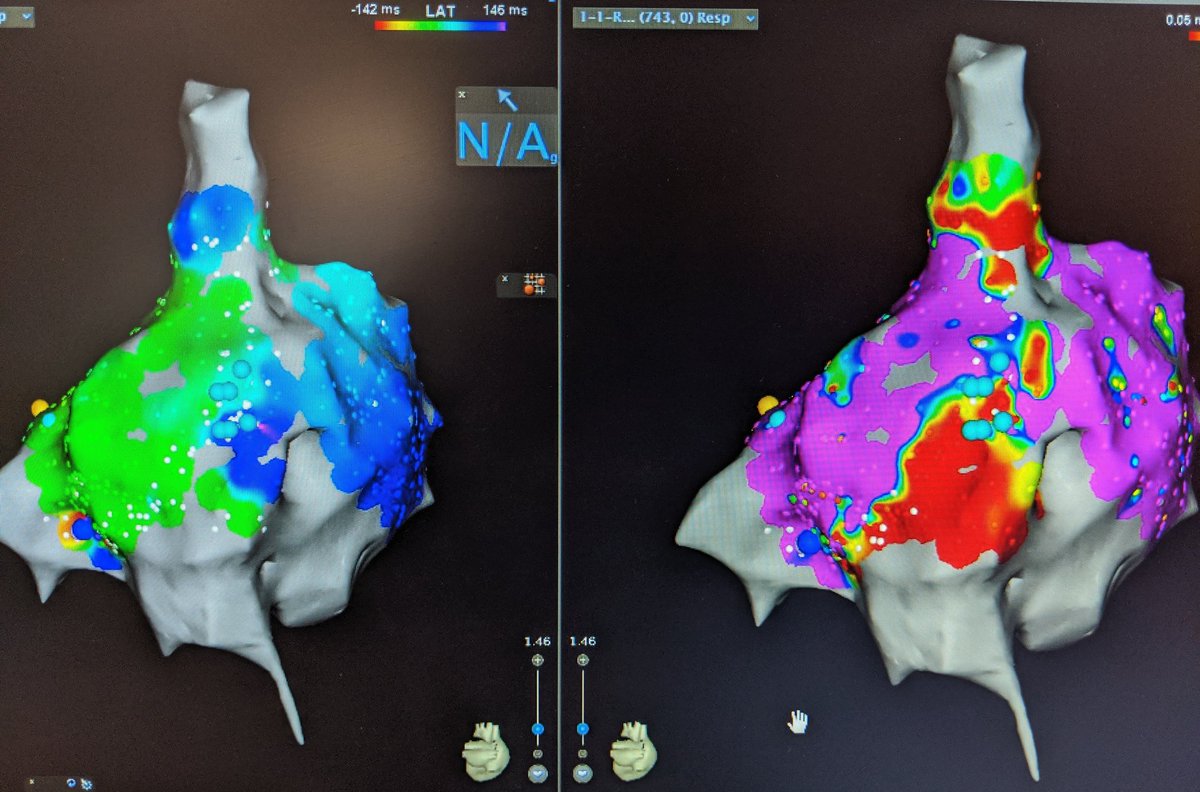
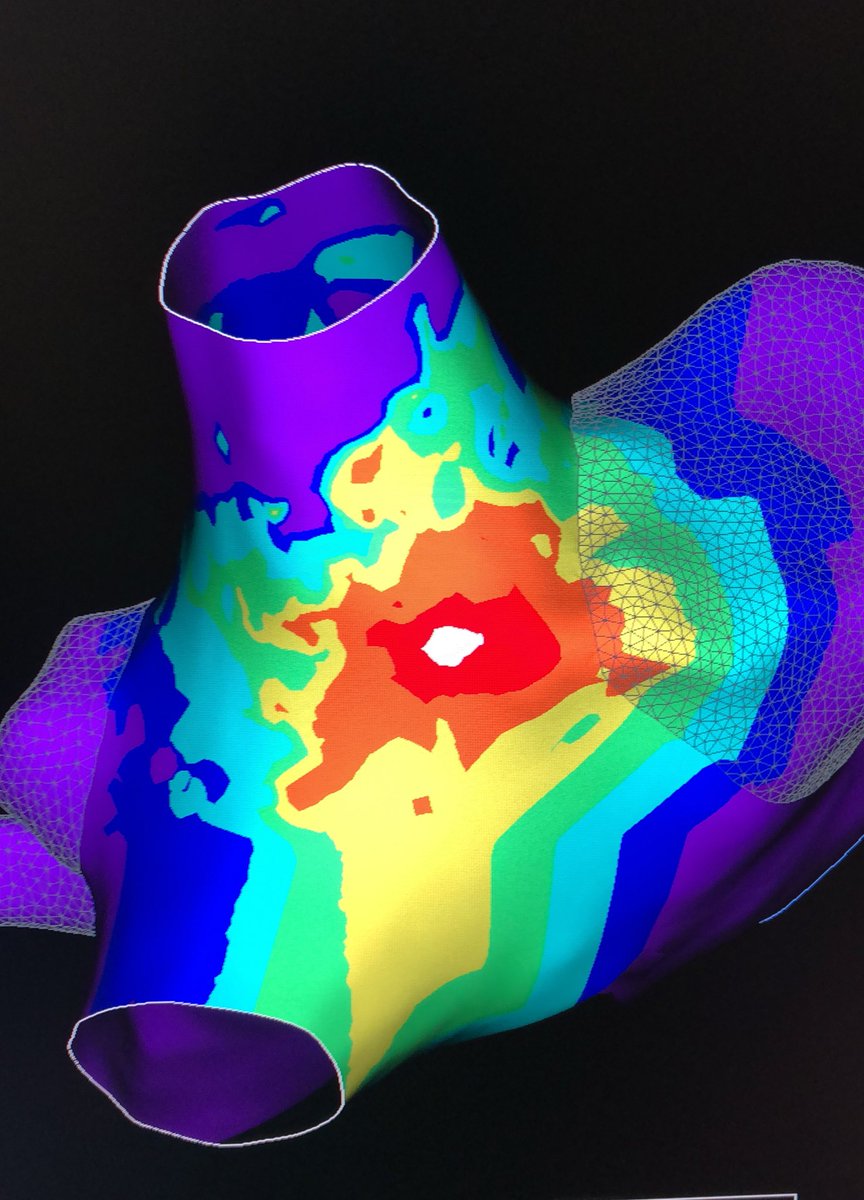
We chose focal ablation! RF in the earliest location (inferior RIPV os) eliminated all PACs, and the AT was subsequently non-inducible. ❤️🔥 Did we choose the right method? Poll below. #AblateAT
6
7
1,342
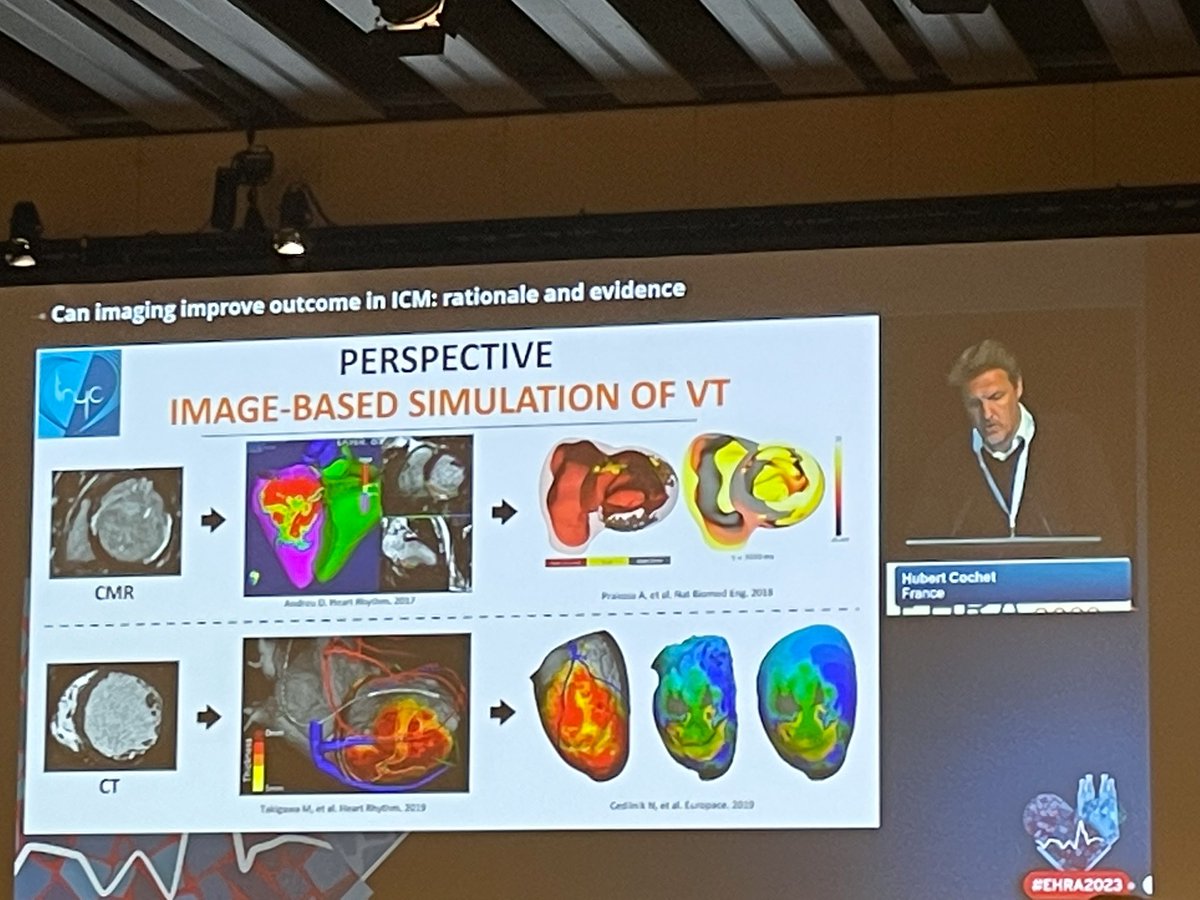
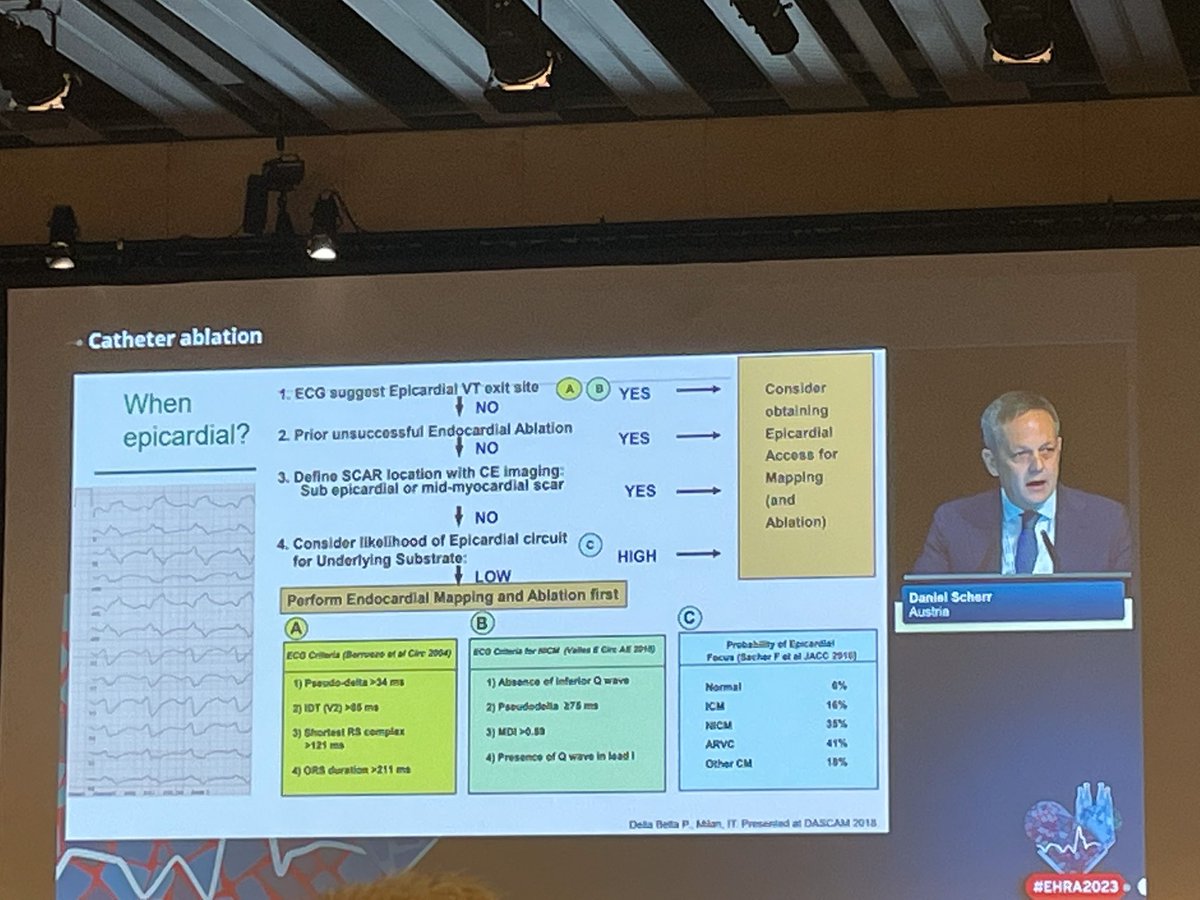
17 Apr 2023
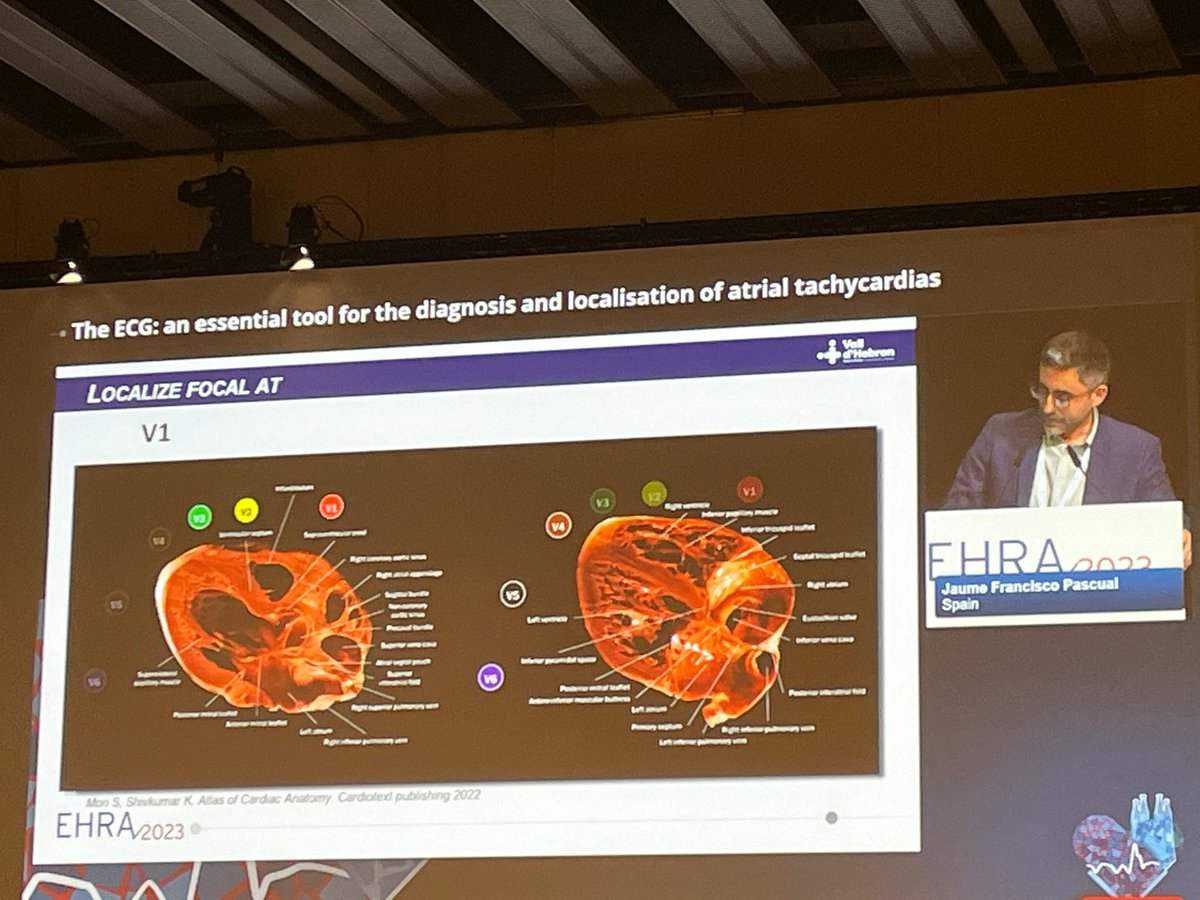
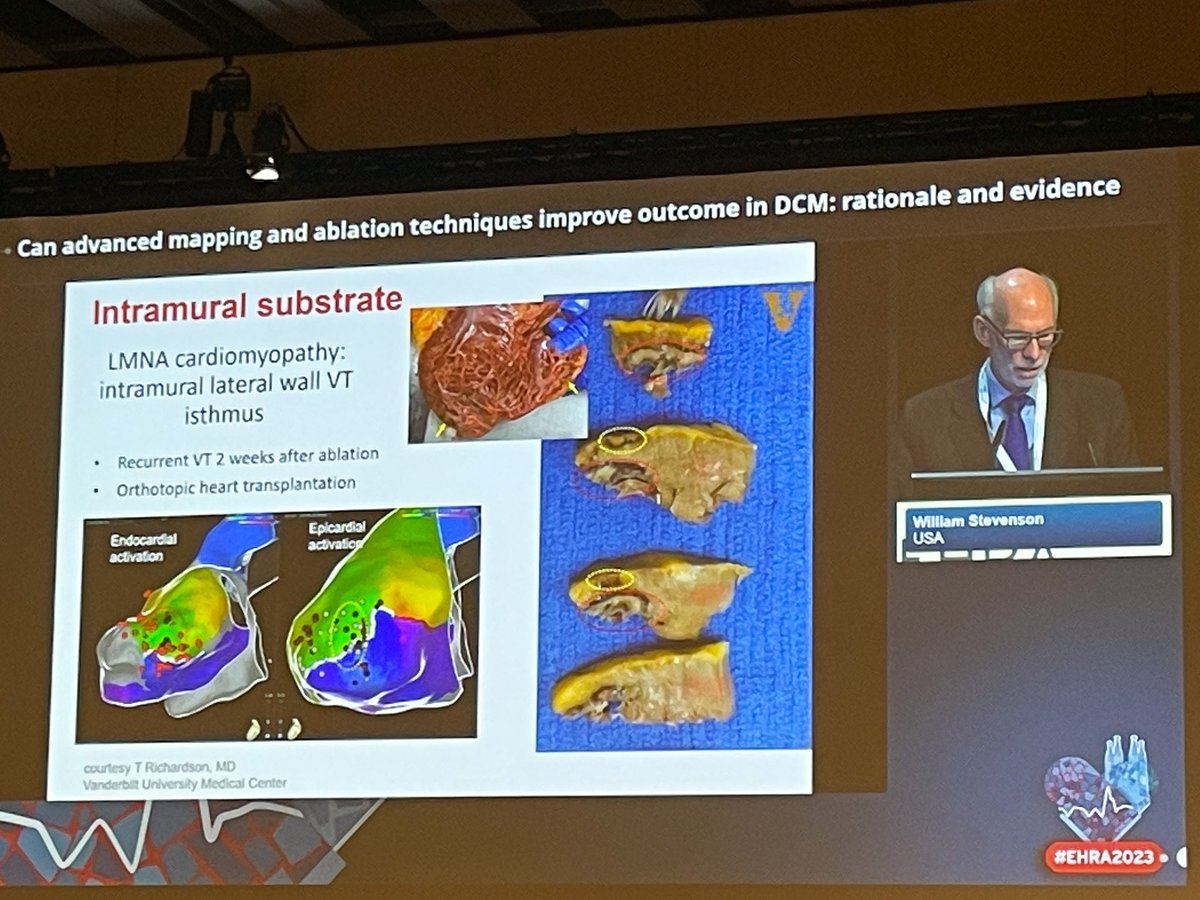
Inspiring talks at #EHRA2023 🔥 #EPeeps #ablateVT #ablateAT #CardioTwitter @C_Meyer_MD @EHRAPresident @FredSacher_EP @DanielScherr3 @shivkumarmd @MarmarVaseghiMD @AGEP_DGK
4
15
2,832

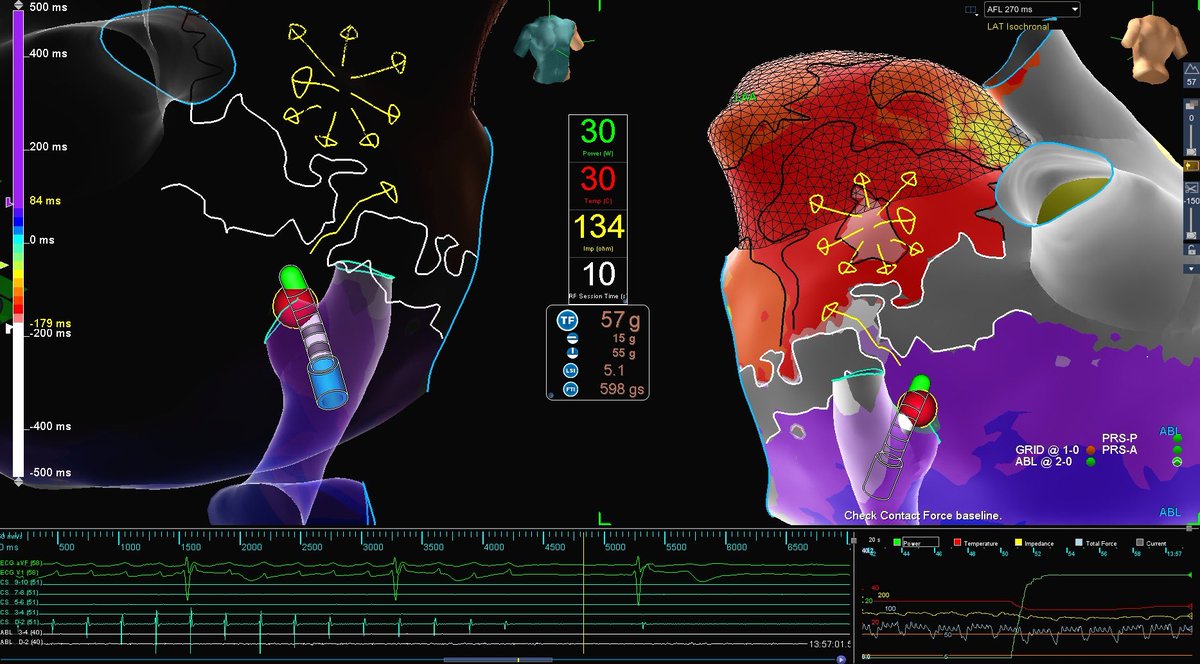
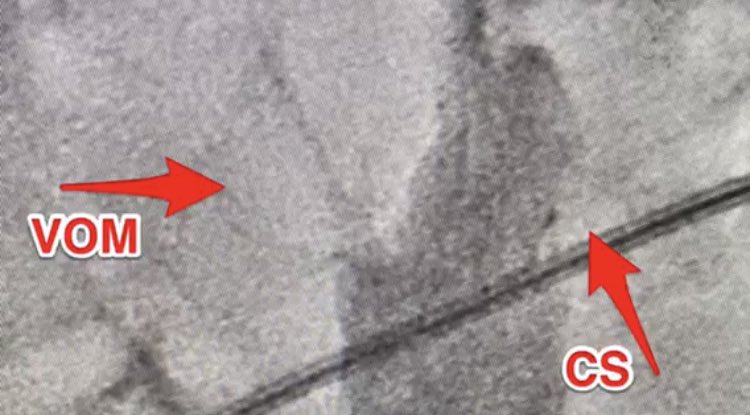
28 Sep 2022
#EPeeps
PMH: x1 Rf OH
PMAT after term of roof-dep AT at yellow dot.
HP endo LML slowed but failed to terminate, probably due to CSm/VOM.
Quick termination thru CS just across endo line & block after epi lesions.
@elifoykucelik @ziya_er @Emreozrdm @BiosenseWebster #ablateAT
2
28

15 Jul 2022
Strong work as usual from @XavierR_EP and @EptingLeslie @Erinwfinnegan @AbbottCardio #HDgrid #EP #ablateAT
2
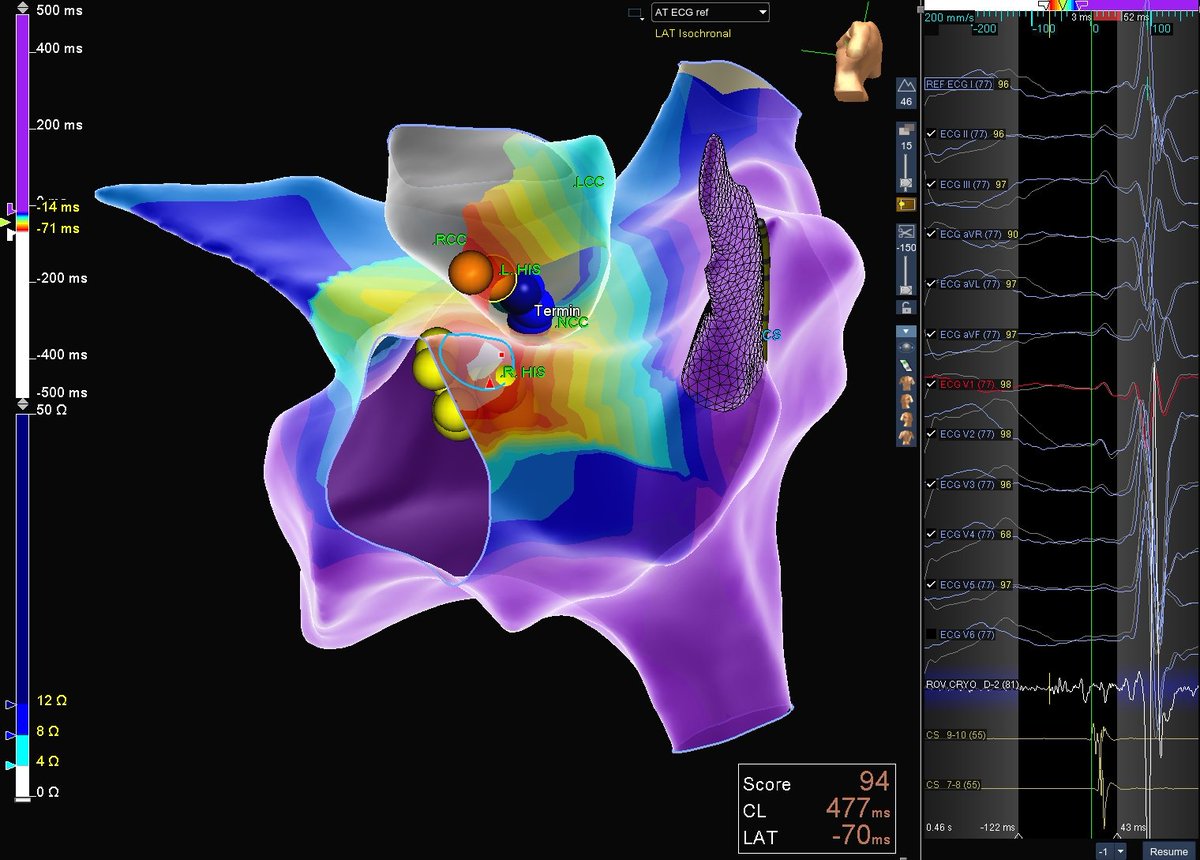
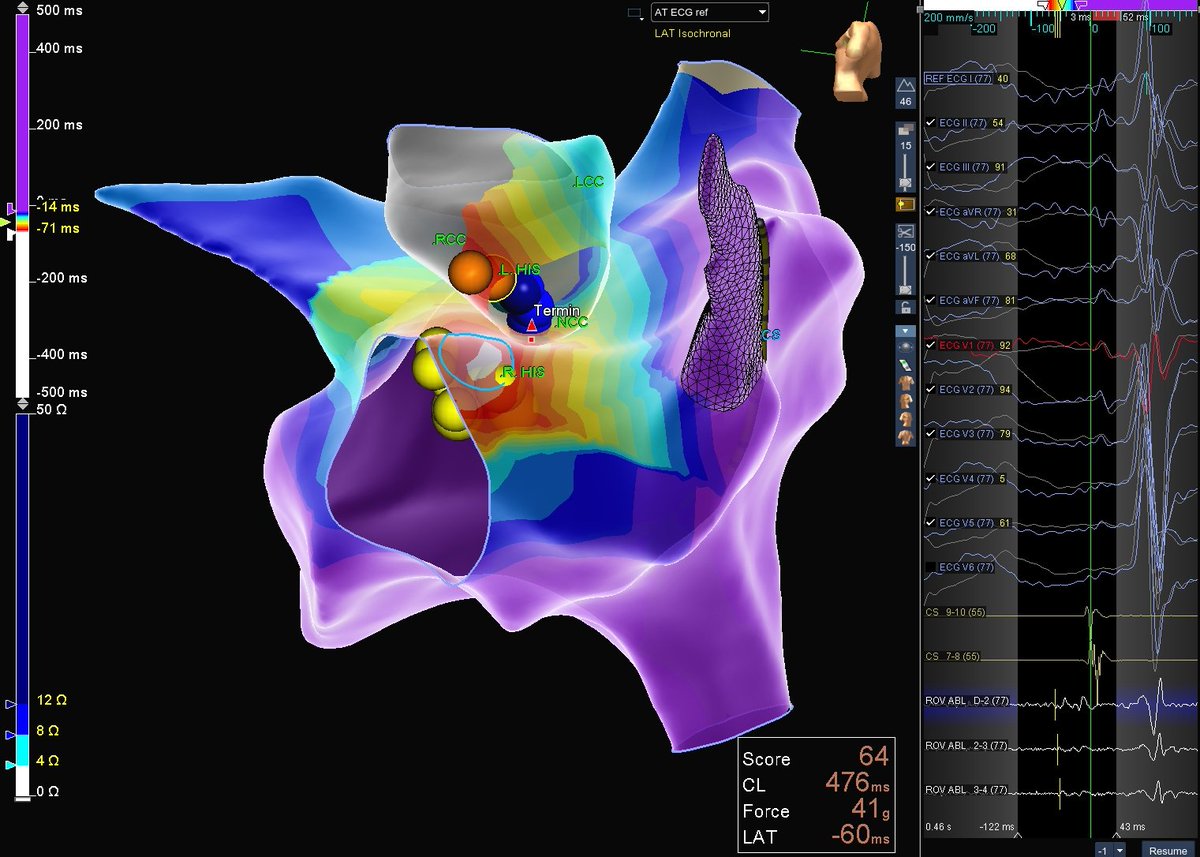
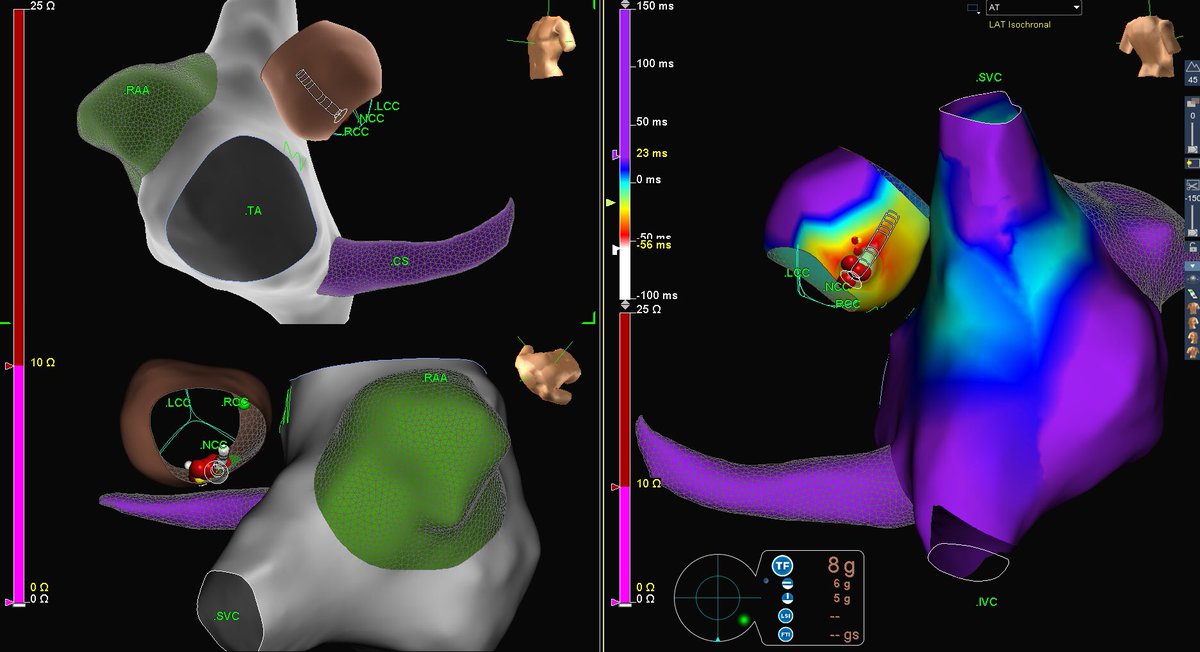
7 Nov 2021
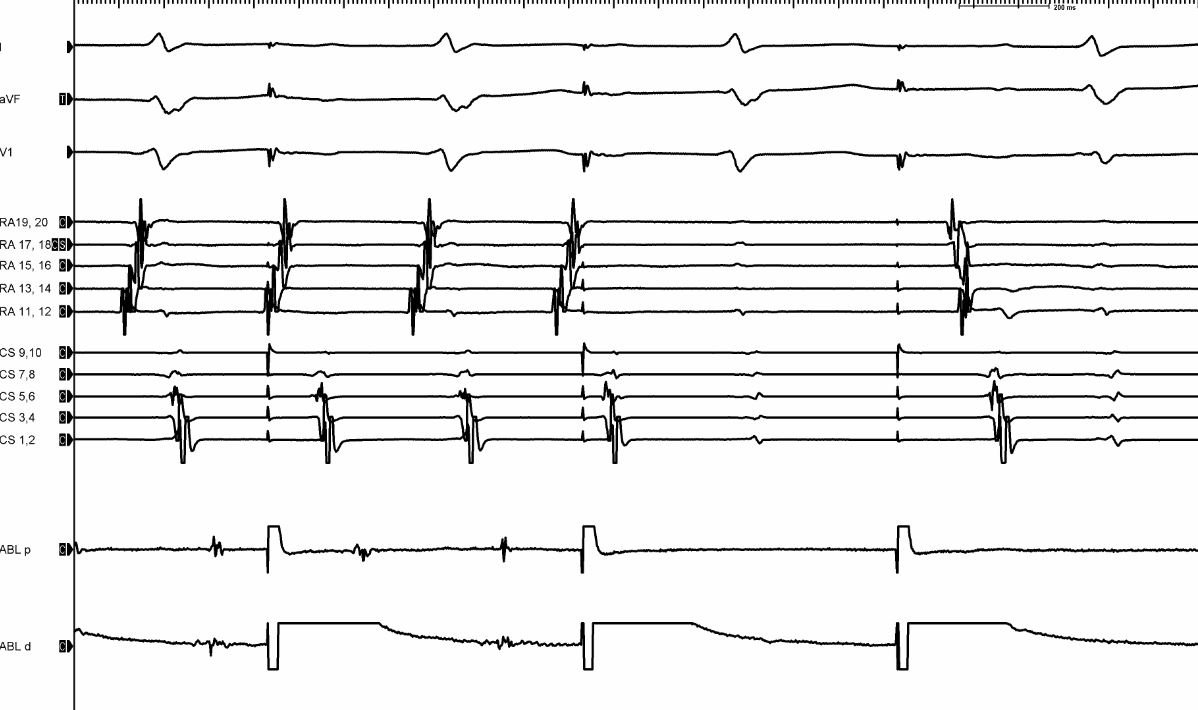
Comparison of earliest AT EGMs at Right HIS vs NCC. NCC timing was slightly later and signal not quite as juicy, but RF still successful without the high risk of AV block (as long as one stays above the valve). #ablateAT #TacticathSE @AbbottCardio
2
3
20

22 Sep 2020
Beautiful map of pt with prior MI line & atypical atrial flutter. VOM ablation resulting in termination (can see endocardial breakthrough on map). Mapping by @Tacoma_EP #AblateAT by Eathar Razak @NasirShariff14 @NathanSegerson @RaviKilaru1 #FranciscanStrongEP @CHIFranciscan
3
9
63

19 Jun 2020
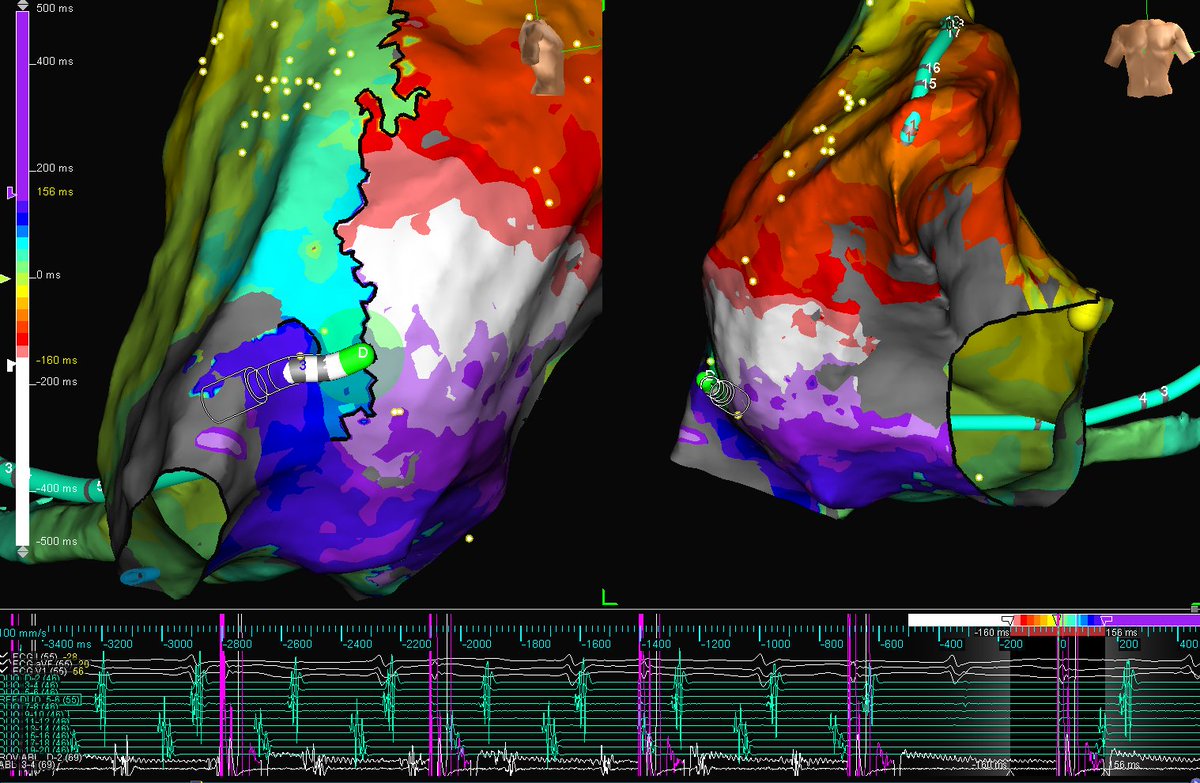
1) Mapping 2) my eyes see a macro-reentrant circuit around left pulmonary veins 2) entrainment manoeuvres confirm what my eyes see 3) selection of best ablation site based on slowest conduction 4) RF on 5) Sinus rhythm.
#EPisBeautiful #AblateAT
4
18
79

26 Sep 2019
Post-MV Repair with AT. Entrained from highly fractionated region near area of linear scar on posterior RA wall with non-global capture. Termination <1 sec with RF at blue dot. @DrJCheungEP @nickkotch @NicholasCostaMD #EPeeps #AblateAT
2
1
10

27 Apr 2019
Me too. He devoted himself to #fluorolessablation. Thank you @MRazminia for excellent teaching points about ICE during #fluorolessablation. #Abbott #ablation #AblateAT #AblateAF

2
1
18

26 Apr 2019
Don't see this too often during AT ablation: nonglobal capture during pacing to check for the phrenic nerve leading to AT termination. #AblateAT
3
6
24
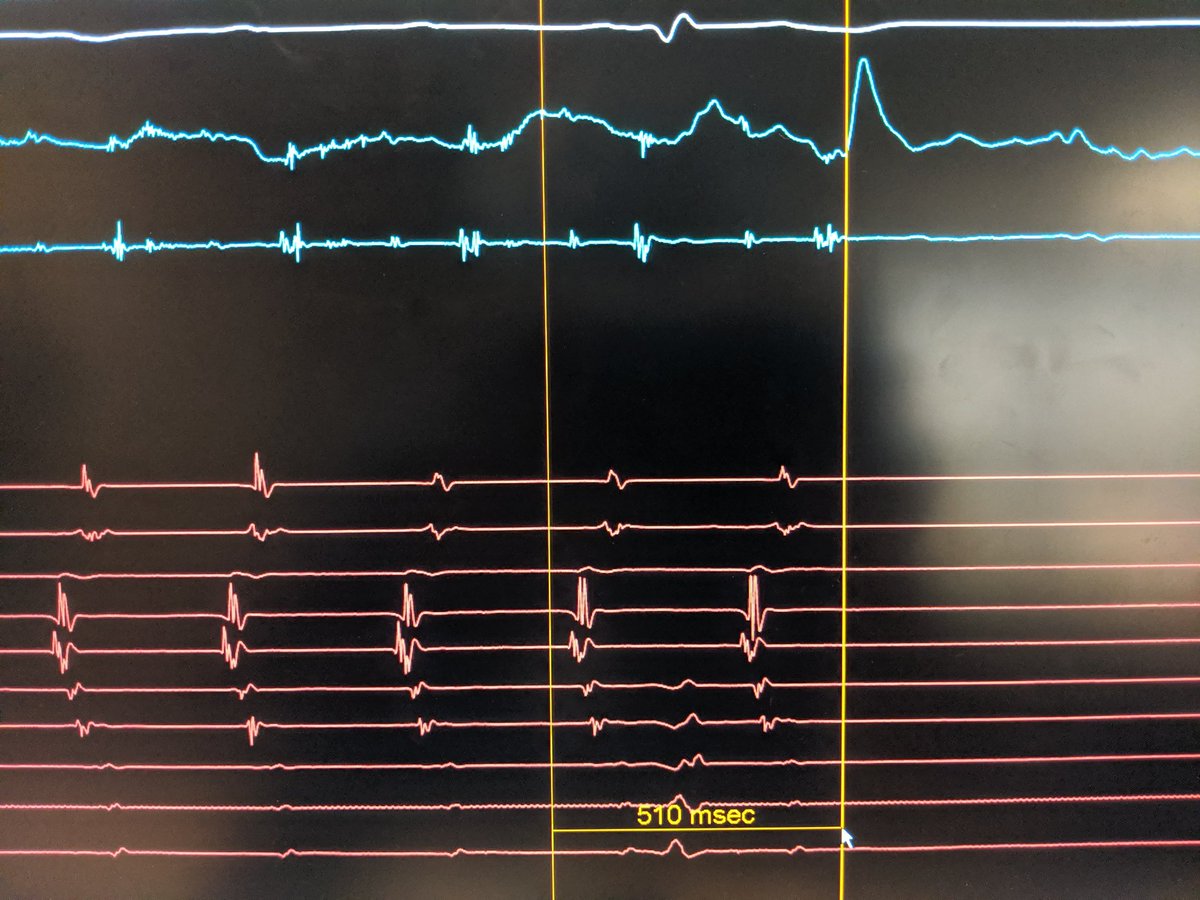
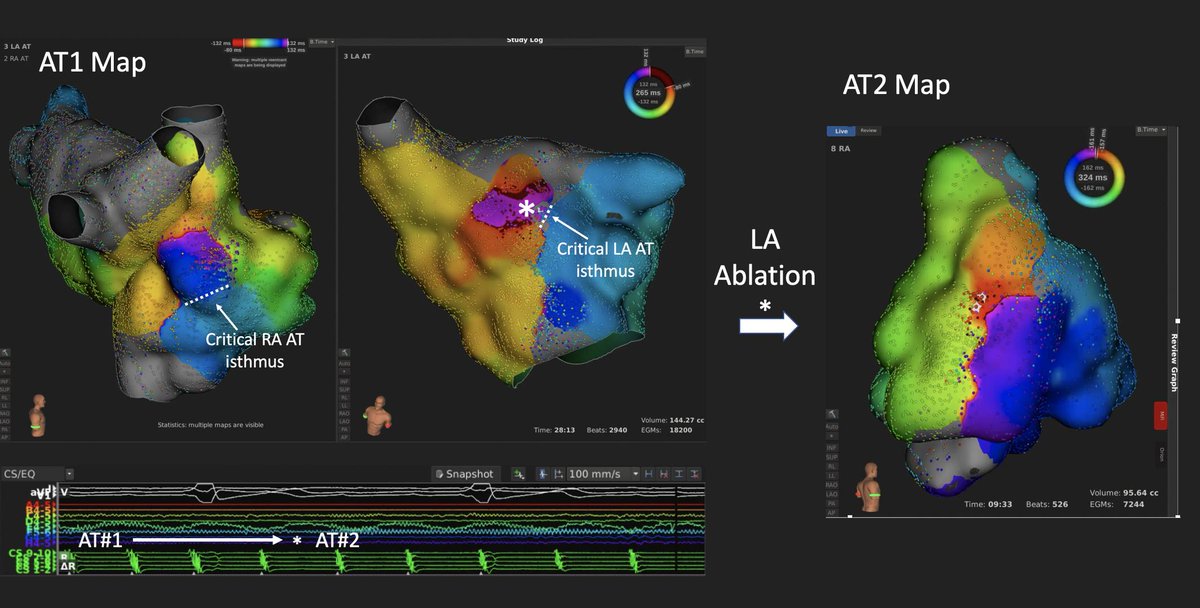
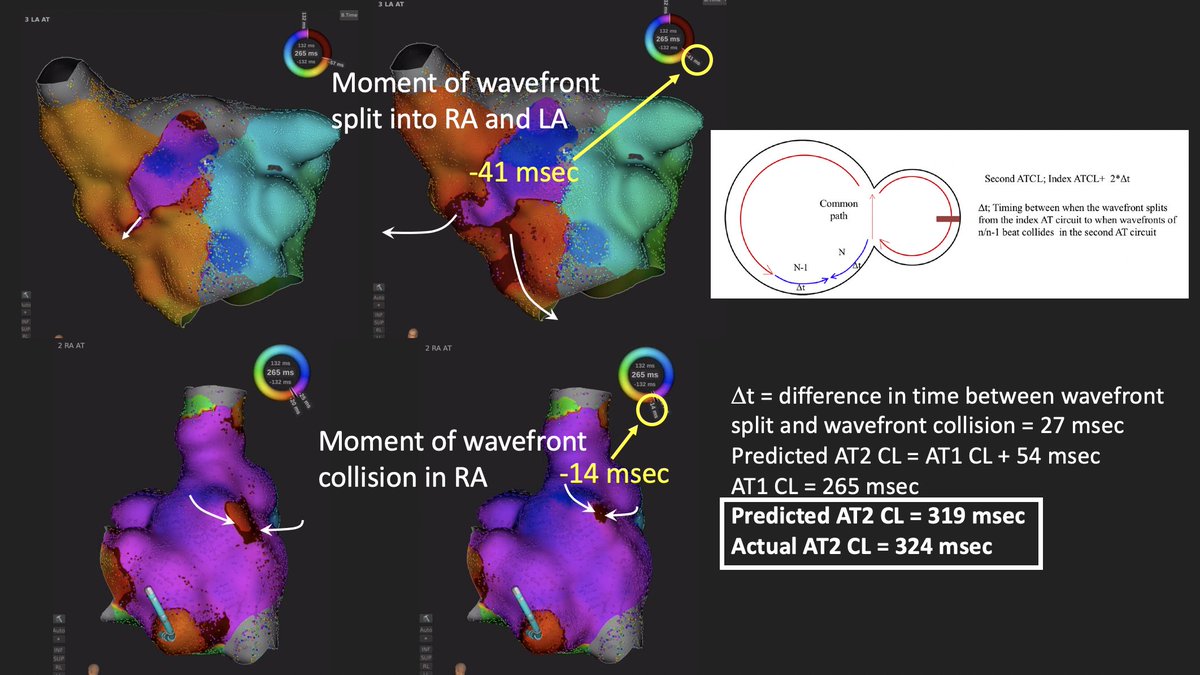
24 Feb 2019
Predicting cycle length of AT1 conversion to AT2 after critical isthmus ablation using biatrial activation maps as per Jais et al. : accurate within 5 msec in this case. Nice when HD activation maps recapitulate cartoon diagrams. #AblateAT heartrhythmjournal.com/artic…
7
24

22 Feb 2019
Biatrial map during flutter. Which functional isthmus would you go after first? #AblateAT
1
13
29

22 May 2018
9
23

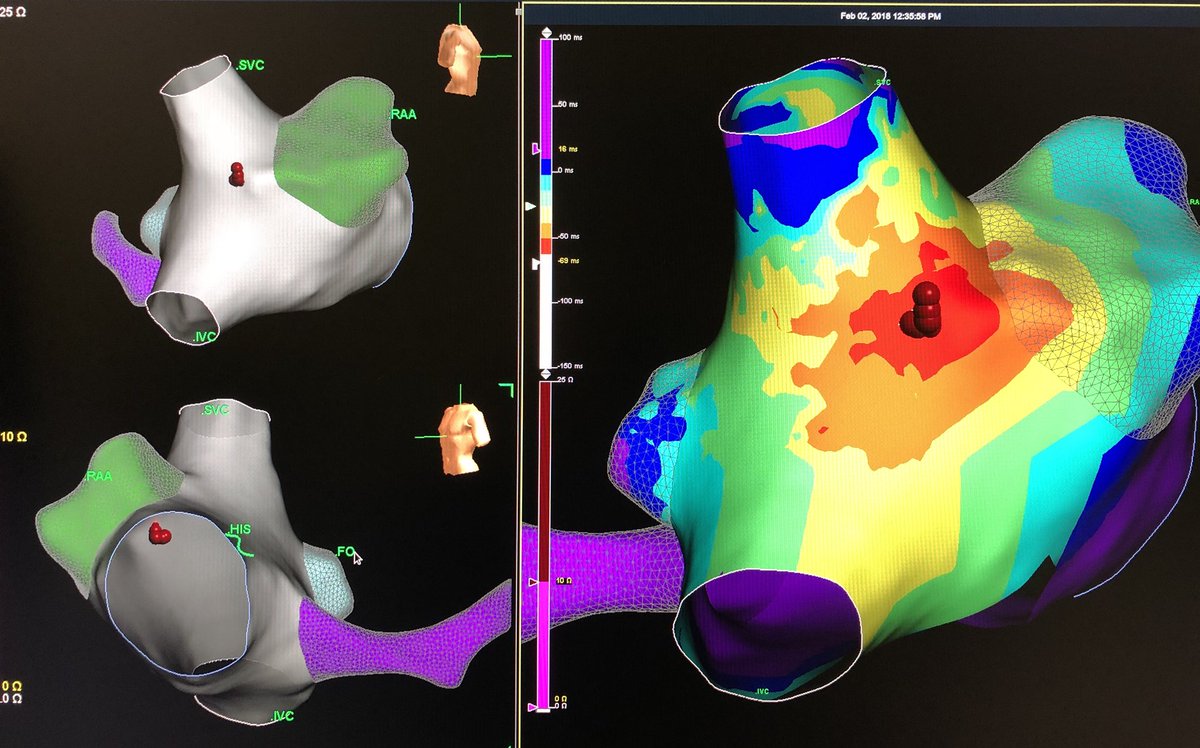
2 Feb 2018
Atrial Tach #ablation on the CT. ~60ms Pre P-Wave and no phrenic stimulation in the area. Termination during RF. #EnSitePrecision #AblateAT @AbbottGlobal
3

11 Jan 2017
1
1
6