Tathagata M. retweeted

Multi-omics reveals microbiota, metabolite, and immunological heterogeneity of age-related endotypes in type 1 diabetes
👇
link.springer.com/article/10…

1
3
3
49

Jun 15
Determining biological mechanistic endotypes is what the $1.5 billion in RECOVER should have done as its first step instead of trying to force fit a symptom survey into an Mecfs phenotype using manipulated statistical models. This is basic biology.

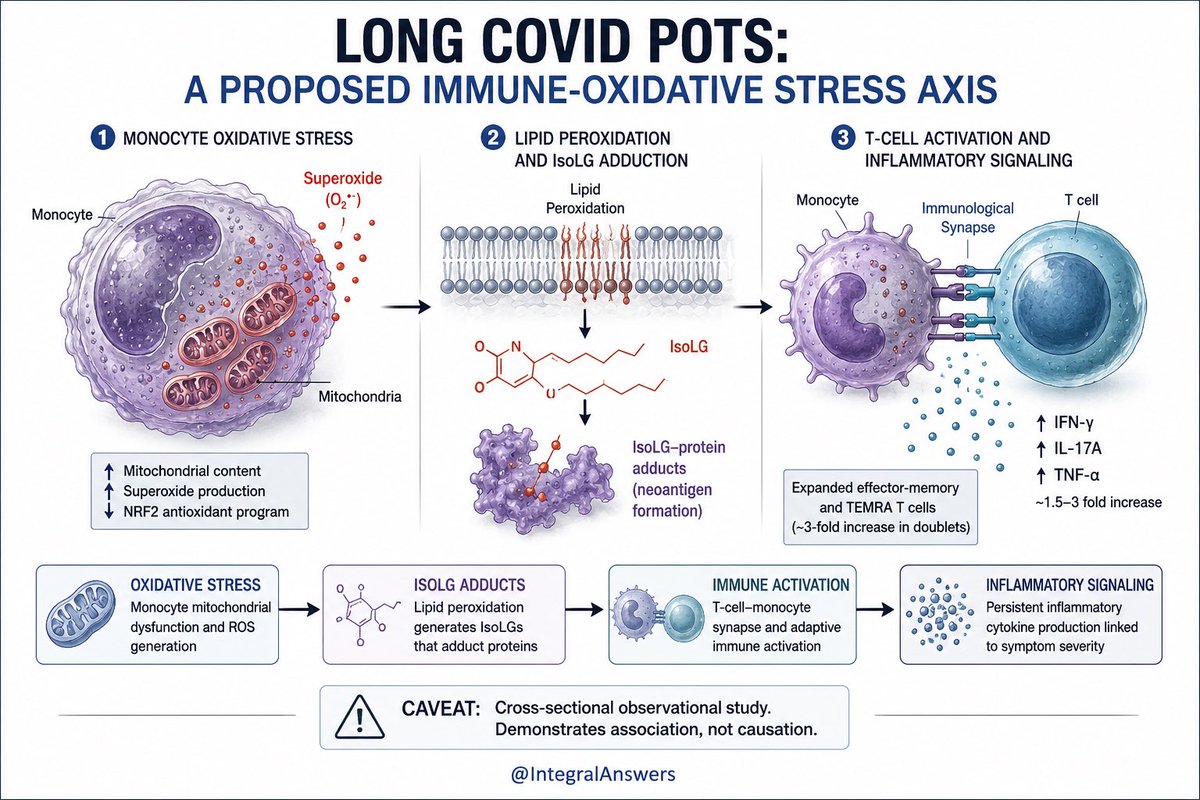
1/ Long COVID research often identifies abnormalities. Fewer studies identify a plausible mechanism linking those abnormalities together.
This new preprint in Long COVID-associated POTS proposes one such pathway:
Monocyte oxidative stress → lipid peroxidation → IsoLG-adduct formation → T-cell activation → persistent inflammatory signaling.
The study found increased monocyte oxidative stress, elevated IsoLG-modified proteins, expanded T-cell–monocyte immune complexes, and higher inflammatory cytokine production in Long COVID POTS patients compared with recovered COVID controls.
Importantly, these findings correlated with symptom burden and autonomic dysfunction.
This does not prove causation.
But it does provide a biologically coherent model that can now be experimentally tested.
That is how progress happens: not by finding “the cause” of Long COVID, but by identifying specific, testable disease mechanisms that may apply to subsets of patients.
5
476
JorgeEdoChava75 retweeted

Jun 14
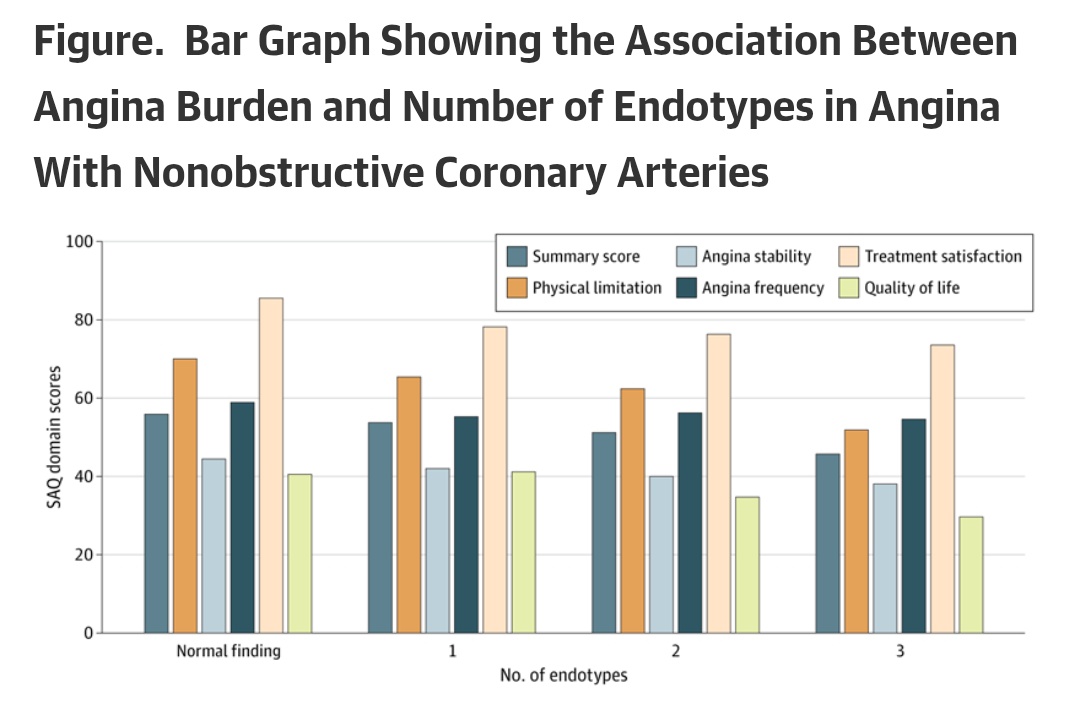
Multiple Endotypes and Angina Burden in Patients With Nonobstructive Coronary Arteries
jamanetwork.com/journals/jam…
Fenotipos MINOCA
1
1
116


This 🇬🇧 study is important in many fronts IMHO
Not because we have an immediate ‘druggable’ target - we have been there before with recombinant IL-10 gastrojournal.org/article/S0…
But it tells us ( or reminds us again !)
📍 IBD have numerous different phenotypes , endotypes and immunotypes
📍in addition to current approaches we will need to start thinking about immune restitution
📍Slowly but surely we are inching towards understanding the biology 🧬 🧫 🧪 of disease
📍For these efforts to bear fruit we need global 🌎 approaches and collaborations
Jun 10

Not every day you see an odds ratio of 50 (for interleukin-10 autoantibodies and a common HLA allele).
~80% of patients with inflammatory bowel disease (IBD) have this HLA allele
These individuals (~3.5% of IBD) may benefit from B cell depletion (such as achieved via CAR T).
nejm.org/doi/full/10.1056/NE…
nejm.org/doi/full/10.1056/NE…

1
7
28
2,334

Jun 12
🎥 Simon Williams, General Manager at PlaqueTec speaks to @BiotechTV, highlighting the aims of our BIOPATTERN trial to identify distinct disease endotypes & novel therapeutic targets for coronary artery disease, stressing that patients are faced with limited treatment options.
Jun 10

𝐅𝐫𝐨𝐦 𝐂𝐚𝐦𝐛𝐫𝐢𝐝𝐠𝐞, 𝐔𝐊: PlaqueTec Ltd.'s has a unique liquid biopsy system and multi omic analysis approach that aims to profile the underlying biology of atherosclerosis.
Full video: biotechtv.com/post/plaquetec…
1
1
17

Jun 11
Take our #AllergyQuiz
Thymic stromal lymphopoietin (TSLP) is an epithelial-derived cytokine involved in airway inflammation and immune activation in asthma. Recent studies suggest that circulating TSLP levels may be linked to specific clinical phenotypes and inflammatory patterns, potentially helping to better characterize severe asthma endotypes.
According to the study “High Serum Thymic Stromal Lymphopoietin (TSLP) Is Characteristic of Late-Onset, Long-Duration, Eosinophilic Asthma”, which of the following statements is NOT associated with high serum TSLP levels?
Check the correct answer by reading the original article by Maho Suzukawa and colleagues. doi.org/10.1111/all.70109
Options:
A) Late-onset asthma
B) Long disease duration
C) Eosinophilic inflammation
D) Seasonal pollinosis
#Allergy_journal
Share your answer in the comment section below. We will post the answer tomorrow.
journalallergy.com/allergy-q…

1
1
2
238

Jun 11
🌿🩺 How do biomarkers, endotypes, pollution & the microbiome shape nasal inflammation?
Explore our Special Issue and submit your research by 30 June 2026!
Guest Editors: Dr. Simonetta Masieri & Dr. Carlo Cavaliere.
🔗 mdpi.com/journal/medsci/spec…

17
Purna Kashyap M.B.B.S., AGAF retweeted

Jun 10
Is there a potential role of proteome-defined endotypes in functional dyspepsia?
@Rajan___Singh & @BMoshiree highlight the need of gaining better insights into functional dyspepsia's mechanisms of action for better therapeutic management
@NGMJournal
tinyurl.com/y6fea6w3
7
9
606

And Adam is an Enigma 🤌; he has parts of all the other endotypes. But the Alpha side is still stronger, although I like to think that his Omega side makes him nest.
1
2
57

Jun 10
@nc_frey @samuel_stanton_
We're currently using Opus to make a new map 🗺️ of medicine, the periodic table of diseases, and would love access to fable's life science program.
Before the periodic table, there was alchemy — two thousand years of sorting substances by what they looked like. Then Mendeleev sorted them by what they are. Chemistry became a science overnight.
Before Google Maps, there was MapQuest — print the page, pray the exit hasn't moved. Then GPS. Logistics became a science overnight.
Before the BioAtlas, there was medicine — labeled by what we can see.
"Asthma" is one word for many molecular endotypes wearing the same name. "Lupus" hides a dozen mechanisms. "Depression" hides hundreds. For four thousand years, doctors have been alchemists in white coats — sorting patients by what hurts, while the actual structure underneath sat invisible.
Then we built the BioAtlas.
Not a model. Not a chatbot. Not a knowledge graph. Not another startup with an LLM on top of UMLS.
The BioAtlas is the substrate. The thing other people build on. The way the periodic table is the substrate of chemistry. The way Google Maps is the substrate of logistics.
The BioAtlas is the substrate of medicine — when medicine remembers it was supposed to be a science.
29