
And he said abacha was not corrupt
He was the head of petroleum trust fund under abacha
He supervised the highest looting in history of the NNPCL and under him d ghost minister of power looted n looted same with Nigeria air, uncountable
I hail the fighter of corruption indeed
2
Colin Sechay retweeted

Jun 8
7,000 miles intervention free on Tesla FSD Supervised:
That’s the equivalent of driving from New York City to Los Angeles round trip & also then driving to Chicago & back all completely hands & pedal free!
Amazing stuff, life changing software
v14.3.3 for the win
49
54
586
49,554

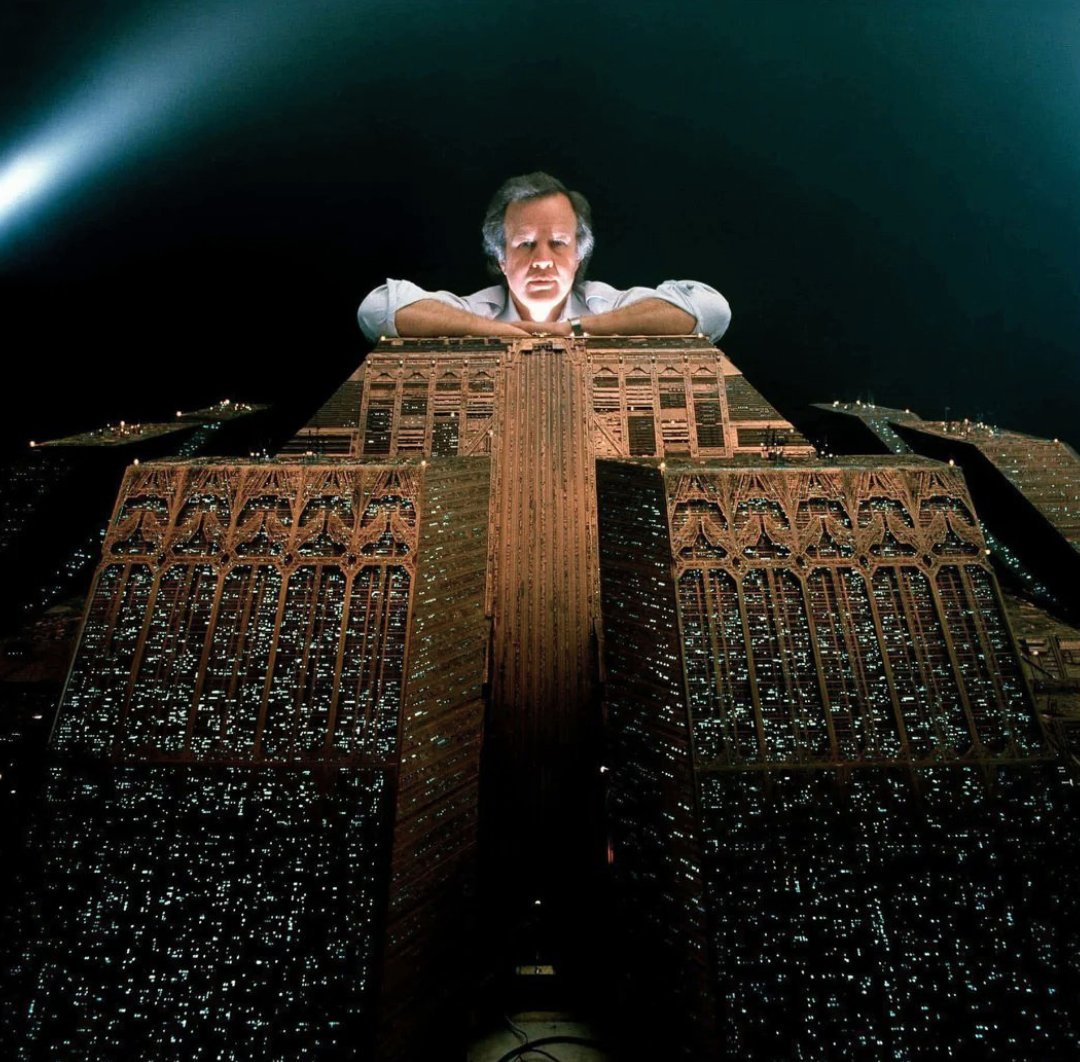
For the 1982 classic film BLADE RUNNER, Mark Stetson and the Entertainment Effects Group, supervised by Douglas Trumbull, used detailed miniature models, smoke, lighting, and aerial photography to create the film’s iconic futuristic sprawling cityscape.


1
77
551
13,462

10m
Transit stations it seems act like sort zones for social abandonment.
And for those who keep failing to move on their “happy path” who are repeatedly overdosing (get strike policy legislation passed on this), psychotic, gravely disabled, obviously unable to care for themselves, there really does need to be an *urgent* as in same-day due-process pathway into mandated care.
I do not mean bring back the loony bins.
I do not mean mass institutionalization.
And not free housing for all the homeless.
More like policy with real triggers: “You are literally dying in public and cannot currently choose safety, so society has to step in with a managed care bed and maybe some sleepy time medicine, for now”
Public spaces do have to be defended.
This part gets dismissed too easily by the “but their autonomy” crowd.
Sidewalks and train station have to be usable by workers, kids, elderly people, tourists, and everyone.
Compassion for addiction does not require surrendering civic space.
In fact, it creates an image of the opposite. Like we see them dying there, but nothing can be done. Like…what kind of so-called society do we actually live in, for real?! The dystopic vibes caused by these individuals can be neutralized by over half with mandatory managed care if [conditons] are met.
And once someone is stable, society should ofter the least restrictive setting they can actually survive in, with fast escalation if they start dying again.
That's the ethical line.
Not "lock them away forever."
Not "let them rot because freedom."
Not "free apartment, no expectations."
Not "jailtime because broken."
More like:
You have been witnessed experiencing repeated life-threatening impairment in public x number of times, and the current pattern shows that you cannot reliably choose safety. That does not mean you are being discarded, punished, or locked away forever. It means society has a duty to intervene before watching you die in a train station, underpass, sidewalk, or emergency room cycle.
You are being placed into managed healthcare environment with structure, and a path back to autonomy.
You will remain in this level of care until you are medically stable, no longer acutely psychotic or gravely disabled, consistently able to meet basic self-care needs, engaged with treatment, and supported by a realistic discharge plan.
Once those conditions are met, you will move to the least restrictive appropriate setting: residential treatment, supervised recovery housing, assisted outpatient treatment, a halfway house, or independent living with case management, depending on your demonstrated stability.
Autonomy returns in stages as capacity returns. If you remain stable, the restrictions decrease. If you repeatedly relapse into overdose, psychosis, grave disability, or public life-threatening self-neglect, care escalates again to more structured settings until reintegration is possible.
The goal is not permanent confinement.
And the ultimate goal is to transition them out of the public legal system, (obviously we gotta pass some laws or sign some order that mandates all of this, with the alternative being criminal charges for extreme and repeated noncompliance) not become even more forever enmeshed in the system.
The goal is survival, stabilization, accountability, and a real path back to freedom. And getting obviously extremely unwell human beings who are on a very public path to their own demise off of our fucking sidewalks and stairwells, it ain’t cute.
3
Romito San Biagio retweeted

Jun 13
NEWS: Tesla FSD Supervised is now approved in 5 EU countries, with 4 more likely next.
Approved so far. The Netherlands, Lithuania, Estonia, Denmark and Belgium. Each one accepted the Dutch RDW approval, so Tesla skips a full re-test in every new country.
Likely next.
~ Greece. The transport ministry has signaled a bill to recognize the Dutch approval
~ Ireland. Tesla is in talks with the national standards body and the transport department
~ Latvia. Testing is underway and a sign-off is rumored
~ Sweden. Public road testing is already running in several cities
Spain is close behind. Its test fleet of 30 plus cars has covered about 80,000 km with zero incidents.
Still waiting. Germany, France and Italy want the EU-wide committee to rule first.
A vote could come late in 2026, with full EU rollout eyed for early 2027.


18
70
476
16,994
banamali mandal retweeted

Two days after JTBC defaulted, four other JoongAng Group entities filed for court-supervised corporate rehabilitation: holding company JoongAng Holdings and affiliates Contentree JoongAng, Megabox JoongAng, and JoongAng P&I.
1
29
225
10,268
Susan Waters retweeted

Jun 13
Anyone wanting to watch 19 minutes of me experiencing @Tesla FSD supervised in Utrecht, here’s the raw video with no edits. You’ll see two interventions, both caused by road closures that were not identified on the sat nav. Otherwise you’ll see a confident drive. @TeslaOwnersUK
9
9
121
19,164
Larry Steele retweeted

Insane to me that Spielberg made both these films in the same year, and supervised post-production on one whilst directing the other. Jurassic Park became the highest-grossing film of all time; Schindler, one of the greatest films ever made. Annus mirabilis, indeed.


6
35
375
10,531

Felix Meyer retweeted

So then please approve Tesla's Full Self-Driving (Supervised) to reduce car accidents 👏🏻⚡️
6
28
274
John Doe retweeted

Jun 13
🇪🇺 Europes Regulators who didn't approve FSD supervised yet are responsible for avoidable accidents - someone should hold them accountable.

Just experienced my first @Tesla Full Self Driving ride, here in Belgium. A friend of mine was one of the first to get the update.
It was smooth, slow, safe and frankly quite boring, but in a good way. After years of watching YouTube videos showing Autopilot and FSD improvements in the US, we finally get to experience it here in Europe.
I’m glad @AnnickDeRidder fast-tracked the approval. On the other hand, it’s quite cynical that stopping to forbid a technology that has been around for years in the US is seen as “innovative” by our politicians.
Europe is still lagging. We have a lot of catching up to do.
Now let’s allow my iPhone to actually be smart instead of forbidding its AI features?
13
33
321
11,545

22m
Tesla FSD Supervised가 덴마크에서 승인되었다. 네덜란드, 리투아니아, 에스토니아에 이어 유럽 네 번째다. 6월 9일 발표 후 곧 덴마크 차량에 배포된다. 네덜란드 초기 데이터에 따르면, FSD Supervised 사용 차량의 충돌률이 수동 운전 대비 3.5배 낮았다.
#Tesla #FSD
출처 → teslarati.com/tesla-full-sel…
19
AaronGonp retweeted

Warum ASTRA in der Schweiz FSD Supervised freigeben muss – für mehr Sicherheit auf unseren Strassen
@UVEK @BR_Sprecher @TCS_Suisse @TOS_Switzerland

1
5
34
737

Consumer car can be washed or wiped by the owner at any time orc transition from unsupervised and just toggle on supervised if conditions aren’t able to be met. A fleet car can’t. I don’t understand how washers are going to help you in the rain though tbh.
2
1
7
Cristóbal Vega retweeted

🔥🇨🇳 A video showcasing Tesla FSD (Supervised) v14 in China has leaked on social media!
The video is intended for FSD (Supervised) page in China, which has not yet been published.
I was able to access it a few days ago thanks to @ardacebie, but decided not to share it at the time.
Here is the video, extracted directly from Tesla’s official website:
3
3
40
3,562

26m
[11/25] 📄 arXiv cs.CL
Supervised fine-tuning and reinforcement learning enable LLMs to achieve strong automated medical ICD coding performance, exceeding prompting-only approaches.
arxiv.org/abs/2606.13940
1

ADS L4 regulation approval at UNECE level might happen before L2 DCAS get to the level of FSD Supervised
1
2
68

The situation has rapidly progressed. Despite the intense friction caused by the early morning Israeli airstrike on Beirut, President Trump and Iranian officials have officially announced that a comprehensive **peace deal has been reached**, bringing an end to nearly four months of devastating warfare.
Trump took to Truth Social late Sunday evening to deliver the formal announcement:
> "The Deal with the Islamic Republic of Iran is now complete. Congratulations to all! I hereby fully authorize the toll free opening of the Strait of Hormuz, and, simultaneously herewith, authorize the immediate removal of the United States Naval blockade. Ships of the World, start your engines. Let the oil flow!"
>
## Core Pillars of the Agreement
While the exact textual nuances are still emerging, the broad terms of the memorandum of understanding (MOU) finalized through Qatari mediation include:
* **End of the War:** The deal dictates an immediate end to the 100 day war between the U.S. and Iran, and crucially integrates a sweeping "hold fire" mandate across all fronts, explicitly including Lebanon.
* **Maritime Reopening:** Iran will immediately halt interference in the Strait of Hormuz, which has been functionally choked off since the war began on February 28. Under the agreement, Iranian forces will clear defensive mines within the first 30 days and waive transit tolls for a 60-day period. Simultaneously, the U.S. is lifting its naval blockade on Iranian ports.
* **Nuclear Material Concessions:** Tehran has reaffirmed its commitment not to procure or develop nuclear weapons. Crucially, Iran has agreed to allow International Atomic Energy Agency (IAEA) supervised on-site dilution of its massive 9,000kg enriched uranium stockpile (which includes roughly 440kg of near weapons-grade material).
* **Phased Economic Relief:** The U.S. will grant immediate oil export waivers to Iran for the duration of a 60-day ceasefire extension. However, permanent sanctions relief and the unfreezing of overseas Iranian assets remain strictly tied to step-by-step progress when formal nuclear negotiations commence.
## The Reality in Jerusalem: A Deep Strategic Fracture
The inclusion of Lebanon in the final agreement has triggered an existential policy shockwave in Jerusalem. Israeli officials had actively lobbied to exempt their northern operations from the U.S.-Iran framework, signaling they would comply with protecting the capital of Beirut but intended to continue pushing deep into southern Lebanon to clear out Hezbollah.
Trump soundly rejected that position, demanding an absolute halt to Israeli operations across the entire country. The diplomatic fallout is stark:
* **The Southern Lebanon Withdrawal:** Behind closed doors, Trump went so far as to propose that Israel physically withdraw its ground troops from southern Lebanon as a component of regional stabilization—a demand Prime Minister Netanyahu reportedly rejected outright.
* **A Resounding Slap in the Face:** A senior Israeli official close to the Prime Minister told local networks that Trump's public, expletive-laden dressing down of Netanyahu's judgment represents a "resounding slap" that takes diplomatic restrictions on the IDF to an unprecedented level, calling Trump's expectation of a total halt "incompatible with the behavior of a strategic ally."
## What Comes Next
Iranian Deputy Foreign Minister Kazem Gharibabadi confirmed the breakthrough on state television, noting that implementation will scale up immediately. According to Pakistani Prime Minister Shehbaz Sharif, who has been intimately involved in tracking the regional mediation, the warring parties are now scheduled to meet for a formal, in-person signing ceremony on **Friday, June 19, 2026, in Switzerland**.
16

Oshiomole is a former NLC chairman, served as governor for eight years, and is now a senator of the Federal Republic of Nigeria.
One would expect a man with this profile to have someone helping him with research and providing accurate information. Instead, in this video, Oshiomole spews two outrageous lies.
The Bakassi Boys ceased operations in 2002/2003. Therefore, Obi did not encounter them when he assumed office. The fact that Oshiomole didn’t know this, yet spoke about it with confidence, speaks volumes about our leaders.
Secondly, Obi was one of the very first governors to enact a rule that any house associated with kidnapping would be demolished. Obi personally supervised some of these demolitions. Obi was more than brutal to criminals in Anambra.
Again, that a man of Oshiomole’s caliber would appear on a podcast and spew outright lies speaks volumes.
While Obi discusses Nigeria's problems, these men discuss Obi.
1
5
67