
Geopolitical analyst & columnist, pro life, 1a,2a, coffee addict, traveller by heart, space exploration enthousiast
Joined November 2023
- Tweets 119,115
- Following 59,143
- Followers 76,646
- Likes 103,418
7,454 Photos and videos













Pinned Tweet

13 Jul 2025
Check out my latest op ed in @Saxafi
Somaliland; a nation denied no more; a path to diplomatic recognition by 2029 leveraging their Stable democracy, thriving economy, & strategic location.
saxafimedia.com/somaliland-n…
57
101
724
84,738
Jun 7
The Gaza Roadmap will collapse in months. Here’s the brutal reason no one wants to admit:
zero real disarmament and zero deradicalization.
blogs.timesofisrael.com/gaza…
3
3
12
537
Jun 5
Trump declared the Abraham Accords “mandatory” for Saudi Arabia, Qatar, Turkey, Pakistan & more as part of any Iran deal.
Think this is a huge win for Israel? This must-read explains why it could actually make Israel less safe:
blogs.timesofisrael.com/trum…
7
5
14
644
Brian McDonald B retweeted
Jun 1
Democrats try to nuke Israel’s 50-year nuclear ambiguity policy
the one thing that’s kept the Middle East from going full nuclear arms race. The legal trap is real and the timing is no coincidence. Read this:
blogs.timesofisrael.com/the-…
7
21
1,328
May 27
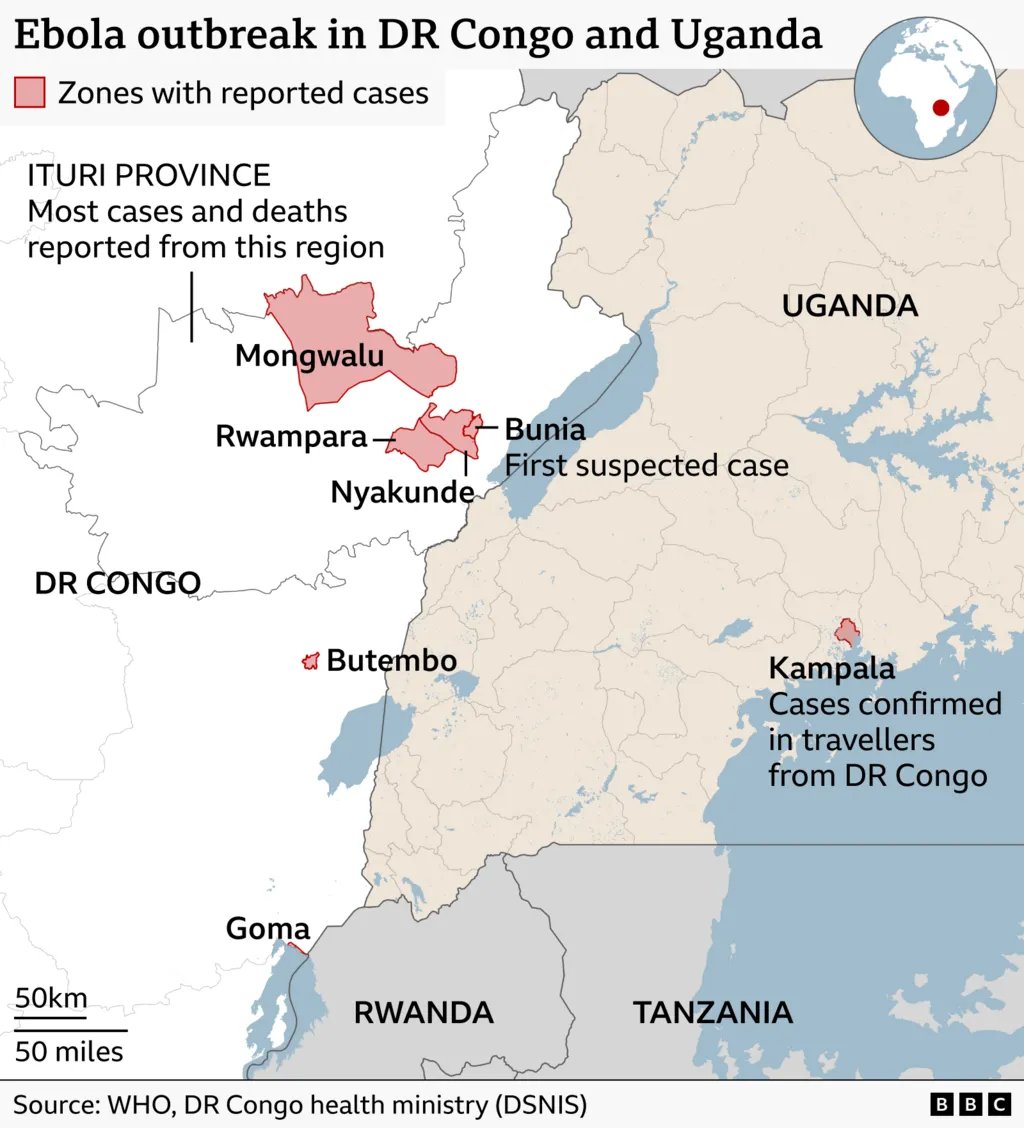
Ebola-hit DR Congo faces 'catastrophic collision' of disease and conflict, WHO warns
The World Health Organization (WHO) has declared the outbreak of the rare Bundibugyo variant of the Ebola virus in the Democratic Republic of Congo (DRC) and Uganda an ‘international emergency’.
Bundibugyo is a deadly virus strain for which no vaccine exists, nor is there any treatment available. So how can the outbreak still be contained? The coming days are crucial, says epidemiologist and microbiologist Amrish Baidjoe of Doctors Without Borders.
How big will this outbreak become?
‘The numbers we are seeing now are substantial, especially when you look at previous outbreaks.‘The virus was discovered late.’ When the outbreak was confirmed, we were already at a fairly high number of deaths , at least 220 ‘suspected’ deaths in various regions , and hundreds more infections in the DRC as well as in Uganda.
DR Congo health authorities have been struggling to confirm cases of the 220 deaths, only 17 people so far have been confirmed by lab tests as having died from the disease. Medics are also facing a race against time to trace 3,600 people identified as contacts of the infected group.
Some 2,000 tests have been distributed, with a further 4,000 due to be sent out. Experimental treatments , including an antibody developed in the US , could also be introduced soon.
This means that the virus has been circulating for at least a month. The virus appears to be widespread. The numbers mentioned are likely an underestimate of the number of sick and dead. I am not going to speculate; the situation on the ground is still too unclear and too dynamic, but I am concerned.
The WHO’s use of the term ‘international emergency’ is justified. The coming days are crucial: how quickly can aid workers arrive, how quickly can clinics be set up?
‘It is going to be one of the bigger outbreaks regardless. But there are many things we do not know yet. Everything depends on the response in the coming days and weeks. Every day of delay significantly increases the risk.’
How deadly is this Bundibugyo strain?
‘The mortality rate of the Bundibugyo virus is high: between 40 and 60 percent. It is a strain we do not see often. That means that little research has been done on it.
These percentages are based on relatively small outbreaks. We know that mortality decreases when people are treated more quickly. As an outbreak progresses, you often see the mortality rate drop.’
Sometimes the mortality rate rises to 90 percent. How is that possible?
Baidjoe: ‘You only see that when there is absolutely no treatment. In those complex situations, it is often difficult to test exactly what someone is dying from.
People sometimes also suffer from other fatal diseases, such as malaria or AIDS. Treatment for those can come to a standstill because all attention is focused on the Ebola outbreak.’
How can an Ebola patient be recognized?
Baidjoe: ‘The image of fear everyone has of Ebola is the patient whose eyes are bleeding.’ And it is true, these are hemorrhagic viruses.
People can bleed from their ears, from their noses, and from their mouths. They also have internal bleeding, which can lead to massive bruises, although these are not always clearly visible on dark skin.
But the complicated part is that this only happens in the final, most severe phase. Initially, patients actually exhibit nonspecific symptoms: fever, muscle pain, malaise, and later also diarrhea and vomiting.
We often don't even see that bleeding. If we do see it in a patient, they are actually already so sick that there is not much more that can be done. But people often die at an earlier stage.’
‘The main problem with the Ebola virus is that patients become severely dehydrated due to vomiting and diarrhea. That can happen quickly. This virus is very aggressive. Due to that dehydration, all organs shut down, and patients eventually collapse.’
Baidjoe: ‘So it is difficult to identify patients early, especially in areas where malaria is also prevalent. It is hard to distinguish; it all looks very similar.’
What should the approach of aid workers be?
Baidjoe: ‘You have to focus on active ‘case finding’. So, you ask everyone who has a fever to stay at home. After that, you have to keep looking for them and place them in isolation at the local hospital if their condition worsens – although it is questionable whether there will be enough space there.
Especially at the beginning of an outbreak, this way of working is complicated. Health workers have to go through cities, villages, and homes. But are there enough people to do that? Can they even enter that region? And also: how do you equip them?
I just know that right now there isn't enough protective clothing for healthcare workers in the affected areas. They are at enormous risk. The virus is highly contagious, via all bodily fluids. Then keeping a distance is sometimes the only thing they can do.’
Hopman: ‘Health workers need to build a bond with the community leaders. With the chief, the traditional healer, the religious leader. If there is mutual trust, or actually, it should already be there, then you often see that the response goes well.
If not, then it becomes complicated. Something like that is crucial. If people think that upon reporting illness they will simply be taken away and locked up without having any say in the matter, then they won’t report themselves. Something we also saw during previous Ebola outbreaks in West Africa.’
Stories are circulating in the media about young people dragging the deceased and placing them in graves with bare hands and without face masks or further protection. How do you view that?
Hopman: ‘All those materials – gowns, face masks – need to be shipped and flown to the area as quickly as possible in the coming days. But the distances are enormous, the roads are bad.
The Democratic Republic of Congo is one of the largest countries in the world; we sometimes forget that. But the main problem is the armed conflict.
You can't just go from village to village there with the local health service, like we do in the Netherlands. Eleven incidents involving healthcare workers have already been reported. It is unsafe, and it is very complex to work there.’
Are there tests for the Bundibugyo virus?
Baidjoe: ‘Testing is currently only possible in a laboratory setting. You have to start setting up facilities for that. Rapid tests using a drop of blood do not exist yet. At least: no validated tests.
I know that teams have been sent to the area that can build a small laboratory from a dozen suitcases, allowing them to test people on the spot.’
Which factors exacerbate the situation?
Baidjoe: ‘The area is close to the border with South Sudan, a country with one of the most fragile health systems in the world. People travel back and forth a lot in that region. Funeral ceremonies also constitute major sources of infection: we still frequently see people washing the body of the deceased. What makes matters even more complicated is that there is no vaccine against Bundibugyo yet.
During outbreaks involving other variants, we built a shield around a source of infection through vaccination campaigns so that it could die out.’
Why does that vaccine not exist yet?
‘The Bundibugyo variant has caused relatively few outbreaks; the last one was in 2012, so there was no opportunity to test vaccines in practice.’
What can doctors do for infected patients?
Baidjoe: ‘For other variants, doctors can administer so-called monoclonal antibodies, but these do not yet exist for Bundibugyo. The only thing you can really do is administer fluids via an IV.’
#ebola #uganda #drccongo #who
1
3
4
702
May 25
Factcheck ;Ex-CIA Larry Johnson claims Israeli F-35 fighter jets lack the operational range to hit targets inside Iran
Asnwwer; Wrong, The F-35s hitting Iran aren’t your standard F35's the US uses. Israel’s modified F-35I Adir has extended range to reach Tehran without needing refueling.
Key Facts
◾️Israel operates the F-35I Adir, a heavily customized variant, the most modified F-35 of any operator. It includes Israeli-made electronic warfare systems, software, weapons integration, and stealth-compatible range-extending fuel tanks (conformal and low-observable external tanks).
◾️These modifications give the Adir an effective combat radius of ~1,700 - 1900 km, enough to reach western and central Iran (including Tehran) for many mission profiles without mid-air refueling.
◾️During the June 2025 strikes and 2026 operations, modified F-35Is conducted deep strikes into Iran. U.S. officials told Middle East Eye that the F-35Is operated without mid-air refueling during key attacks.
◾️Refueling is only needed for non-F-35 aircraft (F-15I, F-16I) and deeper eastern Iranian targets, but it is not needed for the F35 Adir on the main areas Israel has struck.
◾️Recent reporting (May 2026) confirmed Israel used secret forward outposts in western Iraq for refueling and logistics. These helped overall operations but were not required for F-35I strikes on western and central Iran.
Sources
◾️Range modifications & 1,700 km radius: The Aviationist (Jun 2025), The War Zone/TWZ (multiple 2025–2026 reports), National Interest (Feb 2026), Israeli Ambassador confirmation via Times of Israel (Feb 2026).
◾️No refueling in 2025 strikes: Middle East Eye (Jun 2025, citing U.S. officials).
◾️Secret Iraqi bases: New York Times (May 17, 2026), Wall Street Journal (May 2026), Jerusalem Post (May 2026).
Bottom line: The F-35I Adir was specifically modified to eliminate reliance on refueling tankers for strikes on western and central Iran. The claim treats it like a standard F-35 which is not what Israel uses.
May 25

🚨🇺🇸🇮🇷 Any theory about Israel executing a military strike against Tehran is mathematically impossible without massive American intervention.
Ex-CIA Larry Johnson points out that Israeli F-35 fighter jets fundamentally lack the operational range to hit targets inside Iran without multiple mid-air refuelings from U.S. tankers.
Larry said that If a single bomb drops on Iranian soil, Tehran is fully locked, loaded, and prepared to instantly turn the entire Gulf into a total war zone.
@newsonof
3
3
10
1,301
Brian McDonald B retweeted
May 21
About abusive relations and shifting alliances in the Middle east
FDD expert @hahussain rightly notes the relationship between Iran and Saudi Arabia is very much that of a teenage girl(saudi Arabia) unable to get over her love tofor her abusive partner (Iran)
Meanwhile the adult in the room, MBZ from UAE is distancing the UAE from failing states and organisations ( OPEC and OPEC and reviewing Arab league and OIC) who didnt show up when it counted, when UAE was under attack.
and forging a future with like minded countries like India, Israel, USA, Somaliland etc.
While the Saudis are getting closer to Pakistan ,Turkey and Qatar, and are not seeing its a dead end. its a collection of radicalised, largely Muslim Brotherhood compromised countries on the wrong side of history.
MBS has had such bold plans for the future, from his Vision 2030 to modernise Saudi Arabia and reforms for women, social refomrs, labor reforms, here is what he introduced:
Women’s Rights & Social Reforms
◾️Driving Ban: Lifted the decades-long ban on women driving.
◾️Guardianship Laws: Weakened the strict male guardianship system, permitting women to travel, work, and access government services without male permission
◾️Public Entertainment: Reopened cinemas, permitted music concerts, and allowed public, co-ed celebrations.
◾️Religious Police: Stripped the Committee for the Promotion of Virtue and the Prevention of Vice (the religious police) of their powers of arrest and harassment.
Legal & Judicial Modernization
◾️Codified Laws: Replaced a patchwork of judicial discretion with formalized legal frameworks.
◾️New Legislation: Enacted codified laws addressing civil transactions, evidence, and personal status.
Economic Diversification & Fiscal Reform
◾️Subsidies & Taxes: Phased out broad utility and fuel subsidies and introduced a 15% Value Added Tax (VAT) to diversify government revenue.
◾️Tourism & Visas: Launched tourist e-visas to open the country to international travelers and boost foreign investment.
◾️Megaprojects: Invested heavily in new high-tech cities, tourism corridors, and entertainment sectors, such as the NEOM development project.
Labor Market
◾️Employment: Greatly increased female participation in the workforce.
◾️Nationalization: Enacted "Saudization" policies aimed at replacing foreign workers with Saudi citizens to lower domestic unemployment.
For a brief time it seemed like he wanted to join the progressive camp in the Middle East.
But he never did the deep groundwork in society the way UAE did, like deep reforms of the education system, curricula, religious freedom, mediareforms and government needed to turn public opinion towards a more positive attitude towards Israel and to turn Saudi society more progressive. He lacked the larger vision that the UAE had, who understood that to bring the country into the future they needed to reform public opinion and invest in it, to create the poltical domestic room for the bold moves they made.
MBS economic reforms largely faltered as he failed to achieve the degree of doversification of the economy away from oil like UAE managed. His headline projects like Neom and the Line are all scaled down as investor interest has been lacking
So in a irrational move MBS reverted back to play the strong islamic conservative card, the nationalistic card, and anti israel playbook , repeating past failed policies that iwll get him nowhere.
He and his inner circle see Israel as the larger regional threat(while Israel has no ambitions for expansion, hasnt started any war first) and rival after the june 2025 war and 2026 war,
but fails to see the Turkish neo ottoman expansionist ambitions and risks financing a rival(Erdogan) who would like to replace MBS and Iran as regional power broker.
When history will be written years from now, this strategic miscalculation by MBS will be noted as what doomed Saudi Arabia.
May 21

The current relationship between Saudi Arabia and Iran today is like one between a teenage girl (Saudi) unable to get over her love to her abusive partner (Iran).
1
6
16
1,940
Brian McDonald B retweeted

The Calm Before the Storm: Decoding Iran Negotiations
Join us for a critical conversation on the future of Iran negotiations, regional security, and the implications for Israel and the Middle East.
📅 Sunday, May 24
🕦 11:30 AM EST | 6:30 PM Israel time
📍 Live on X via @MOSSADil
Featuring: @JSchanzer | @Dan_Diker
Moderated by @sabrinasoff
Be there.

4
21
53
70,324
May 22
Starship’s Raptor engines ignite during hot-staging separation
2
4
10
715
May 22
New attempt to launch starship testflight 12
with the newly designed V3 starship
See the launch on this livestream as Musk keeps pushing to go back to the Moon, Mars and beyond

Watch Starship's twelfth flight test x.com/i/broadcasts/1pKkOykQR…
1
3
534
May 22
Iran has issued a NOTAM, banning flights in the western part of its airspace until Monday morning.
1
2
4
632
May 22
No consensus on the 2026 #NPTRevCon final document.
At the last plenary session of the 2026 #NPTRevCon the President says last night's text represents his best shot at a consensus document. But no consensus was reached. After 2015 and 2022 this is the next NPT review with no consensus reached
2
491
May 22
#NPTRevCon What would be better for the NPT ?; A Hollow Document or no document?
As the conference still debates the latest watered down Rev4 draft and has not agreed to it yet the real question is whether adopting another very weak document is better or worse than allowing the conference to end without one.
A thin document would avoid a third consecutive failure and keep the review process formally alive. Some limited procedural steps could still move forward, and it would prevent an immediate sense of institutional collapse.
However, the cost is credibility. A document this hollow , stripped of difficult issues and offering little beyond ritual language allows states to claim the process is still working while avoiding the hard choices the current environment demands. It rewards obstruction and gradually erodes the legitimacy of the review process itself.
A collapse, by contrast, would make the impasse impossible to ignore. It could serve as the necessary shock that forces NPT members to confront the reality that the current path has reached a dead end.
Without that shock, there is little pressure to accept that something more fundamental has to change — whether in the structure of the review process, expectations around transparency, or the willingness of nuclear-weapon states to engage on meaningful disarmament steps. At this point, the choice is between preserving the appearance of progress and acknowledging that the existing framework can no longer deliver substantive outcomes under present conditions.
1
1
488
May 22
#NPTRevCon NPT review conference ; New draft document Rev4 further waters down Rev3
Latest: no agreement yet on the watered down draft
On the Final Day of the NPT review conference the latest revised draft (CRP.4) shows further watering down of the already meager text rather than any substantive strengthening.
Disagreement over Iran reference
The most visible sign of ongoing disagreement is in paragraph 15, where the explicit reference to Iran
“Iran can never seek, develop or acquire any nuclear weapons”
has been placed in square brackets. This is classic NPT drafting: bracketed text means it remains contested and could still be removed before the conference closes today.
Beyond the Iran language, several notable retreats from the previous Rev3 draft stand out:
◾️The national reporting mechanism for nuclear-weapon states, which had been one of the few modestly forward-leaning elements in Rev3, has been significantly weakened. It is now limited to “the next Review Conference,” rephrased from “interactive discussions” to softer “in-person discussions and exchange of views,” and explicitly placed in private plenary settings. What was presented as a step toward greater transparency has been deferred and made less open.
◾️Specific language on the Zaporizhzhia Nuclear Power Plant and the IAEA Director General’s Five Concrete Principles has been removed. The text on attacks against nuclear facilities remains (para 33), but in more generalized form.
◾️A new preambular paragraph (viii) was added reaffirming the obligation of all states to comply with international law, including international humanitarian law — a modest addition likely tied to concerns over attacks on nuclear facilities.
The document is now only 7 pages long. For comparison, the 2010 NPT Review Conference produced a 46-page final document with detailed actions across all three pillars. Even by recent low standards, this is thin.
What’s missing is as revealing as what remains.
◾️There is no mention of New START’s expiration.
◾️No substantive treatment of Russia’s nuclear rhetoric and coercion in the context of its war in Ukraine.
◾️No reference to South Asian nuclear arsenals.
◾️Nuclear sharing and extended deterrence are touched on only in the most anodyne terms.
◾️The specific challenges posed by the current deterioration in great-power relations and the renewed political value placed on nuclear weapons by the nuclear-weapon states are largely avoided.This is not an accident.
It reflects a deliberate choice to strip out almost anything that would seriously discomfort any of the nuclear-weapon states in order to produce a consensus text.
The desperate attempts to avoid a third consecutive review conference failure (after 2015 and 2022) appears to have overridden any ambition for meaningful content.
Overall assessment
CRP.4 is a damage-limitation document, not a substantive one. It represents a further step back even from the already modest Rev3 draft. The parties have prioritized producing something, anything over advancing the Treaty’s core objectives.
This outcome is consistent with the broader trend: in an era of renewed great-power competition and increased reliance on nuclear weapons for security and status, the NPT review process is struggling to generate consensus on anything beyond the lowest common denominator.
The result is a text that protects the appearance of the regime while avoiding the difficult political choices required to strengthen it.Whether this minimal document is ultimately adopted today remains to be seen. Even if it is, it will be a thin and fragile consensus that does little to address the real pressures the Treaty currently faces.
link to latest draft: reachingcriticalwill.org/ima…
1
2
771
Brian McDonald B retweeted
May 21
Analysis
2026 NPT Review Draft CRP2 Rev3 Exposed: Polished Words that mask zero progress
The Treaty on the Non-Proliferation of Nuclear Weapons (NPT) is the supposed cornerstone of the global nuclear order. Signed in 1968, it promised to stop the spread of nuclear weapons, required the five recognised nuclear powers to eventually disarm under Article VI, and guaranteed everyone’s right to peaceful nuclear energy. Every five years the 191 states parties hold a Review Conference to check what’s actually been delivered.
The current 2026 Review Conference (27 April – 22 May) is in its final hours. After the total collapses of 2015 and 2022 (no consensus documents at all), diplomats are about to adopt CRP2-Rev3 (dated 21 May 2026) and will almost certainly spin it as a “success” because they avoided another outright failure. But a straight read of the 8-page draft shows the same old story: lots of ritual language, zero meaningful progress, and a complete detachment from real-world reality.
Preamble & Nuclear Disarmament (paras 1–13, pages 1–3)
The text opens with the usual lofty declarations — the NPT is the “cornerstone”, past commitments “remain valid”, and “a nuclear war cannot be won and must never be fought”. It “deeply regret[s] the lack of recent progress” on Article VI (para 3) and “urge[s]” the nuclear-weapon states to reduce and eliminate their arsenals. Yet New START expired in February 2026 with no successor in sight. The US wants China included in any new framework, Russia wants France and the UK at the table, and China rejects the whole idea.
The draft stays completely silent on this impasse and offers only vague “strategic risk reduction” measures (para 6) that “cannot substitute” for actual disarmament. Meanwhile all five nuclear powers are modernising, and some (China and France) are actively expanding. Even IAEA Director General Rafael Grossi has openly warned that we could soon see 20–30 nuclear-armed states if current trends continue. The document ignores that warning entirely.
Nuclear Non-Proliferation & the Two-Tier Double Standard (paras 14–24, pages 3–5)
Here the hypocrisy is blatant. Paragraph 16 singles out Iran: “Iran can never seek, develop or acquire any nuclear weapons.” But when it comes to attacks on safeguarded nuclear facilities (para 34, page 6), the text only expresses “grave concern” and “strongly urge[s]” everyone to refrain, without naming the US or Israel.
Worse, the draft is silent on how recognised nuclear states use their arsenals to enable aggression. Russia’s nuclear-backed invasion and annexation of parts of Ukraine shows exactly how possession of nuclear weapons gives impunity and creates a powerful incentive for other countries to want their own. The non-proliferation norm is being eroded from within by the very states the Treaty protects.
Middle East, Peaceful Uses & Universality (paras 25–38, pages 5–7)
The draft reaffirms the 1995 Middle East Resolution and calls for a WMD-free zone, but adds no new steps. On universality (para 37) it urges India, Israel and Pakistan to join “promptly and without conditions” and South Sudan “as soon as possible.”
North Korea gets the usual different treatment (para 24): it “cannot have the status of a nuclear-weapon State” and must fully denuclearise. Everyone knows this is detached from reality, Pyongyang learned the Libya and Ukraine lessons and will never give up its arsenal.
The Only “New” Thing (paras 39–45, page 8)
The sole concrete decision is a modest procedural tweak on structured reporting by nuclear-weapon states. Everything else is aspirational.
The Bigger Picture
Let’s be honest: the NPT has helped limit the number of nuclear-armed states for five decades, but that success was never the Treaty’s alone. Israeli strikes on Iraq’s Osirak reactor (1981) and Syria’s reactor (2007), plus sanctions and the regional environment that helped convince Libya to give up its programme in 2003, played major roles.
Today the bargain looks hollow. The original five nuclear powers used the NPT to lock in their monopoly and UN Security Council status, while paying lip service to disarmament they never delivered and have no intention to do so and every member knows that.
The draft repeats the same ritual phrases we’ve heard for 50 years, attaches no consequences to the recognised nuclear states, and pretends the rising proliferation pressures (South Korea, Poland, Japan, Saudi Arabia, Turkey) don’t exist.
We are about to get the third consecutive Review Conference with no meaningful outcome , just another weak consensus paper that will be hailed as “progress.” Most participants know the emperor has no clothes. They keep showing up every five years, pay lip service to a Treaty many no longer fully believe in, and hope the facade holds a little longer.
The real question is no longer whether the NPT can deliver real disarmament or stop proliferation. It’s whether the diplomatic community will ever admit the grand bargain is broken ,and focus on real solutions.
And will the diplomatic community dare to face the honest conclusion that in this time of eroding international frameworks and norms, and increasing use of might makes right great power competition that the NPT is basically dead.
What do you think, another five years of non proliferation theatre, or time for something different?
reachingcriticalwill.org/ima…
1
3
3
1,050
May 22
Today we remember… May their memories be a blessing. We love you Yaron and Sarah 💔 🇮🇱
They were full of dreams, full of plans together, fighting the good fight
But they were murdered in cold blood by Elias Rodriguez, as he was chanting "Free Free Palestine."
Murdered for supporting Israel
Murdered for simply existing
never forget their love.
never forget theri dedication.
never forget their their light.
May their memories forever be a blessing.
1
4
13
291