
Wife. Mom. Researching education concerns & helping parents. Host of the A Time To Stand podcast. This journey began in 2016 and it's why I homeschool. 🚫 WSCC
Joined April 2009
- Tweets 17,451
- Following 3,844
- Followers 13,769
- Likes 48,567
1,982 Photos and videos



The CDC has inserted themselves into education via the WSCC model of Community/Healthy Schools. The model is not transparent. They want children accessing psycho/social-emotional/medical/sexual/ reproductive/dental services at school. They want to remove parental consent/rights.

Grateful to join @4TiffanyJustice on the @Moms4Liberty podcast to introduce the alarming concerns of the WSCC model. The CDC and the many other coordinated groups investing into Community/Healthy Schools are usurping the role of parents and intruding into the family.
76
427
633
240,822
Kelly S. retweeted

Yes.
The ultimate betrayal of trust.
Jun 13

Senator Ron Johnson says some parents did everything they were told to do during COVID.
They trusted the experts, vaccinated their children, and then faced every parent’s worst nightmare.
“Imagine you’re one of those parents.”
“You believe in the lies.”
“You actually have your child vaccinated.”
“And then your child doesn’t wake up.”
“Imagine that.”
“It happened way more than 10 times.”
“Which is what FDA has acknowledged.”
@Senronjohnson @ChildrensHD @chdlive
1
12
35
1,262
Three SF Giants pitchers didn't give in to the manipulative demands for conformity so @outsports and @Scott_Wiener are trying to shame them. These critics should instead stop sex-denying sterilization and harmful mutilating surgeries and protect sex-based sports and spaces.
15h

Three SF giants pitchers disgraced themselves at the team’s Pride Night, weaponing the Pride rainbow and attacking the LGBTQ community.
outsports.com/2026/6/13/2413…
2
14
326
I love this! One January, in Tennessee, our Uber driver heard that I enjoy studying history and that I had always wanted to see Franklin, TN at Christmas. He kindly drove my family and I around, shared history, and ended by showing us the Christmas tree in Franklin. #America250
Jun 12

A wise man once said, if you want to hate America, watch the news. If you want to love America, drive across it.
These European World Cup tourists are experiencing the REAL America for the first time: not New York City or LA, but middle America and all its hospitality. 🇺🇸
1
1
12
1,131
Kelly S. retweeted

I spoke about Community Schools & Whole Child spending at the TX Republican Party Convention Leg Priorities on Thursday. Tx MUST get these programs out! @TexasGOP @Bentley4Texas @ZebraStrongMama @M4LHarris @mamaknowsbooks @cslape @CMooreFreedom @PriscillaWest77 @JulieABehling
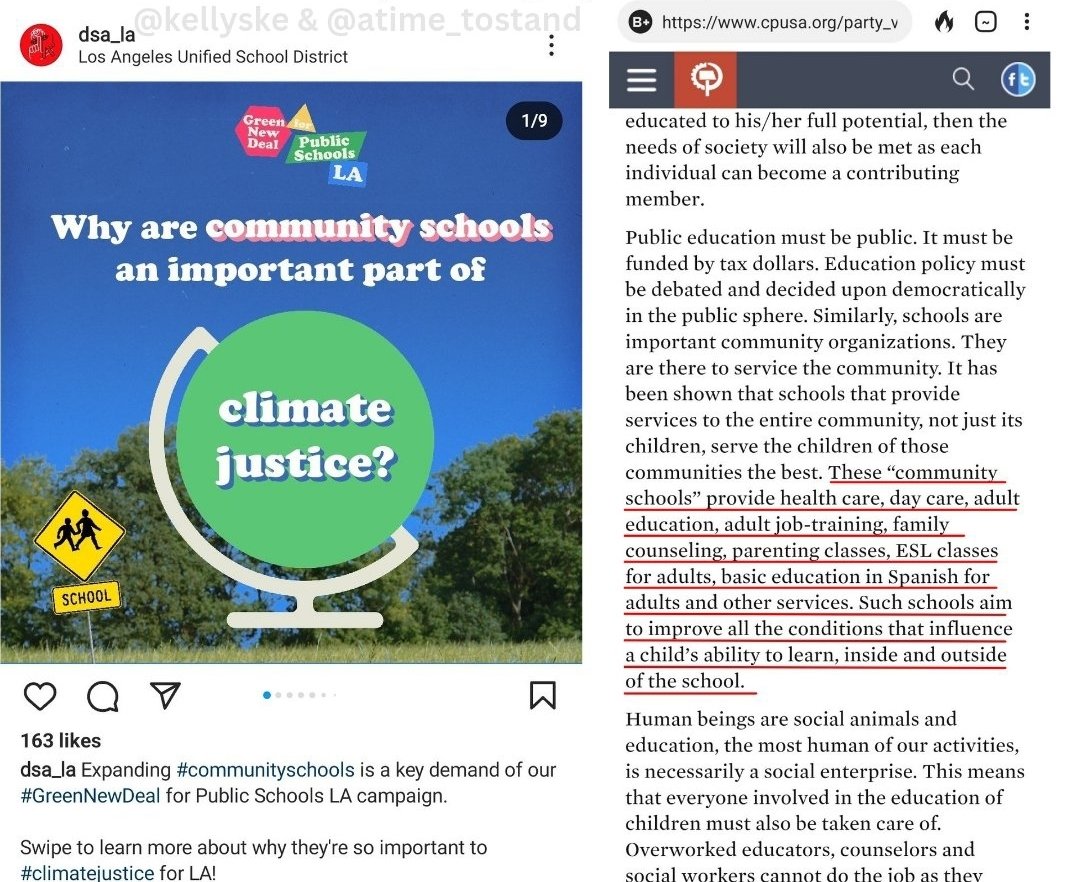
Communists and Democratic Socialists want every school to become a Community School.
Community Schools are marketed like the new envy in school transformation. But, it's a bait and switch.
cpusa.org/party_voices/the-c…
Join @JillSimonian and I as we discuss:
youtu.be/DBIhQ-6-GVo?si=3pde…
2
8
221
Kelly S. retweeted

In case you haven’t heard, a boy pretended to be a girl, entered the girls’ wresting tournament, and while wrestling put his fingers INSIDE a girl. A judge ruled that it’s all just a part of wrestling.
Will anyone EVER stand up for the girls????
117
1,021
4,447
36,319
Kelly S. retweeted

FOLLOW THE LAW or
FIND OUT 🇺🇸🇺🇸🇺🇸
@slf_liberty
@kimmiehermann
@Moms4Liberty
@KSAGOffice
Parents are DONE watching schools violate parental rights
Get onboard or
get out of the way 🎯🎯🎯

Schools should be places where students can focus on learning, not worry about their privacy being compromised. SLF applauds the Department of Education's action and hopes it sends a clear message to school districts across the country that Title IX protections must be upheld and students' privacy must come first.

1
4
9
348
Kelly S. retweeted

Jun 11
Taxpayers are funding a state-run leadership academy that requires public school principals to confess their racial sins, grade themselves on ideological purity, and then return to their buildings to implement race-based policies.

How did so many teachers and school administrators become so radically left wing? For many, it was DPI's Wisconsin Urban Leadership Institute training them to become "equity champions." @ColbeyDecker presents an eye-opening investigation. heartlandpost.com/wisconsin-…
6
11
19
1,443
Kelly S. retweeted

EPIC FAIL:
How activists used a massive gov’t-protected industry to invade YOUR life:
- force “gender” compliance
- give kids secret access
- bias doctors & nurses against elderly patients
- put women’s health at risk
Another 🔥 in-depth from @ColoradoDoctors’ Unpaid Intern🧑⚕️

WHEN EPIC ISN'T REALLY EPIC: How Gender Ideology Was Integrated into Epic Systems' Electronic Health Records
Epic Systems Corporation’s electronic health record (EHR) platform, used by approximately 41% of 🇺🇸 hospitals and historically as many as 80% of outpatient settings, as well as internationally, has systematically incorporated structured fields for self-identified gender identity that are separate from, and often displayed more prominently than, biological sex. The integration happened through a deliberate sequence of internal technical development at Epic, coordinated external advocacy from trans industry organizations, and federal regulatory requirements tied to incentive payments. The result is the Sexual Orientation and Gender Identity (SOGI) SmartForm, (sex) organ inventory tracking, visible patient banners and headers, automated SmartLinks, and configurable MyChart proxy access settings. These features treat gender identity as core, structured, queryable data embedded throughout clinical workflows, notes, portals, faxes, research queries, and national interoperability standards. To gender identity believers, nothing says “evidence-based medicine” quite like elevating subjective self-report to the level of immutable biology.
HOW IT STARTED
The internal catalyst at Epic was Janet Campbell, who joined the company in 2003 immediately after graduating from Carleton College with a computer science degree and additional coursework in gender studies. But, of course. Her first assigned project required building system rules to restrict diagnostic and billing codes according to recorded patient sex, for example, blocking orders for cervical examinations on patients whose record listed “male.” This work quickly revealed that Epic’s longstanding single “sex” field, limited since the company’s founding in 1979 to the options male, female, or unknown, was functionally "overloaded", as per Janet Campbell. It was seen to be simultaneously serving as a proxy for real sex or "sex assigned at birth", legal sex, and the emerging activist concept of gender identity. The resulting mismatches produced billing errors, inappropriate clinical alerts, and unreliable data for research or quality reporting, problems that, in a less ideological era, might have been solved by simply respecting biological reality rather than inventing new fields to accommodate delusuins.
In approximately 2004–2005, Campbell volunteered to deliver an internal educational presentation during Epic’s regular workplace talk series. One slide stated verbatim: “Epic is almost completely unable to deal with this level of complexity, and neither is the medical profession, for that matter.” Sure, Jan. By January 2012 she had posted an internal wiki page proposing a two- or three-step data-capture sequence: sex assigned at birth, legal sex, and gender identity. A cross-functional workgroup was assembled that included several "transgender" and "non-binary" Epic employees - its stated purpose was to assist customers with implementation. In 2013 the group produced and distributed a “SOGI Strategy” handbook that supplied both technical instructions and sections on "transgender cultural competence" and the distinction between identity and sex, helpfully ensuring that every hospital using the system received a gentle primer on why feelings should sometimes trump chromosomes.
INFLUENCE OF THE TRANS INDUSTRY
The external pressure that accelerated these changes came from a sustained advocacy campaign. The coalition involved represented a wide network of LGBT health, HIV advocacy, and related organizations, with prominent leadership from The Fenway Institute at Fenway Health. In January 2013 this coalition of 145 leading LGBT and HIV/AIDS organizations submitted a formal public comment to the Office of the National Coordinator for Health Information Technology (ONC) urging inclusion of sexual orientation and gender identity (SOGI) data collection in Meaningful Use guidelines. Early in 2014 the same network expanded to 153 organizations and submitted recommendations asking ONC to direct the National Library of Medicine to develop new SNOMED code sets specifically to support accurate and effective SO/GI data collection in certified EHRs. These submissions formed part of a broader effort to embed SOGI capacity within the proposed 2015 Edition Certified EHR Technology (CEHRT) criteria for Meaningful Use Stage 3. Because when biology proves stubborn, the next best step is apparently to lobby the government to reprogram the nation’s medical software. Fenway Health, operating through its Fenway Institute and National LGBTQIA Health Education Center, functioned as the central technical and policy coordinator.
As early as 2011, Fenway had begun testing two-step gender identity questions (gender identity asked first, followed by sex assigned at birth) at its own federally qualified health center. In roughly 2012 it published the policy brief “How to Gather Data on Sexual Orientation and Gender Identity in Clinical Settings,” which formalized the two-step approach originally developed by the Philadelphia Transgender Health Advocacy Coalition in 1997 and later endorsed by UCSF’s Center of Excellence for Transgender Health. Fenway partnered with the Center for American Progress on the “Do Ask, Do Tell” project, releasing online toolkits explicitly aimed at EHR vendors and providers. In 2014 Sean Cahill, PhD (Director of Health Policy Research at the Fenway Institute) co-authored key papers and policy statements, including the PLoS One article “Sexual Orientation and Gender Identity Data Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities,” which framed SOGI collection as essential for equity and disparity reduction. Fenway supplemented these writings with slide decks, tip sheets, and formal regulatory comments that repeatedly positioned SOGI capacity as a NON-NEGOTIABLE REQUIREMENT FOR FEDERAL CERTIFICATION 🚩, turning a contested religious belief at best into a certification checkbox.
IT'S ALWAYS THE GOVERNMENT
These advocacy efforts aligned precisely with federal rulemaking. The 2015 ONC and Centers for Medicare & Medicaid Services (CMS) Meaningful Use/Promoting Interoperability final rules mandated that certified EHRs possess the technical capacity to record, store, change, and retrieve structured SOGI data in order to qualify for incentive payments. The requirement applied across approximately 78 percent of outpatient clinics by 2018. In 2016 the Health Resources and Services Administration (HRSA) further embedded the expectation by adding SOGI fields to the Uniform Data System (UDS) reporting obligations for all federally qualified health centers. The combination of coalition pressure and incentive-linked certification created powerful compliance incentives for both vendors and health systems, because nothing motivates hospitals quite like the threat of lost federal dollars for failing to ask patients about their feelings. It's a clear, breathtaking case of policy winning over ethics in the medical field.
EXPANSION WITHIN
Inside Epic, Campbell’s initial workgroup scaled into a 25-person “Volunteer Army.” The team performed a full-system audit and remapped hundreds of references to the original “sex” field throughout patient headers, laboratory normal ranges, genetic pedigrees, clinical decision-support logic, and other modules. Campbell characterized the overhaul as “like the Y2K of the health record.” Development milestones followed in rapid succession: a two-item gender identity update released to clinical customers in June 2016, followed by the complete SOGI SmartForm in November 2016. The SmartForm is a guided questionnaire triggered by clicking the gender or age line in the patient Storyboard or during registration, nursing assessment, or clinical encounters. It begins by recording gender identity; any mismatch with recorded sex automatically prompts follow-up questions on pronouns (including they/them and additional options), transition steps, and an organ inventory that distinguishes organs present at birth from those present currently, because the most reliable way to practice “precision medicine” is apparently to ask patients what their body parts used to be while politely ignoring what they actually are. This also serves as proof of the linguistic weaponization trans activists indulge in - conflating legitimate things like kidney donation with calling an inverted penis lined with scrotal skin a vagina. It's part of the tactic to normalize grotesque and experimental "transgender surgeries" as "just routine medical procedures".
Further refinements to the EPIC EHR in 2017–2018 introduced explicit distinctions among legal sex, gender identity, sex assigned at birth, and “sex for clinical use,” while chosen names and pronouns were propagated system-wide via SmartLinks. By mid-2017 Campbell reported that 10–20 percent of Epic customers had activated the updates. The captured data is structured rather than free-text, making it visible and actionable: chosen name, gender identity, and pronouns appear in patient banners and headers; SmartLinks automatically insert the information into notes, schedules, faxes, and reports. Patients, including minors as young as 12 in many implementations, can enter or update these fields directly through the MyChart portal; changes become part of the official record without mandatory clinical verification, because self-ID is apparently so infallible that no second opinion from a doctor is required. Hospitals frequently incorporate SmartForm completion rates into quality metrics, disparity dashboards, and DEI scorecards, and staff training modules draw heavily on Fenway’s cultural-competence materials.
Campbell has explained the design rationale in public remarks. In 2017 she stated: “Our goal is that patients get the right and appropriate treatment no matter who they are.” On the decision for universal collection she added: “I think that starting to collect this information from everyone will normalize it in many people’s eyes. It’s not that we’re asking certain people whether they happen to be trans, we’re just asking everybody.”
The trans activism is ever present, presented dishonestly. In the August 31, 2022, Clinical Architecture Informonster Podcast (Episode 23: “Discussing Gender Harmony”), recorded with Fenway’s Chris Grasso, Campbell explained that the original single field “had become overloaded and was asked to do double duty.” She described the 2017 safety corrections, such as revised creatinine-clearance calculations based on mismatched legal sex, and noted broader applicability: “The work that we’re doing here will benefit the entire patient community… It’s not just transgender patients who want to be called by a name that’s different than the name on their birth certificate.” Regarding documentation she advised: “If a patient isn’t living their gender identity, don’t document that information in those fields… the system will take your word for it and will put that everywhere.” Right, all that confusion and hoop-jumping due to the religious and fanatical belief in "gender identity", trying to get ahead of the chaos being caused. Epic continues to participate in the HL7 Gender Harmony Project, which has produced a national interoperability standard separating recorded sex/gender, gender identity, and “sex for clinical use,” each with validity periods. The SOGI and organ-inventory data therefore support anatomy-based alerts while preserving identity fields as the primary display element, because the clearest way to avoid clinical confusion is apparently to make identity the banner headline and biology the optional footnote. Gender ideologues purposely calculate to supercede the practice of ethical medicine to bolster their claims, reality be damned.
TARGETING MINORS IS NOT ACCIDENTAL
MyChart proxy access for minors remains configurable by each health system and is age-tiered. Common configurations include independent portal access at age 12 (UF Health Shands), “Teen Plus” limited parental views (Wellstar), and parent-teen access at age 13 (UNC). "Sensitive sections" like SOGI data, preferred pronouns, organ inventory, and transition-related notes, CAN BE HIDDEN FROM PARENTS, frequently extending beyond the original intent of adolescent privacy statutes written for STIs or contraception. A 2025 Do No Harm @donoharm report catalogued these settings and quoted Epic’s own documentation, which states that proxy access “changes as they get older” according to each organization’s interpretation of privacy laws. Vague enough. The cumulative architecture produces a workflow in which gender-identity documentation is routine, frictionless, and self-reinforcing, marketed to the very young and old alike.
DECLINES TO ANSWER
If elderly patients are confused about "personal pronouns", they are marked as "Declined to answer" in a prominent manner in their profiles that anyone opening their chart can see. I have seen this happen to patients with dementia! This phrasing of "refused to cooperate" is meant to create bias in the minds of the clinician that the patient is difficult, and try to force compliance with gender ideology in both the doctor and the patient. Clinicians encounter prompts in core interfaces, data auto-propagates across the record and external systems, and non-use of the features can register as incomplete documentation or failure to meet incentive or equity metrics. These dubious metrics have converted advocacy goals into certification requirements. The outcome is a dominant EHR platform that has embedded self-identified gender identity as a core element across millions of patient records, completely ignoring evidence-based safeguards.
PATIENT SAFETY CONCERNS, THE ULTIMATE EPIC FAIL
Even in electronic health record systems where biologic sex, legal sex, and gender identity are all separately and clearly documented, significant patient-safety concerns remain because downstream clinical systems frequently fail to operationalize those distinctions consistently. Multiple health systems and informatics groups have documented that laboratory software, radiology workflows, preventive screening algorithms, insurance systems, and clinical decision-support tools often still rely on a single operative sex variable despite more sophisticated chart architecture.
At Geisinger Health System, clinicians and informatics staff described needing extensive custom modifications to Epic because standard workflows could not reliably coordinate birth sex, organ inventory, hormone exposure, and preventive screening logic simultaneously. The Veterans Health Administration similarly acknowledged tension between visibility of natal sex and identity-related workflows, warning that suppressing or obscuring biologic sex could impair preventive care and emergency clinical reasoning.
Real-world failures described in the literature include biologically female patients losing automated cervical cancer reminders after administrative sex changes, insurance denials for Pap smears or PSA testing when legal sex conflicted with anatomy, pregnancy-related safeguards failing because workflows operationalized identity-facing fields incorrectly, and laboratory systems inconsistently applying sex-based reference ranges for hemoglobin, creatinine, eGFR, CK, and troponin. Pathologists and laboratorians have repeatedly noted that current systems struggle to interpret altered hormone states because a testosterone-treated female remains biologically female while exhibiting partial shifts in selected analytes, creating ambiguity that simplistic identity-based categorization cannot safely resolve.
Researchers in medical AI and informatics have additionally warned that inconsistent handling of sex, gender identity, legal sex, and hormone exposure produces “sex/gender slippage” in datasets, threatening the reliability of epidemiology, predictive algorithms, and machine-learning models. The central concern raised by clinicians focused on sex-based medicine is therefore not merely missing data fields, but that medicine remains fundamentally organized around biologic sex while many EHR systems and institutional workflows operationalize sex-related variables inconsistently, creating opportunities for diagnostic error, screening failures, inappropriate clinical decision support, and degraded research quality even when all demographic categories are technically present and clearly separated.
The corruption of Epic EHR demonstrates how gender ideology became medical infrastructure when the right mix of activists, incentives, federal cooperation, and software engineers decided that their unfounded beliefs trump reality, endangering patient healthcare in the process. Your mind and body are both the donor organs and the subsequent profit to the trans industry. An EHR is a tool and repository that helps maintain and improve medical records. Using it to cement the nebulous concept of gender identity as fact is subjecting the material reality of patients and doctors to dangerous process errors and repeated trans industry indoctrination. Get your act together, EPIC, and put patient safety first, before it's too late.
SOURCES AND REFERENCES
- Ingraham N, et al. Overcoming technical and cultural challenges to delivering equitable care for LGBTQ individuals in a rural, underserved area. JAMIA Open. 2022.
PMC article
- Klee A, et al. Evolving Sex and Gender in Electronic Health Records. Fed Pract. 2018.
PMC article
- Greene DN, et al. Challenges in Transgender Healthcare: The Pathology Perspective. Clin Chem. 2016.
PMC article
- Cheung AS, et al. Approach to Interpreting Common Laboratory Pathology Tests in Transgender Individuals. J Clin Endocrinol Metab. 2021.
Oxford Academic article
- Keyes O, et al. Sex trouble: Sex/gender slippage, sex confusion, and sex obsession in machine learning using electronic health records. Patterns. 2022.
ScienceDirect article
- Kannan V, et al. Challenges with Accuracy of Gender Fields in Identifying Transgender Patients in Electronic Health Records. AMIA Annu Symp Proc. 2020.
PMC article
- Collecting Sexual Orientation and Gender Identity Data in Electronic Health Records. National Academies Press.
NCBI Bookshelf
- Wired.com, “The Battle to Get Gender Identity Into Your Health Records” (June 30, 2017) – Campbell’s timeline, internal presentation quote, 2012 wiki proposal, workgroup formation, 2013 SOGI Strategy handbook, Volunteer Army audit, Y2K comparison, and technical rollout details.
- Isthmus.com, “UW Health aims to be more sensitive to gender identity” (July 6, 2017) – Campbell’s direct quotes on the SmartForm purpose, normalization through universal collection, and adoption statistics (10–20% of customers, 20–40 providers).
- Clinical Architecture Informonster Podcast, Episode 23: “Discussing Gender Harmony” (August 31, 2022) – Full transcript excerpts of Campbell discussing the overloaded single sex field, 2017 clinical safety fixes, HL7 Gender Harmony collaboration, privacy advice, and benefits for all patients; includes joint discussion with Fenway’s Chris Grasso.
- Do No Harm report, “Parental Access to Children’s Medical Records” (October 2025) – Details on Epic SOGI SmartForm mechanics, organ inventory, MyChart proxy access configurations at specific health systems (UF Health Shands, Wellstar, UNC), and analysis of concealment practices beyond legal minimums.
- Fenway Health / National LGBTQIA Health Education Center, “Collecting Sexual Orientation and Gender Identity (SO/GI) Data in Electronic Health Records” (2016 PDF) – Implementation toolkits, clinical workflows, and ties to Meaningful Use / HRSA requirements.
- Cahill et al., “Sexual Orientation and Gender Identity Data Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities” (PLoS One, 2014) – Core advocacy paper outlining the case for SOGI inclusion.
- Fenway Health, “How to Gather Data on Sexual Orientation and Gender Identity in Clinical Settings” (policy brief, ~2012) – Early testing protocols and two-step question recommendations.
- Center for American Progress / Fenway Institute joint statement (October 7, 2015) – Praise for the 2015 ONC/CMS Meaningful Use rules requiring SOGI capacity in certified EHRs.
- Fenway Health “Do Ask, Do Tell” toolkit and related 2014–2016 publications – Broader SOGI EHR advocacy, promotion of standardized questions, and collaboration with other groups.
ONC/CMS 2015 Edition Certified EHR Technology (CEHRT) Criteria and Meaningful Use/Promoting Interoperability final rules – Federal requirements for SOGI data capacity in certified systems, tied to incentive payments.
- Additional cross-referenced context from HRSA Uniform Data System (UDS) updates (2016), HL7 Gender Harmony Project documentation, and public Epic customer implementation examples (e.g., University of Wisconsin, Geisinger). All information is drawn exclusively from publicly available records as of 2025.
- Cahill S. “Sexual Orientation and Gender Identity Data Collection Update: U.S. Government Takes Steps to Promote Sexual Orientation and Gender Identity Data Collection Through Meaningful Use Guidelines.” LGBT Health (2014/2016 update) – Details on the 153 LGBT and HIV groups’ 2014 recommendations to ONC for SNOMED codes and the 2013 public comment from 145 organizations.
- Cahill S, Makadon H. Related policy briefs and Fenway Institute publications (2012–2016) – Documentation of coalition advocacy, two-step questions, and EHR implementation guidance.
#sexnotgender #genderidentity #epicEHR #epic #epicfail #ehr #medicalethics #MedTwitter #MEDX #donoharm #safety #propaganda
3
31
61
5,759
Kelly S. retweeted

Jun 11
Unfortunately not hyperbole.
Get informed.
Parent Alert l, via @prageru
Thank you to everyone who has already tuned in! Here's the new link to my full interview with @JillSimonian of @prageru:
youtu.be/DBIhQ-6-GVo?si=3pde…
1
2
175
Communists and Democratic Socialists want every school to become a Community School.
Community Schools are marketed like the new envy in school transformation. But, it's a bait and switch.
cpusa.org/party_voices/the-c…
Join @JillSimonian and I as we discuss:
youtu.be/DBIhQ-6-GVo?si=3pde…
1
8
13
576
Kelly S. retweeted

Jun 10
If you have children, WATCH:
👀
Thank you to everyone who has already tuned in! Here's the new link to my full interview with @JillSimonian of @prageru:
youtu.be/DBIhQ-6-GVo?si=3pde…
1
5
181
Thank you to everyone who has already tuned in! Here's the new link to my full interview with @JillSimonian of @prageru:
youtu.be/DBIhQ-6-GVo?si=3pde…
1
10
25
4,958
Kelly S. retweeted

Jun 10
@CivilRights finds UC Davis Med School’s deliberate use of race “proxies” in admissions illegal & shocking. Despite lower average GPA & MCAT scores, black or Hispanic admission rates were 2-9x higher than whites or Asians. Future doctors must be chosen based on skill, not race!
justice.gov/opa/pr/justice-d…
156
1,078
3,786
114,547
Thank you to everyone who has already tuned in! Here's the new link to my full interview with @JillSimonian of @prageru:
youtu.be/DBIhQ-6-GVo?si=3pde…
3
5
274
Kelly S. retweeted
Kelly is an increasingly recognized expert on Community Schools.
This is an innocent-sounding ploy to squeeze out families.
Don't miss this important interview tomorrow! I joined @JillSimonian of @prageru to discuss the Full-Service Community School agenda. Set your notification to livestream tomorrow at 10:30am PT, 1:30pm ET 👇
youtube.com/watch?v=P4FZQ7xp…
1
2
13
344
Don't miss this important interview tomorrow! I joined @JillSimonian of @prageru to discuss the Full-Service Community School agenda. Set your notification to livestream tomorrow at 10:30am PT, 1:30pm ET 👇
youtube.com/watch?v=P4FZQ7xp…
6
32
74
13,491
Thank you to everyone who has already tuned in! Here's the new link to my full interview with @JillSimonian of @prageru:
youtu.be/DBIhQ-6-GVo?si=3pde…
1
10
25
4,958
Thank you everyone for tuning in! Here's the new link to our full interview:
youtu.be/DBIhQ-6-GVo?si=3pde…
Don't miss this important interview tomorrow! I joined @JillSimonian of @prageru to discuss the Full-Service Community School agenda. Set your notification to livestream tomorrow at 10:30am PT, 1:30pm ET 👇
youtube.com/watch?v=P4FZQ7xp…
3
12
519
Kelly S. retweeted

Jun 10
Tune in now! @kellyske @prageru to discuss the dangers of the #CommunitySchools model infecting our schools.
Don't miss this important interview tomorrow! I joined @JillSimonian of @prageru to discuss the Full-Service Community School agenda. Set your notification to livestream tomorrow at 10:30am PT, 1:30pm ET 👇
youtube.com/watch?v=P4FZQ7xp…
1
1
6
259