
Agence du numérique en Santé @esante_gouv_fr
Joined June 2007
- Tweets 6,601
- Following 5,733
- Followers 1,574
- Likes 34,425
150 Photos and videos







Laurent Joubert retweeted

Announcing a new division of Midjourney called "Midjourney Medical"
1,659
3,026
25,271
7,427,420
Laurent Joubert retweeted

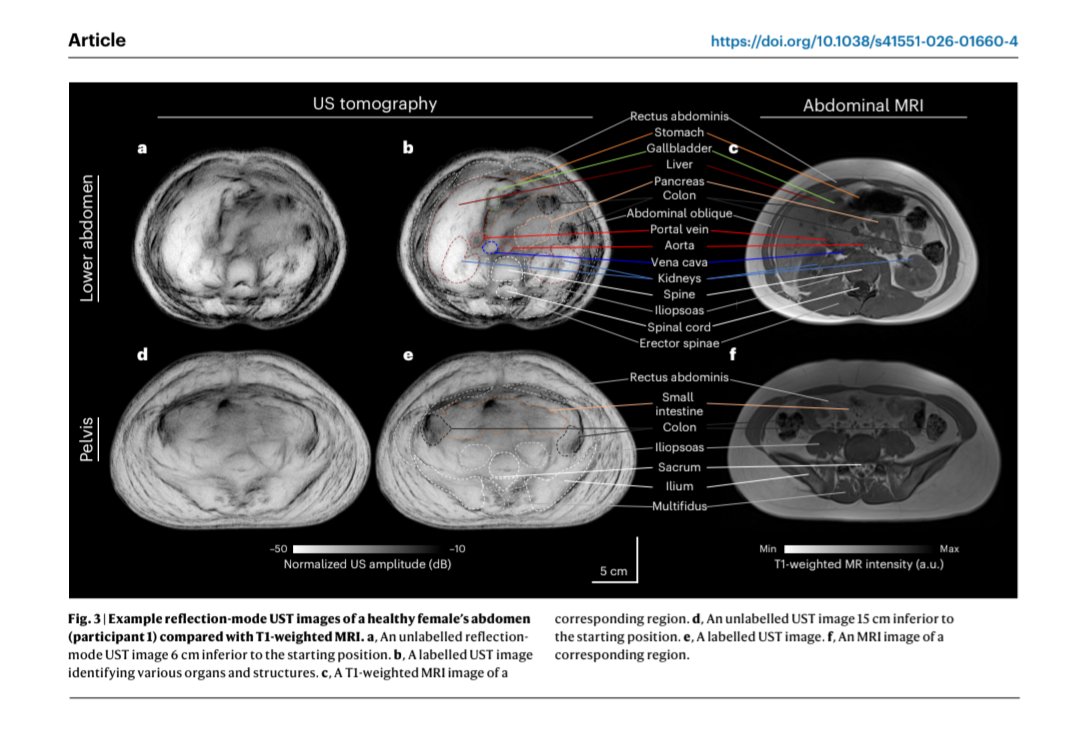
Pros: Radiation-free, magnet-free, fast and low-cost
Cons: Requires person to sit in a water immersion tank, and currently has coarser resolution than CT/MRI
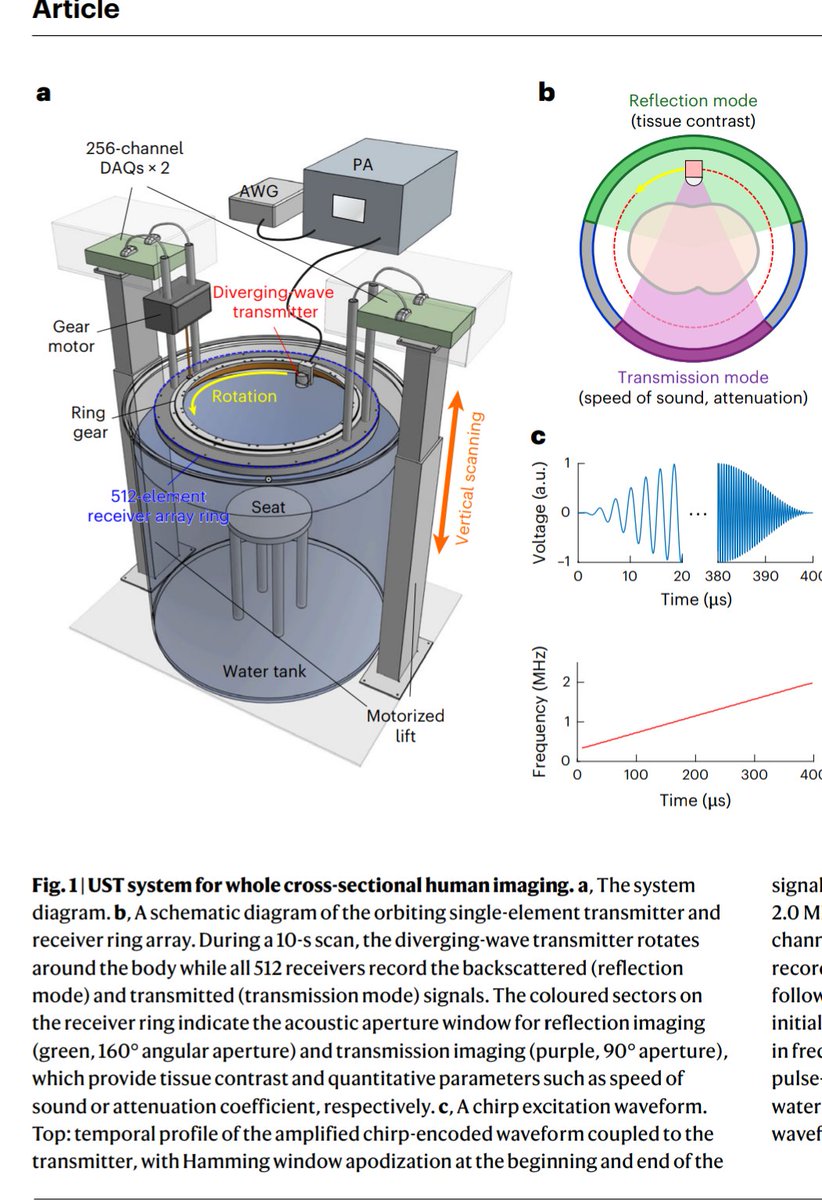


This recent paper is super interesting...
Using ultrasound imaging to generate images of the entire in vivo human cross-section in the abdomen and thighs
Basically trying to do CT/MRI-like imaging but using ultrasound!
Ultrasound imaging is highly underrated :)
43
100
1,508
146,539
Laurent Joubert retweeted

Jun 16
2
6
16
3,686
Laurent Joubert retweeted

Jun 12
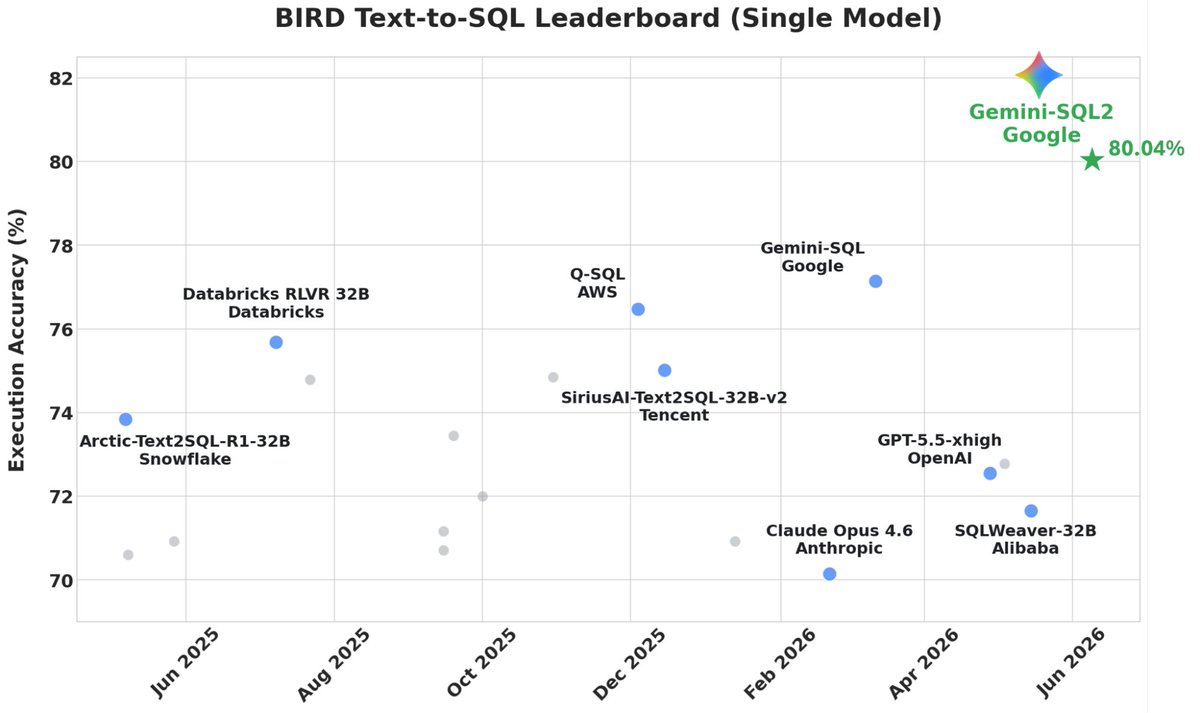
🚀 Introducing Gemini-SQL2, our breakthrough text-to-SQL capability powered by Gemini 3.1 Pro! We've achieved state-of-the-art results on the highly competitive BIRD benchmark, translating natural language into execution-ready SQL queries. 🧵👇
133
629
6,741
674,733

Laurent Joubert retweeted

Jun 5
Homunculus F³ (Full Force Feedback) haptic glove coming soon 😁
10
19
144
30,635
Laurent Joubert retweeted

Jun 3
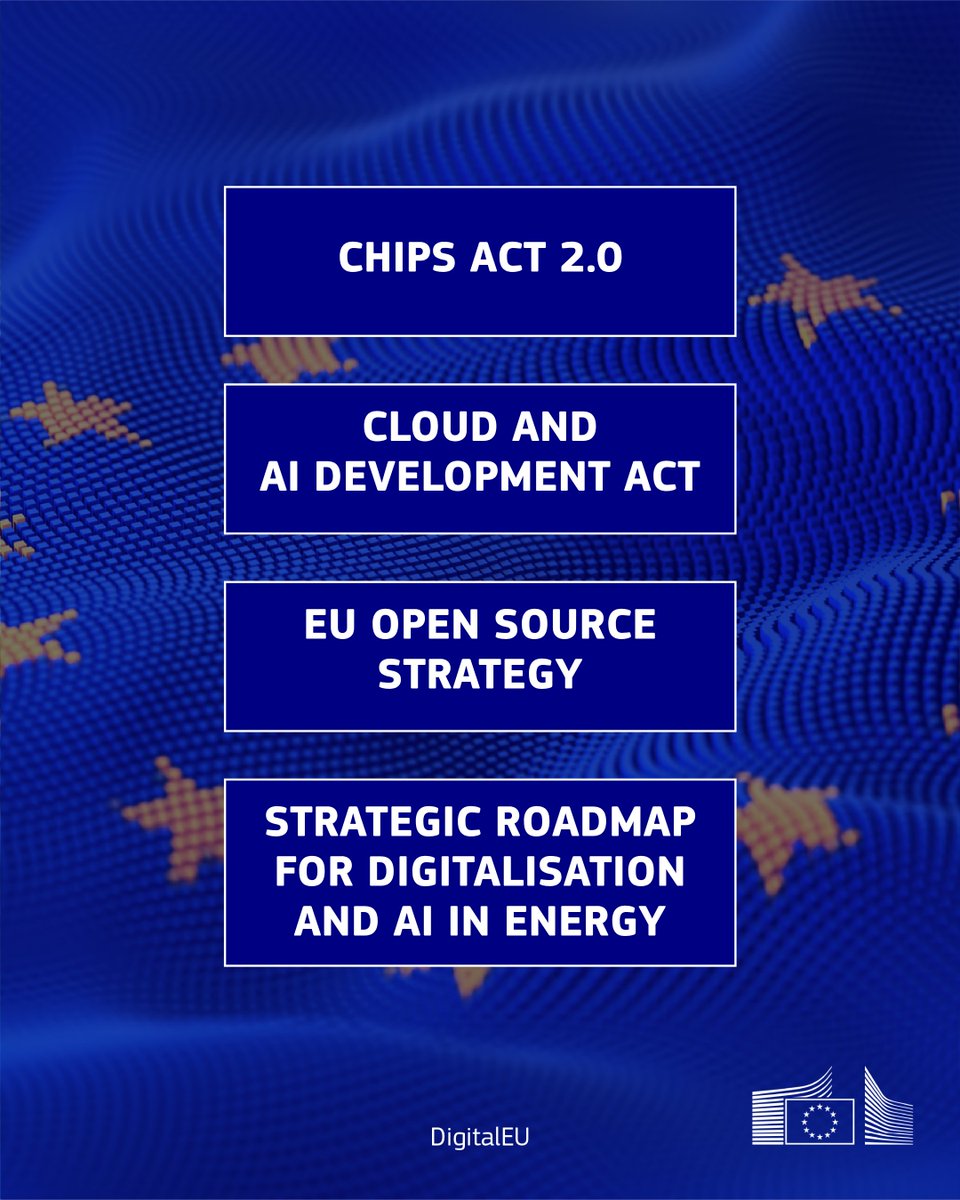
🇪🇺 We are building the future...
The new Technological Sovereignty Package will allow Europe to develop, control and scale up critical technologies ↓

30
49
138
8,446
Laurent Joubert retweeted

May 29
Robostral can now follow natural language instructions. It responds to voice commands and pointing. It is also getting better at fine-grained manipulation where precise force control matters. It generalizes to new objects and tasks not present in the training data.
27
67
485
50,429
Laurent Joubert retweeted

May 28
NEW RELEASE:
Today we're releasing CortexMAE: a family of fMRI foundation models trained on 2.1K hours of open fMRI data.
We're also releasing Brainmarks: an open benchmark suite for evaluating fMRI foundation models.
Full paper is on arXiv (accepted to ICML 2026)
A thread:
4
44
202
40,459
Laurent Joubert retweeted

May 28
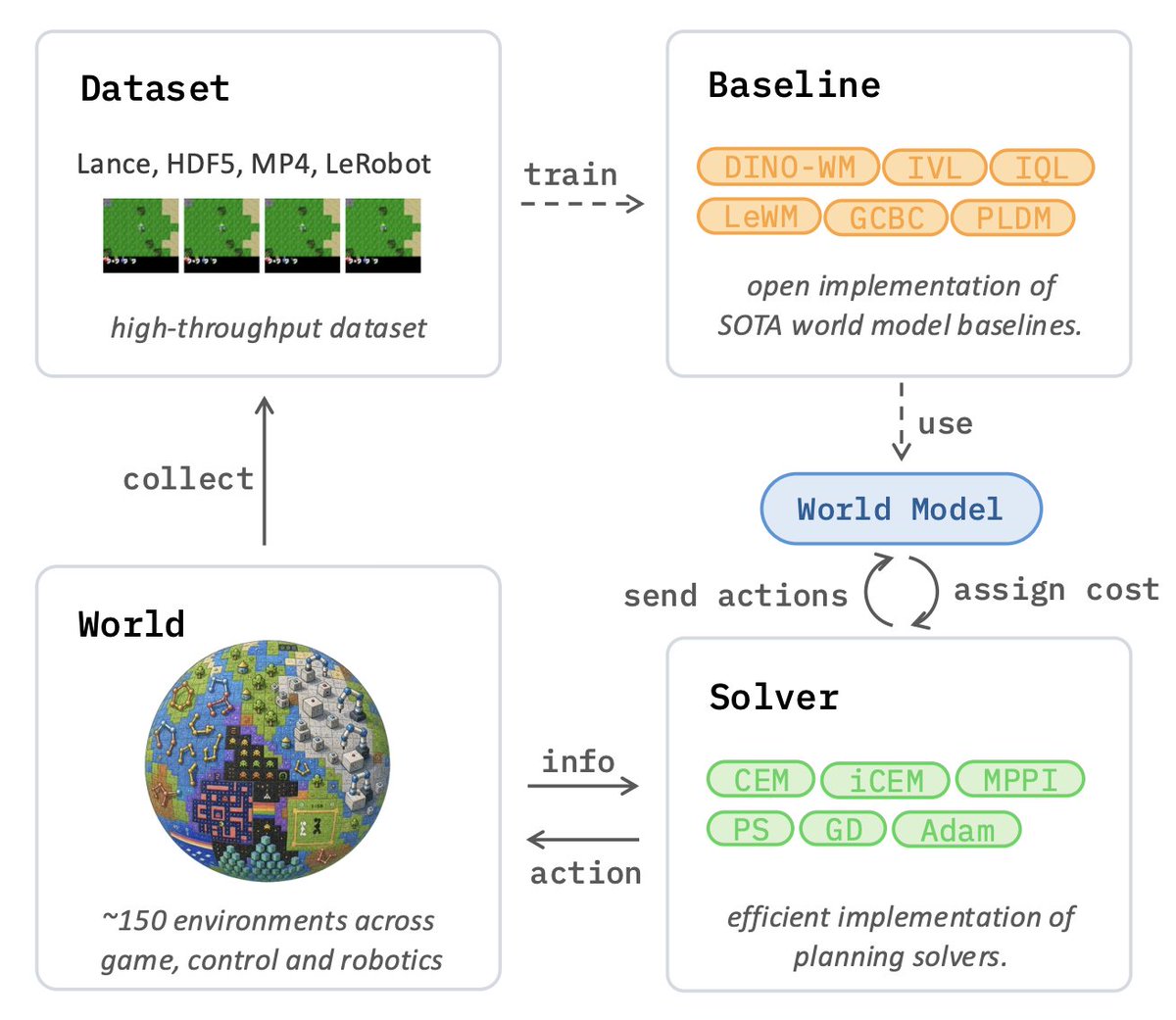
Would you like to join the research effort on JEPA and World Models easily?
After a full year of hard work, we’re excited to finally release stable-worldmodel:
an open-source, scalable platform built to accelerate JEPA & World Model research!
📄: github.com/galilai-group/sta…
40
274
1,819
113,621
Laurent Joubert retweeted

May 27
Introducing the newest Coral board, for efficient, on-device AI!
Check out the demos in the video:
- On-board speech translation
- Natural language controlling hardware
- Vision & sound generating music
183
748
7,739
1,382,593
Laurent Joubert retweeted

May 20
new release for text-to-cad, an open source CAD harness and skills for codex / claude:
- mechanism validation (go from text prompt to functional mechanical design)
- parameters animations for step files
- extended sdf, srdf, urdf support
3k stars, 10k downloads, we cooking
52
252
2,665
251,956
Laurent Joubert retweeted

May 20
What hardware actually powers open-source AI?
Not benchmarks.
Not vendor marketing.
Real-world community usage.
We’re launching @huggingface Hardware:
→ trending GPUs & CPUs
→ VRAM distribution
→ inference hardware trends
→ what the OSS AI ecosystem really runs on

41
71
414
81,031
Laurent Joubert retweeted

May 19
Personal update: I've joined Anthropic. I think the next few years at the frontier of LLMs will be especially formative. I am very excited to join the team here and get back to R&D. I remain deeply passionate about education and plan to resume my work on it in time.
7,990
11,145
150,258
27,595,169
Laurent Joubert retweeted

May 13
Le #CERN rend open-source sa librairie de composants électroniques pour le logiciel KiCAD. Disponible via Gitlab, elle contient des données pour plus de 17000 composants électroniques, y compris des symboles schématiques et des empreintes de circuits.
gitlab.com/ohwr/cern-kicad-l…
7
225
1,089
49,285
Laurent Joubert retweeted
May 12
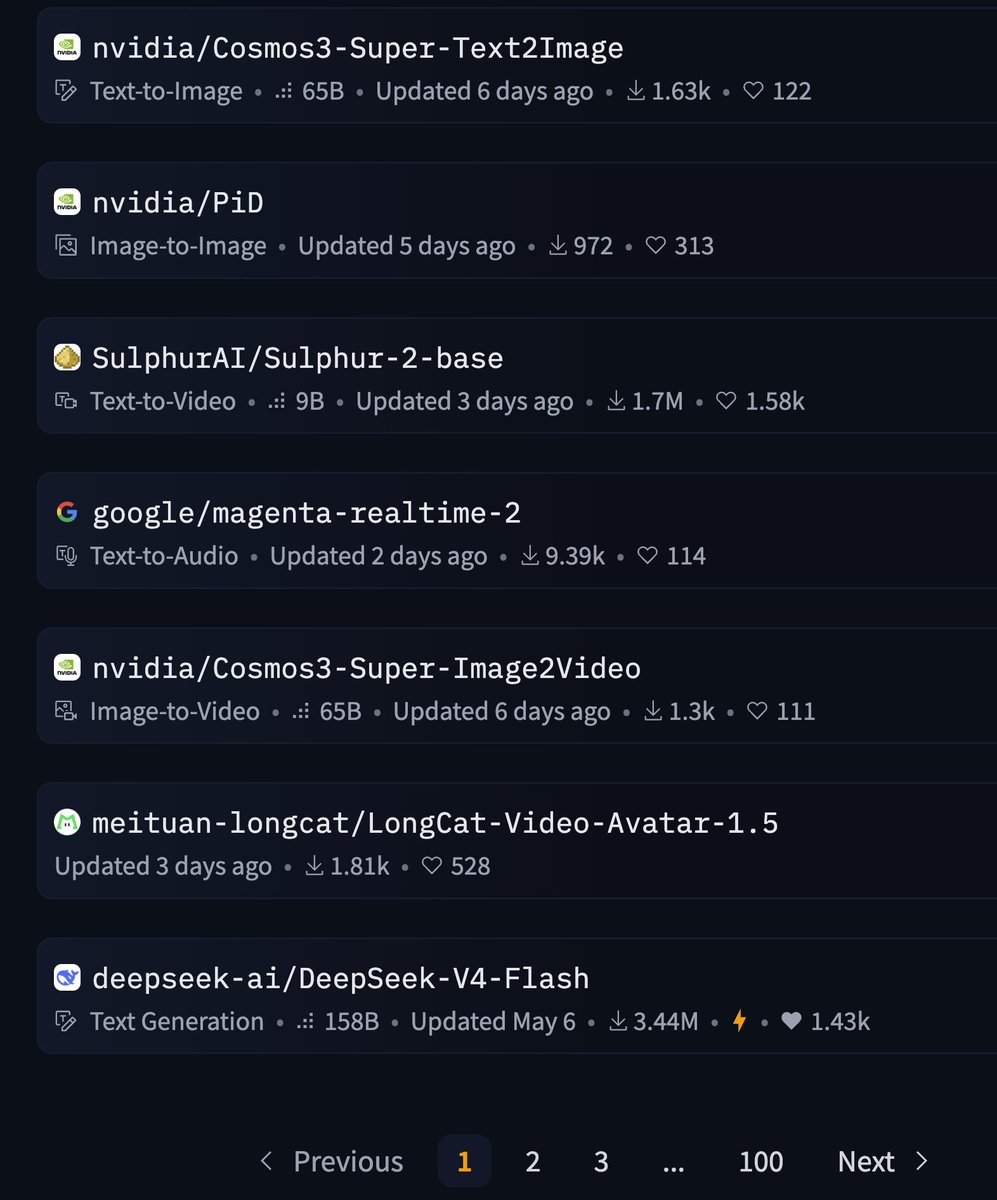
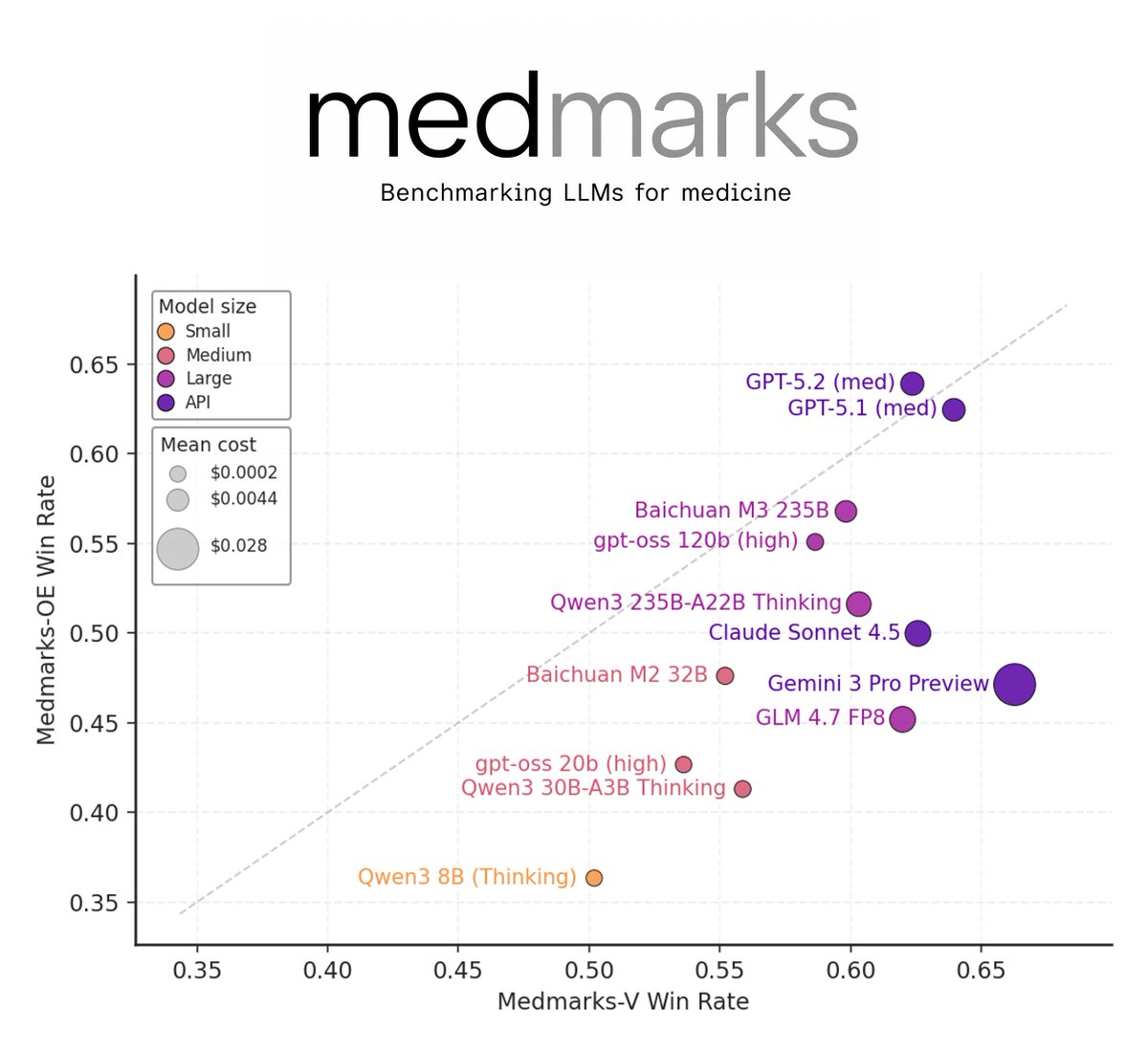
We're excited to release Medmarks v1.0 a technical report!
This is an update to our Medmarks benchmark suite, the largest open-source automated suite for evaluating the medical capabilities of LLMs.
We added 10 benchmarks (20→30) and 15 models (46→61) to the leaderboard!
3
26
96
41,498

DS4 running on DGX Spark (GB10 / CUDA), private branch for now. 12 tokens/sec, the memory bandwidth is limited in this system, at 270GB/sec. But prefill is ways more alighed to M3 Max at ~200 t/s. I'll release when more mature, but it is almost sure that it will get merged.
49
73
786
83,514
Laurent Joubert retweeted

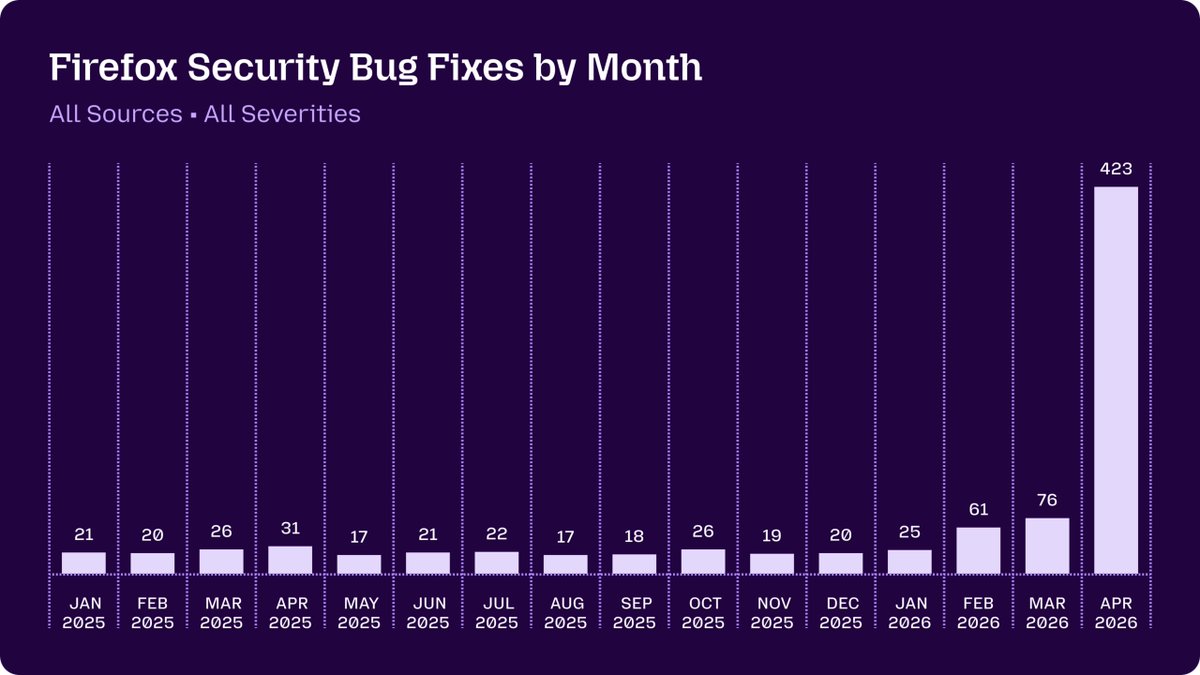
May 7
With the help of Claude Mythos Preview, the Firefox team fixed more security bugs in April than in the past 15 months combined.
344
1,256
15,471
1,488,205
Laurent Joubert retweeted

May 4
I wrote Deep Learning with Python to be the definitive guide to how deep learning works and how to best make use of it. Tens of thousands of people got their career start via this book. 120,000 copies sold, and downloaded by millions more.
And now it's free to read online: deeplearningwithpython.io/
82
557
3,932
719,533

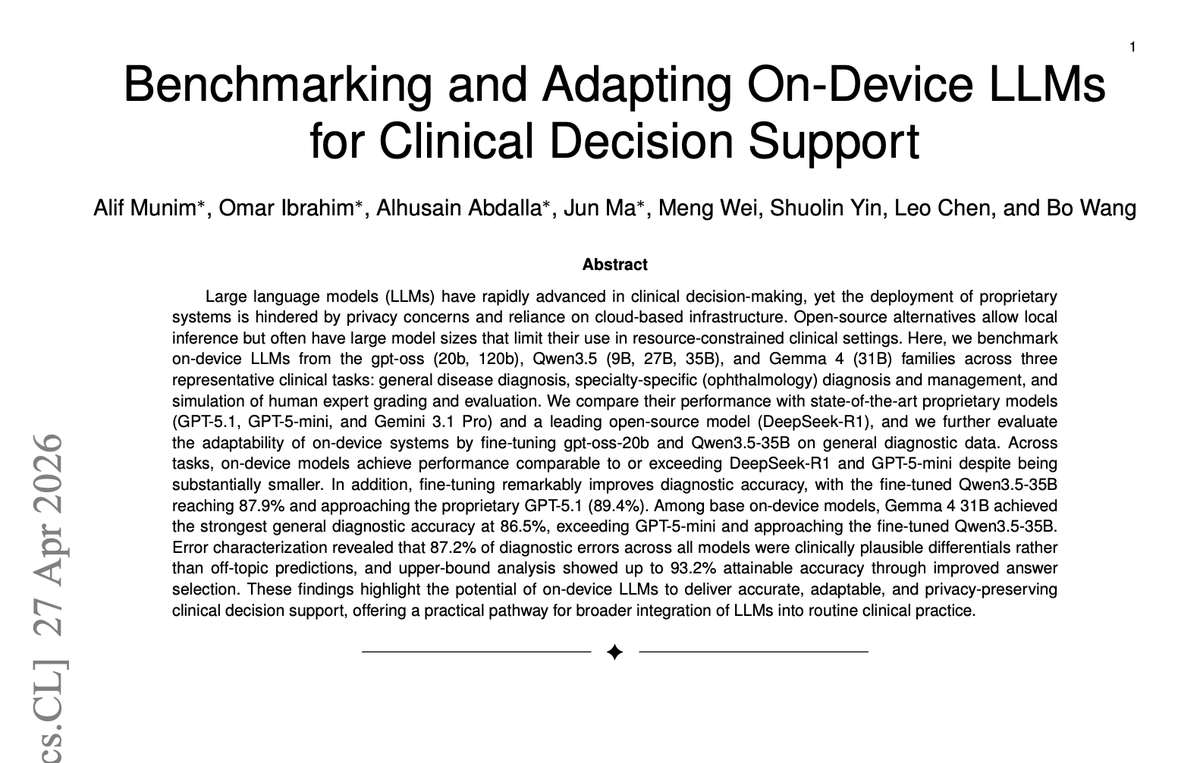
Just updated our paper on on-device LLMs for clinical decision support.
Paper: arxiv.org/abs/2601.03266
Here's why I think this matters:
We've been asking the wrong question. The debate around LLMs in medicine has been "how accurate are
they?", but the harder problem is deployment. Patient data can't leave the hospital. Most clinics don't have the bandwidth or budget for cloud inference at scale. The real question is: can a model that runs locally, on modest hardware, actually be trusted for clinical decisions?
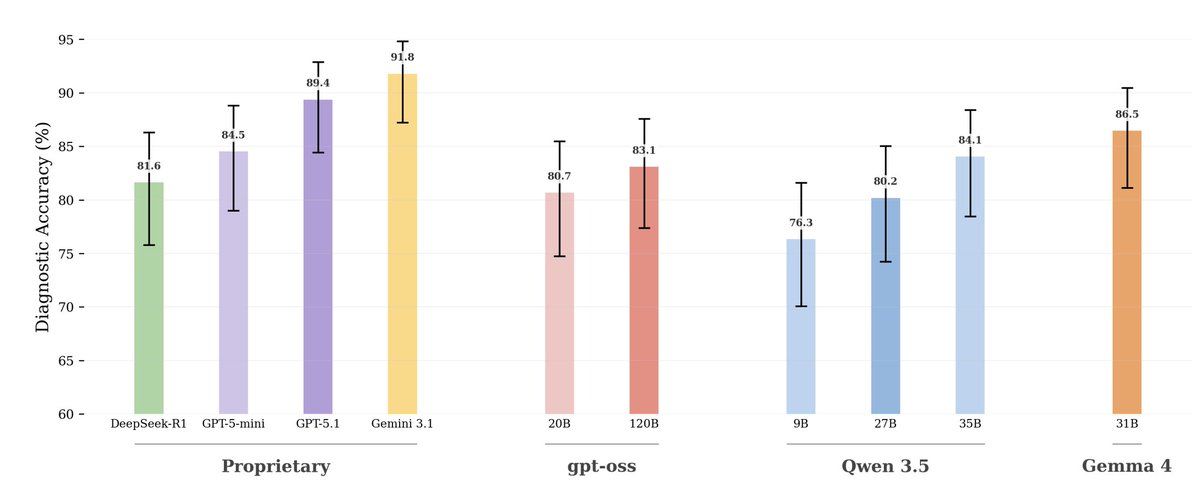
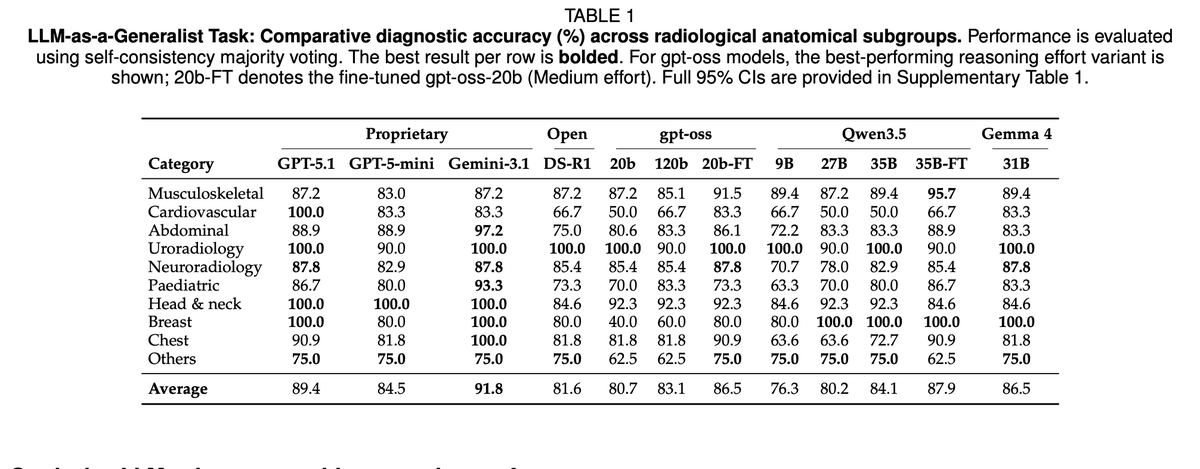
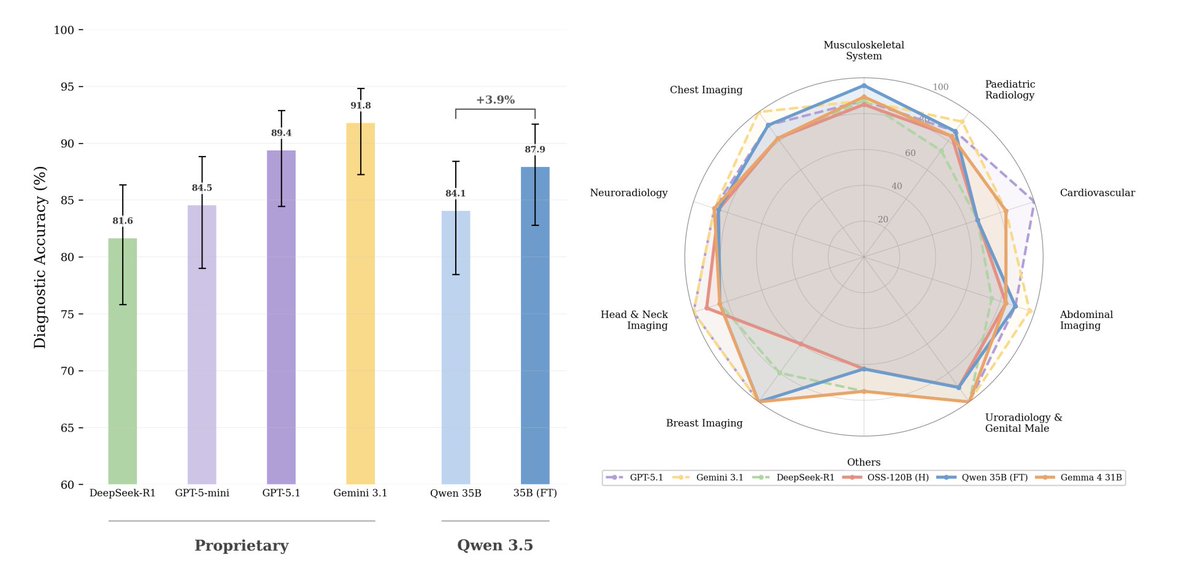
After benchmarking 188 models across general disease diagnosis, ophthalmology, and clinical judgment simulation — the answer is yes.
Gemma 4 31B (@googlegemma) hits 86.5% on general diagnosis, beats GPT-5-mini, scores 100% on uroradiology and breast imaging, and runs at 18 GB. Qwen3.5-27B (@Alibaba_Qwen ) at 16 GB matches DeepSeek-R1 at 671B, that is one-twenty-third the memory, same clinical accuracy. Fine-tune Qwen3.5-35B with domain-specific reasoning traces and it reaches 87.9%, approaching GPT-5.1 (89.4%). No extra memory. No cloud call. No PHI leaving the building.
One thing that surprised me: 87.2% of errors across all models were clinically plausible differentials. the model picked a reasonable diagnosis, just not the right one. Above ~31B parameters, hallucination rate drops to zero. Errors start looking like the kind a careful clinician makes on a hard case, not the kind that would make you distrust the system.
There's also a pass@3 upper bound of 93.2% for fine-tuned Qwen3.5-35B. The model already "knows" the right answer in most cases. That's a verifier problem, not a model-size problem.
Gemma 4 and Qwen3.5 are the first generation where the local deployment story actually holds up under rigorous clinical benchmarking. That's a real milestone.
Huge shoutout to the team who made this happen: Alif Munim (@alifmunim ), Omar Ibrahim, Alhusain Abdalla, Jun Ma @JunMa_AI4Health (all equal contributors), Meng Wei, Shuolin Yin, and Leo Chen from @UHN AI hub. Proud of what this group built 🔥🔥
11
27
147
13,305