
Creating interdisciplinary medical education to advance psychotropic deprescribing, safer tapering, and recovery. 501(c)(3) nonprofit. Join & donate today!
Joined August 2024
- Tweets 1,550
- Following 498
- Followers 456
- Likes 784
36 Photos and videos







Psychotropic Deprescribing Council retweeted

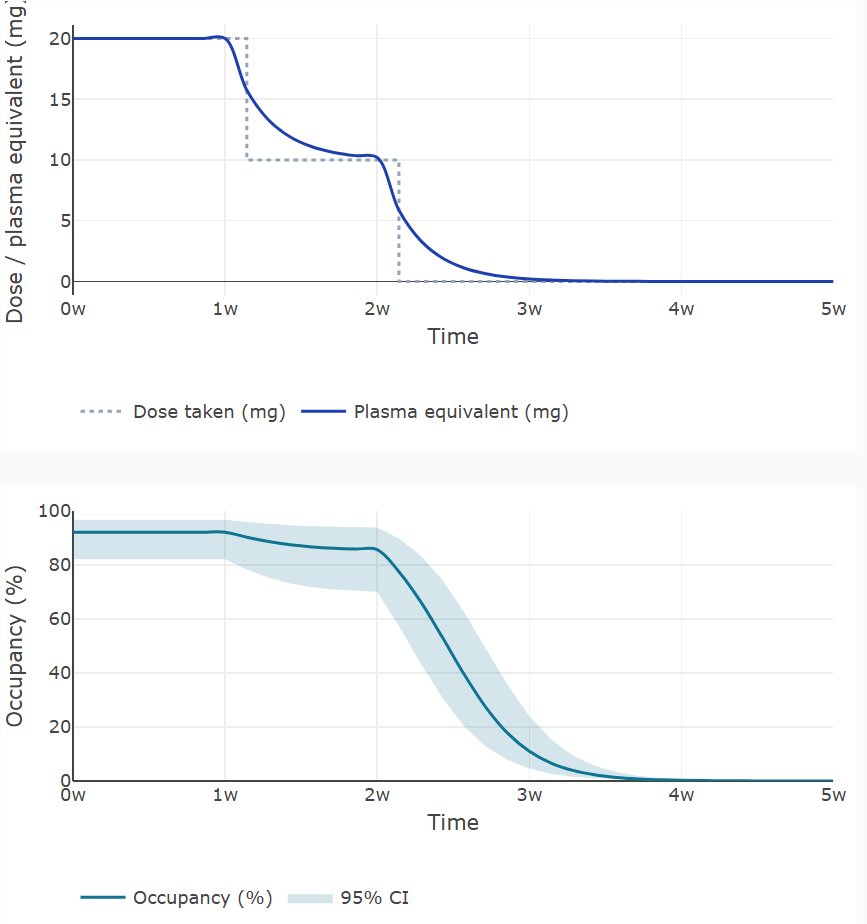
Very useful article in @TheBJPsych evaluating different off-lablel techniques for making small doses to make hyperbolic tapering feasible: reassuring that all were found to be within 90-110% of target values (the same standard used for manufactured tablets).

Hyperbolic tapering is increasingly recommended for the gradual reduction of psychiatric drugs to minimise withdrawal symptoms, yet available formulations rarely accommodate the small dose regimens required. cambridge.org/core/journals/…
5
13
28
2,384
With @RecoveryDoctor and @awaisaftab
agreeing that absolutism is not making psychotropic drug treatment any safer or improving outcomes, this is a BANNER DAY FOR WITHDRAWALOLOGY! 🎉🎆🎇🌈🙂
2
7
521
I agree with it, too.
Social media lends itself too easily to outraged declarations in absolutes. People who tend to black-and-white thinking anyway are over-represented.

This is important to read. 👇🏼👇🏼👇🏼
Even as I disagree with many parts of it (the permanent neurological injury and lived “saved” parts, for example, I wouldn’t assert), this is a necessary perspective. No absolutes, let’s not cancel each other out but try to do better.
98
Psychotropic Deprescribing Council retweeted

This is important to read. 👇🏼👇🏼👇🏼
Even as I disagree with many parts of it (the permanent neurological injury and lived “saved” parts, for example, I wouldn’t assert), this is a necessary perspective. No absolutes, let’s not cancel each other out but try to do better.

Dear anti-psychiatry, this "mental illness isn't real" narrative is making us look bad.
SSRIs can cause permanent neurological injuries that destroy lives via mechanisms we don't understand, and those experiences are not canceled out by the lives they 'save'.
That fact doesn't mean that mental illness isn't real, or is just a simple result of not enough sunshine or human connection. There are many forms of severe idiopathic mental illness that people suffer from, and those diseases are also deserving of legitimate treatment.
Has psychiatry exploited this and gone too far in some instances? Yes. Absolutely. Diagnosing every kid who can't sit still or focus with ADHD and medicating them is a criminal example of this.
However, there are many people who chronically struggle with severe mental illness that cannot easily be cured by natural remedies, and those people are desperate for help. The problem is that those people are just as vulnerable to SSRI neurological injury as those who 'didn't need' them. The mechanisms behind these injuries need to be fully understood, predictable and preventable before they continue to be carelessly given, period.
In the meantime, psychiatrists need to stop writing SSRIs off as merely "less than perfect", and the anti-psychiatry movement needs to stop promoting the idea that the mental illness that MI sufferers sought relief from isn't real in the first place.
The way forward is to simultaneously acknowledge that mental illness is real, and med harm is not just a necessary and unfortunate byproduct of trying to fix it. Med harm is real and a crime against humanity, and the suffering that leads people to become med harmed in the first place is equally real.
To reconcile these two outcomes by saying "they save lives, but they're not perfect" is not good enough.
Neither is saying "all mental illness isn't real, you just need more sunshine and meaning".
Psychiatry and anti-psychiatry needs to do better if we ever want this situation to progress.
5
2
9
1,176
Can't argue with "quasi-linear". Horowitz specifies that a hyperbolic taper can be adjusted at any step. Any psychotropic taper will be "quasi" in relation to a hypothetical model. Close monitoring of & communication with the patient is the key, to keep the taper comfortable.


3
7
597
Any tapering of a psychotropic must be tailored to the needs of the individual. No specific mode of taper guarantees success. The secret sauce has always been in the quality of monitoring the symptom pattern arising from dosage reduction.

3
3
13
739
Psychotropic Deprescribing Council retweeted

Week 1 of the Lived Nervous-System States Series
What Are Nervous-System States?
Many people experience benzodiazepine withdrawal as a constantly changing list of symptoms.
One day, the nervous system may feel intensely activated, restless, overstimulated, and difficult to settle.
Another day, it may feel heavy, disconnected, emotionally flat, exhausted, or unreal.
These shifts can feel confusing and unpredictable. Many people begin wondering if something entirely new is happening each time the experience changes.
Over time, however, many people notice that symptoms often organize into recognizable nervous-system states that can shift, overlap, and change.
Understanding these states can help withdrawal feel less random and more understandable.
Read the full article:
thebenzotaperdoctor.com/post…
#benzowithdrawal #nervoussystem #neurobiology
1
1
160
Psychotropic Deprescribing Council retweeted
People often track withdrawal one symptom at a time.
Anxiety.
Insomnia.
Dizziness.
DP/DR.
Internal shaking.
Restlessness.
But the nervous system does not always operate one symptom at a time.
Often, multiple symptoms occur together as part of a broader nervous-system state.
This is why the overall experience can sometimes feel dramatically different from one day to the next.
The question is not always:
"What symptom am I having?"
Sometimes the more useful question is:
"What state is my nervous system in right now?"
Diagram:
#benzowithdrawal #neurobiology #brainbody

1
1
137
Psychotropic Deprescribing Council retweeted

I agree that epistemic violence is real, especially when experiences of harm are dismissed or pathologized instead of being taken seriously. However, I think the problem is that the science is often limited and value-laden. There is a gap between certainty and humility where harm tends to happen.
2
1
7
1,145
Psychotropic Deprescribing Council retweeted

22 Mar 2021
DSM diagnosis can also be destructive if it:
1)is wrong
2)leads to needless/harmful treatment
3)promotes stigma
4)reduces expectations
5)creates hopelessness
6)has no expiration date
7)is rushed/unempathic
22 Mar 2021

Getting a DSM diagnosis can be a very positive turning point in a person's life if:
1)it is accurate
2)done with empathy
3)promotes feeling understood
4)inspires hope
5)reduces anxious uncertainty & feeling uniquely damned
10
18
109
Psychotropic Deprescribing Council retweeted

May 28
I have a shocking number of those but many are too easy.

1
1
7
181
Withdrawal-induced brain zaps are a symptom similar to L'hermitte's sign, from induced excitability of neurons instead of deterioration of neurons.
If taken regularly, potential remedies gabapentin, benzos, etc. may also cause withdrawal symptoms.

Yes they are liked to the mechanism .
The ‘reversal’ of the excitability of neurons. youtu.be/LJ2v21AyHgs?si=jyUy…
1
7
1,257
Psychotropic Deprescribing Council retweeted
Why do so many people end up on psychiatric medications when they no longer need them? Especially when the evidence says that it is safe to stop them?
Here are some thoughts on the topics of deprescribing, epistemic trust, and the questions we should be asking, but are not actually taking the time to make space for... 🧵
6
10
38
3,269
RT @javeedsukhera: The Institute of Living marked its bicentennial by introducing Radical Recovery. A vision for a future mental health sys…
3
Psychotropic Deprescribing Council retweeted

May 24
What to do when a patient is taking one med from each class?
Here's some answers from my APA talk:
chrisaikenmd.com/polypharmac…
Covered today in the NYT:
nytimes.com/2026/05/24/scien…
(full quote was "meds are not the answer... to all life's problems", oh well)
2
7
22
1,929
Another way withdrawal symptoms can confound research.
Just a reminder that in this trial participants were grossly under-treated with buprenorphine and had residual withdrawal symptoms. Had they been adequately treated for withdrawal it is likely that the benefit for yoga would have been zero. @JohnTorousMD
2
103
Psychotropic Deprescribing Council retweeted
Insightful comments from @awaisaftab in @WebMD summary of hyperbolic tapering: 'If thousands of people are online trying to figure out tapering strategies for themselves to manage antidepressant withdrawal, “something has failed in the medical establishment”' (realise it is a year old...)

If you’ve ever tried to stop an antidepressant and felt like you were "falling to pieces," you aren't alone. For many long-term users, the standard medical advice to taper off over just a few weeks can lead to a "cliff" of severe withdrawal symptoms. Seek a doctor who understands hyperbolic tapering. Hyperbolic tapering offers a personalized, slower path that respects how your brain actually heals. Read the full deep-dive on the science of hyperbolic tapering: wb.md/3RyYRmr
7
20
68
4,587
Psychotropic Deprescribing Council retweeted
May 23
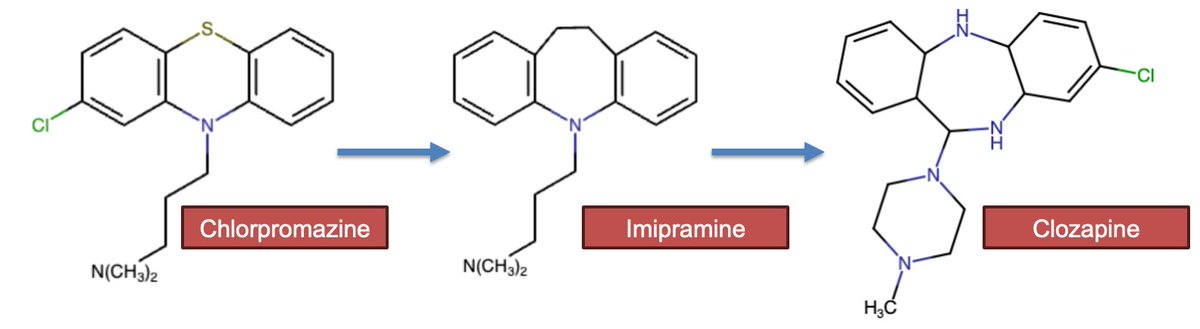
Most psychiatric medications were random mistakes based on methylene blue.
Pharmaceutical companies were chemistry companies that also made dyes. Methylene blue was the basis of Chlorpromazine (Thorazine/Largactil), which was the basis of Imipramine (Tofranil), the first tricyclic, which itself was the basis for the first second-generation antipsychotic Clozapine (Clozaril).
Chlorpromazine was meant for post-surgical agitation aid. Imipramine was a failed antipsychotic. Clozapine was a failed antidepressant.
Fluoxetine (Prozac) and SSRIs were the first psychotropic medications that didn't happen by happenstance. We knew that tricyclics' effect was more dependent on serotonin and selected that trait from Diphenhydramine (Benadryl).
While we are at it, lithium was a random solvent to carry schizophrenic urine.

16
71
381
27,518
If it's a 50/50 question, go with the answer you prefer.
May 23
I recommend coin flips to rumminators who cant make decisions
Why?
1)50/50 questions torture most
2)If there were clear right answer answer they'd know it
3)Deciding usually works better than ruminating
Exceptions: People contemplate self-destructive & impulsive acts.
1
1
108
Psychotropic Deprescribing Council retweeted
4 Aug 2025
“Wild that we are routinely giving a one-bond derivative of meth at the scale of tens of millions of prescriptions each year”
Dr. Chen reviews ADHD! He does a great job explaining the famous MTA study (including the complicated - why you cannot dismiss the finding that meds stop working based on the no-med group starting meds).
"Despite the common teaching that stimulants are 1st-line for ADHD in childhood, the best-controlled study of ADHD suggest that… Psychosocial and socioeconomic factors predict treatment response more than any treatment modality. Focus on modifying risk factors.”

9
16
41
7,385