
Joined February 2019
- Tweets 1,982
- Following 1,847
- Followers 388
- Likes 1,290
52 Photos and videos










William Jones retweeted

Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
92
1,273
6,503
1,151,191
William Jones retweeted

May 14
A WALK-OFF GRAND SLAM!
A MOMENT YOU DREAM OF AS A KID!
269
2,801
23,765
1,447,720
William Jones retweeted

Apr 29
The mic cut out during O Canada at the Sabres game.
Buffalo filled every single second of silence.
Sang it word for word.
This is how you tell your neighbors you see them.
We love Canada. Don’t listen to the noise.
484
3,136
22,317
748,152
William Jones retweeted

Mar 27
Tobi Lutke explains what the VCs who passed on Shopify got wrong
Tobi recounts pitching Shopify to VCs on Sand Hill Road a few years after founding Shopify.
Investors passed because they thought the addressable market was too small. At the time, there were about 40,000-50,000 online stores, and even if Shopify captured 50% of the market, that still wouldn’t be a venture-scale business.
When Tobi ran into the VC partner a few years ago, the partner asked Tobi what he missed (Shopify is valued at almost $100 billion today).
Tobi explained:
“You were actually correct, but what you didn’t realize was that Shopify was the solution to the very problem you identified. The reason there was only 40,000 online stores was because it was hard, expensive, and everyone who tried ran into all these brick walls of complexity, which Shopify, one after another, smoothed over and made simple to do.”
Tobi believes this is a common mistake:
“What a lot of free-market thinkers don’t understand is that between the demand and eventual supply lies friction. And I actually think that friction is probably the most potent force for shaping the planet that people just generally do not acknowledge… That was my theory when I turned my snowboard store into Shopify: there was a lot more people like me except there was too much friction which we needed to solve. And Shopify has proven out that every time we make the process simpler, there’s more consumption. At this point, we have a million merchants on Shopify, which is a mind-blowing number. So friction is a major component, and it’s something that software is uniquely good at reducing.”
Video source: @danmartell (2019)
34
76
956
169,028
William Jones retweeted

Oral anticoagulation after publication of the CLOSURE-AF trial and LAAC deemed “not non-inferior”. 😐
1
39
256
49,789

Mar 18
👀 Wow.

Among patients with atrial fibrillation at high risk for stroke and bleeding, left atrial appendage closure was not noninferior to medical therapy in reducing the risk of stroke, embolism, major bleeding, or death at 3 years. Full CLOSURE-AF trial results: nejm.org/doi/full/10.1056/NE…
Editorial: Left Atrial Appendage Closure — Another Overused Method in Cardiology? nejm.org/doi/full/10.1056/NE…
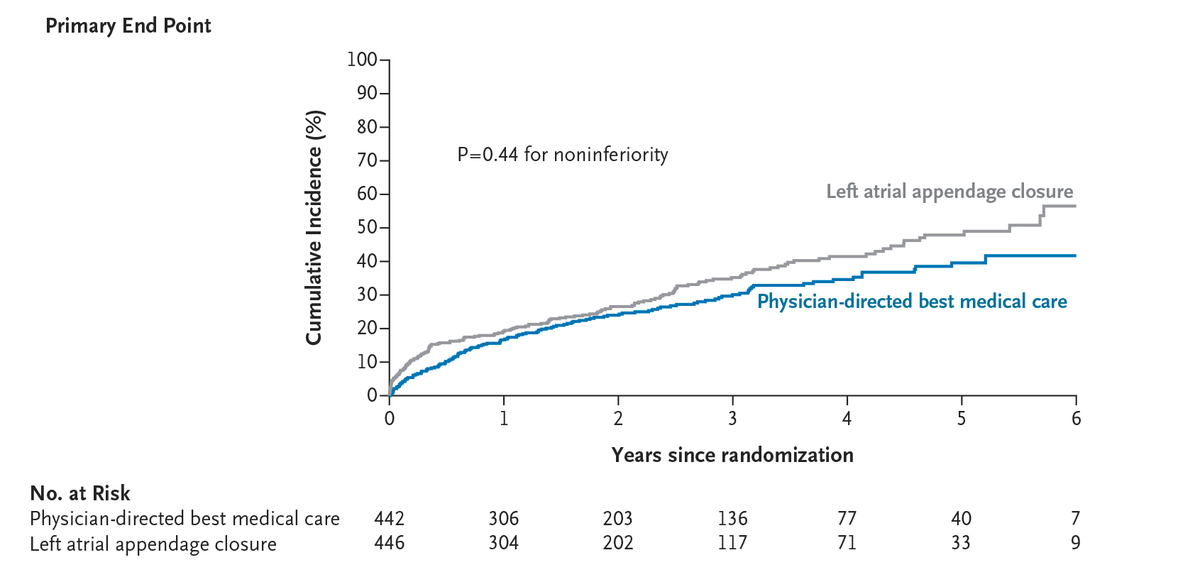
ALT A graph of the primary end point
109
The 510(k) is the 50-yard line, not the end zone. Read the full breakdown here: 510kto5.beehiiv.com/p/gettin…
#MedTech #Startups #HealthTech #510k #VentureCapital
28
William Jones retweeted

OpenAI Employees Raised Alarms About Canada Shooting Suspect Months Ago, Chose Not To Alert Canadian Authorities
Massive scoop by @WSJ about the Tumbler Ridge shooter. Devastating. My god. wsj.com/us-news/law/openai-e…
29
343
692
89,980
Jan 30
Episode 1 - AI Agents for Market Analysis youtu.be/rPehCeOqPB0?si=i80m… via @YouTube #EPeeps #Medtech #LAAC #LAAO #WATCHMAN #AIAgents #Sales #Marketing #Executive
79
William Jones retweeted

Jan 24
We’re buying Canadian, and we’re building Canadian.
8,571
8,802
71,966
4,334,443
William Jones retweeted
Jan 19
I’m in Davos, Switzerland, to secure new trade and investment partners for Canada.
Because Canada has what the world wants — we’re an energy superpower and a reliable trading partner, with the most educated workforce in the world.
6,456
6,767
57,446
2,363,379
William Jones retweeted

Jan 6
Lego launches Smart Brick and high tech Star Wars toys at CES 2026
226
615
4,645
1,266,062
William Jones retweeted

28 Dec 2025
Adding in the cost of an intracardiac ultrasound catheter should do wonders to boost the cost efficacy of this super high value procedure. Grin. Cc @kaulcsmc
28 Dec 2025

Zero-fluoroscopy Left Atrial Appendage Occlusion with the Watchman FLX Device
heartrhythmjournal.com/artic…

4
33
9,412

William Jones retweeted

24 Nov 2025
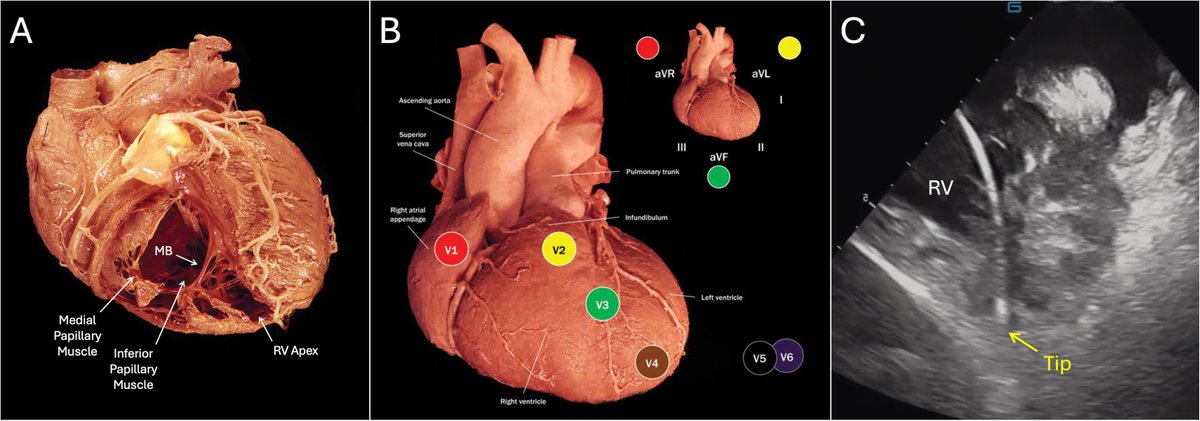
Ablation of Idiopathic Ventricular Arrhythmias from the Right Ventricular Apex #OpenAccess
@rdschaller
heartrhythmjournal.com/artic…
22
67
8,526
William Jones retweeted

9 Nov 2025
I agree with @drjohnm’s perspective on LAAC.
As an additional piece of orthogonal evidence: Our group, as well as multiple others, have shown that AI-ECG can predict AF from sinus ECGs. When you apply these models or try to directly train an AI-ECG model to predict stroke, they perform poorly. Given the publication bias of negative results, we’ve never tried to publish this work, but we’ve tried tens to hundreds of approaches, but AI applied to ECG uniformly only weakly predict stroke.
In parallel, notice that most of the input variables for CHADs2vasc and other stroke risk calculators primarily have EXTRACARDIAC risk factors. There is a long list of positive trials that show efficacy of anti platelet therapy and anticoagulation for stroke, but these are systemic therapies for what’s likely a systemic issue. In parallel, there’s almost an equally long list of negative trials for treatments that are cardiac only (LAAC and PFO closure).
Treating a sole cause (no matter how compelling) when there are multiple culprits of similar effect size is a losing strategy. Sick patients are more likely to have strokes, irrespective if they have AF or don’t have AF. In this way, AF is almost a collider. An to clarify, maybe a little pedantic, LAAC is and never as been a treatment of/for AF. It is a potential (but not very efficacious) treatment for stroke. Systematic therapies have a much larger surface area of potential efficacy compared to targeted treatments that only one mechanism of action/benefit.
An analogy from one of my former attendings, David Liang, come to mind. When humans were on the savanna and more active, it makes sense to err in being slightly hypercoagulable. If you had a chance of being bitten by wild animals, evolution probably selected for faster clotting. But now, we mostly sit out coaches and chairs all day, perhaps the same risk trade off no longer applies. Perhaps most people might benefit from a little anticoagulation, and this corroborates the gradual expansion of indications low dose anticoagulation therapy. This is not true for mechanical devices in the heart.
9 Nov 2025

Great comments below: "but at this stage it seems appropriate to pause and reflect."
Good luck with that Professor. I've been encouraging a pause and reflection on 5 continents, with little success.
All of this could have been predicted from PROTECT and PREVAIL data.
4
20
79
26,256
William Jones retweeted
9 Nov 2025
Great comments below: "but at this stage it seems appropriate to pause and reflect."
Good luck with that Professor. I've been encouraging a pause and reflection on 5 continents, with little success.
All of this could have been predicted from PROTECT and PREVAIL data.
9 Nov 2025

Bad news for enthusiasts of left atrial appendage closure from #AHA25. CLOSURE-AF is not yet published, but reports from New Orleans indicate inferiority compared with best medical care (the trial was designed for non-inferiority, making this the most unexpected and unfavorable scenario).
In 888 patients with atrial fibrillation considered at high risk for stroke and bleeding, a composite endpoint of stroke, systemic embolism, cardiovascular or unexplained death, and major bleeding occurred in 16.83% of patients who underwent left atrial appendage closure and 13.27% of those receiving best medical care (whose exact definition remains unclear — we’ll hopefully find out once the paper is available).
These appear to be patients in whom the appendage is perhaps closed somewhat lightly — the rationale often being “so they won’t need lifelong anticoagulation.” Well, lifelong benefit remains to be seen, but after a median follow-up of 3 years, the risk of events was 28% higher with appendage closure, with a 95% confidence interval for the hazard ratio indicating a potential 1 to 62% increase in risk.
In short, the results are not definitely encouraging, and much remains to be understood. Which events increased? Likely ischemic ones. And further — was it appropriate for the trial to combine ischemic and bleeding events, along with cardiovascular death, into a single non-inferiority endpoint? Probably not, yet the findings have disrupted expectations and made the discussion quite compelling nonetheless.
Finally, could the expected long-term reduction in events (beyond 3 years, potentially lifelong) eventually offset the initial, possibly procedural and hemorrhagic, risks — shifting the balance back in favor of closure for patients with longer life expectancy and prolonged exposure to anticoagulation? Hard to say without full data. And in any case, this is only one trial; at least three others are ongoing in high bleeding-risk populations (STROKECLOSE, CLEARANCE, and LAA-KIDNEY).
Let’s also recall that somewhat more favorable data have been seen in anticoagulation-eligible populations, but at this stage it seems appropriate to pause and reflect.
If you’d like to reflect with us, join the @escardio webinar on Monday, where I’ll also be participating — it feels perfectly timed.
esc365.escardio.org/event/20…
5
19
88
47,759
William Jones retweeted
3 Nov 2025
It’s our country, it’s your future, and we are going to give it back to you.
2,604
439
2,754
238,285

Davis Schneider's dad captured the moment his son hit a leadoff homer in #WorldSeries Game 5 🥹
📹: @bballdad44745
95
677
6,749
384,057
30 Oct 2025
Let me know, I'm ready.
29 Oct 2025

Maybe we should do this
98