
Abbott EP
Joined May 2013
- Tweets 268
- Following 381
- Followers 1,112
- Likes 5,132
57 Photos and videos










Mike Lean retweeted
Starting the year with a recap on a recent challenging VT case at @mhshospital @Mapbastian @JC_EPMaps @mike_lean @joel_chic
A 3rd time redo in a non-ischemic VT patient.
Success in these cases requires the use of advanced techniques - however, advanced techniques do not mean unsafe procedures.
Some specific workflow highlights that led to a successful bipolar case without complications and 0 clinical VT on follow-up:
- Meticulous mapping was performed to fully understand each VT before delivering energy.
- Reentrant VTs are inherently 3D in nature, often revealing only a portion of the channel in the chamber mapped (in this case, only the exit for each VT).
- Entrainment at the presumed VT exit confirmed what the map suggested.
- Remote entrainment from the RV was helpful to confirm diastolic signals on mapping catheter were within circuit.
#AblateVT #EPpeeps #WIC #WomenInEP
4
13
79
5,235

17 Nov 2025
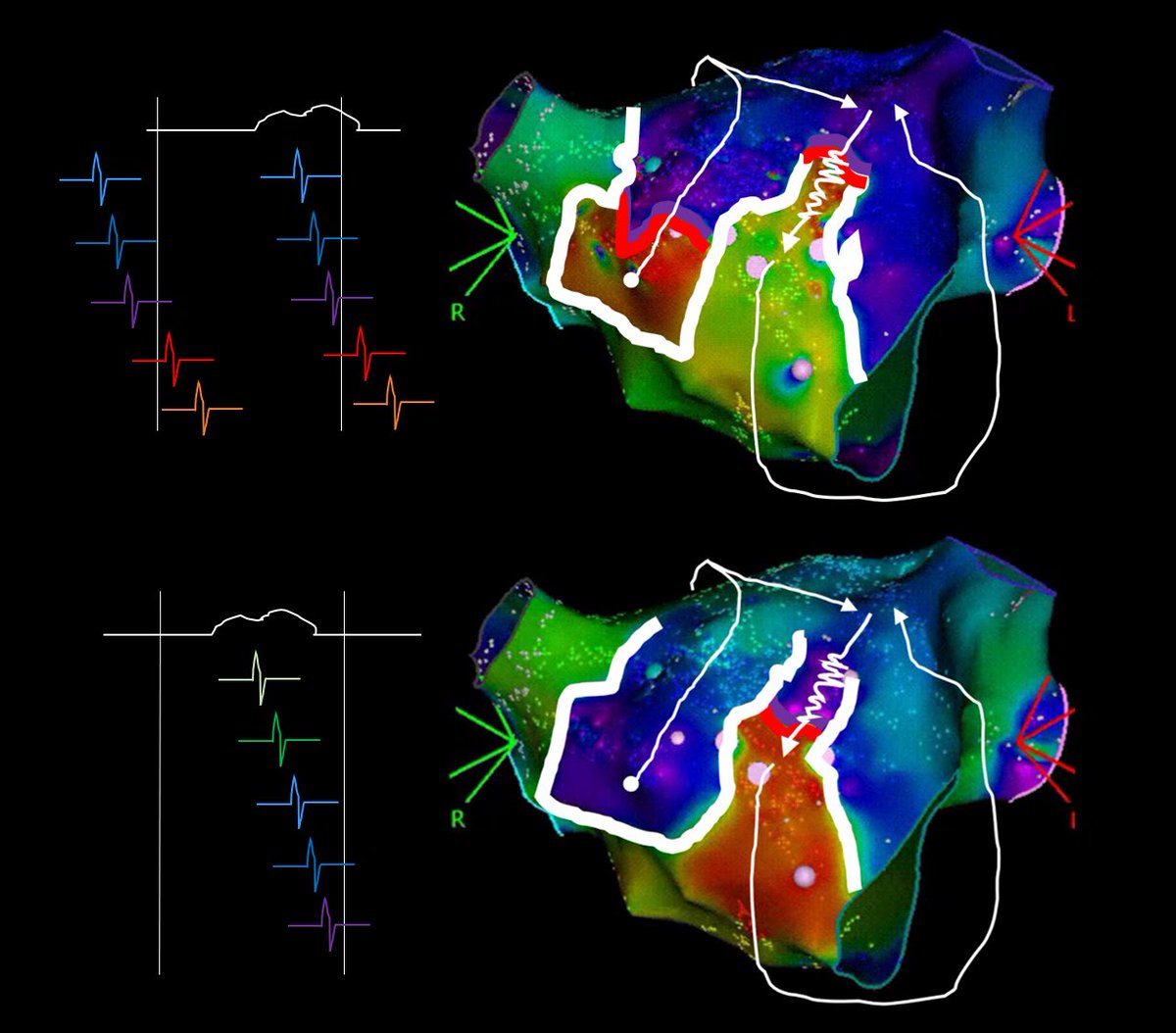
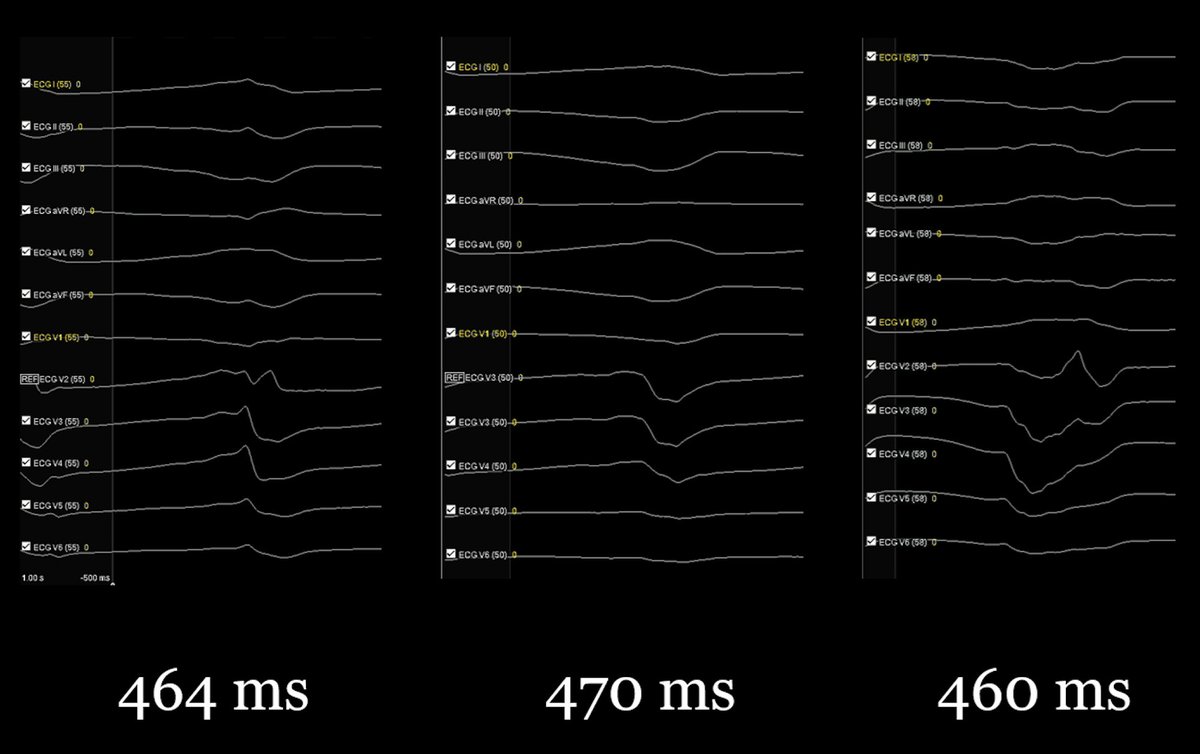
Some post-case learning with @danealson (Dr. Neal Bhatia) and @_shannonmillard: following an ischemic VT case, together we compared how the clinical VT circuit presented when mapped with the First Deflection algorithm versus EnSite™ OT Near Field.
What we found brings up an interesting question. Is it better to….
- Force the system to visualize the full circuit with First Deflection, or
- Illustrate the potential midmyocardial bridges and touchdown points with OT NF?
While there may not be a "correct" answer, we think there is value in appreciating both pieces of information. And if nothing else, it makes for a fun discussion with talented colleagues like Dr. Bhatia and Shannon.
7
25
103
6,712
Mike Lean retweeted

11 Aug 2025
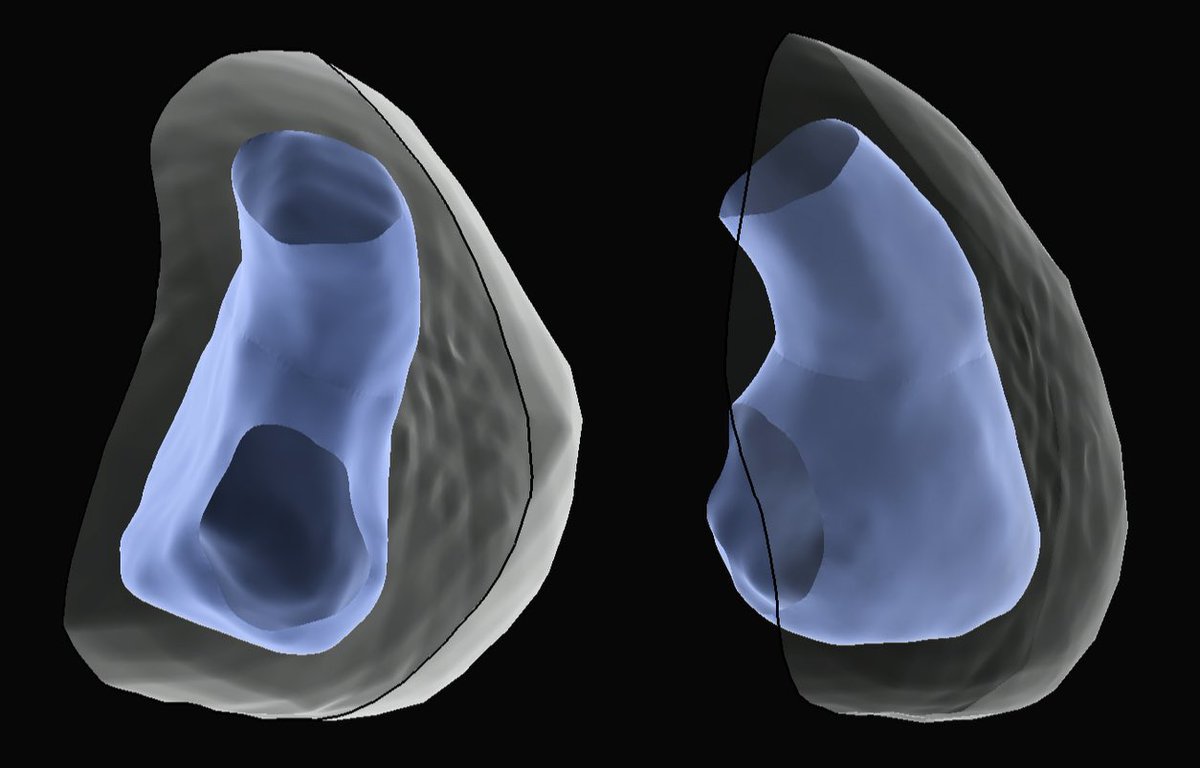
Utilization of #AI based tools for delineating cardiac structures with ICE during #AblateVT cases as part of #FIH trials with new @AbbottCardio exceeded expectations - rapid definition of valves, paps in LV:
3
64
201
10,153
Mike Lean retweeted

26 Jul 2025
"Roads...where we are going, we don't need roads."
Happy to share our work @rimhalabymd @ChrisGBruce13 using VINTAGE for intramural VAs - first in human. We demonstrated that we can successfully navigate to "inaccessible" areas such as the LV summit, deep septum, and papillary muscles and deliver successful ablation lesions. More to come on this exciting new "space" in VT!
jacc.org/doi/10.1016/j.jacep…
@melchami99 @FaisalMMerchant @BadhwarNitish

19
45
5,787
Mike Lean retweeted

15 Apr 2025
Challenging VT storm with multiple morphologies in a hemodynamically unstable patient for redo procedure. Substrate-guided strategy, focusing on areas of wavefront discontinuity with dual pacing wavefronts suggested a potential VT isthmus. Area corresponded nicely with @inheartmedical wall thinning. Non-inducible on PES after RF. @AbbottCardio @mike_lean @Mapbastian
Thankful for lessons learned @JRWinterfield @Davilandre @DrRoderickTung #AblateVT #NoExitBias #EPeeps #WADL
2
12
65
3,981
Mike Lean retweeted

7 Apr 2025
8
41
126
7,433
Mike Lean retweeted

10 Mar 2025
VT storm ablated with a first burn term over the weekend thanks to @JRWinterfield. #GridX with OT near field algorithm allowed for quick and accurate mapping in complex substrate.
3
15
65
8,566
Mike Lean retweeted
20 Feb 2025
LAD infarct VT. Critical isthmus and bystanders. Mapped, entrained, and ablated by the skilled @dhakalbish @MUSC_EP #GridX
7
28
100
6,707
Mike Lean retweeted
7 Feb 2025
Enjoyed assisting with some workflow and technology improvements in FIH trials of novel Viewflex X ICE catheter from @AbbottCardio -- we performed ablation of PVC from suspected intramural site with RF to septal RVOT and adjacent ASOV. Will be curious to see what @dhakalbish thinks with his @PennEPFellows based ICE approach in trials tomorrow. Contouring of key structures including pap muscles and ASOV shown below:
@AMatthews0 @mikelean @Zachkoch13
8
57
176
14,697
Mike Lean retweeted
31 Jan 2025
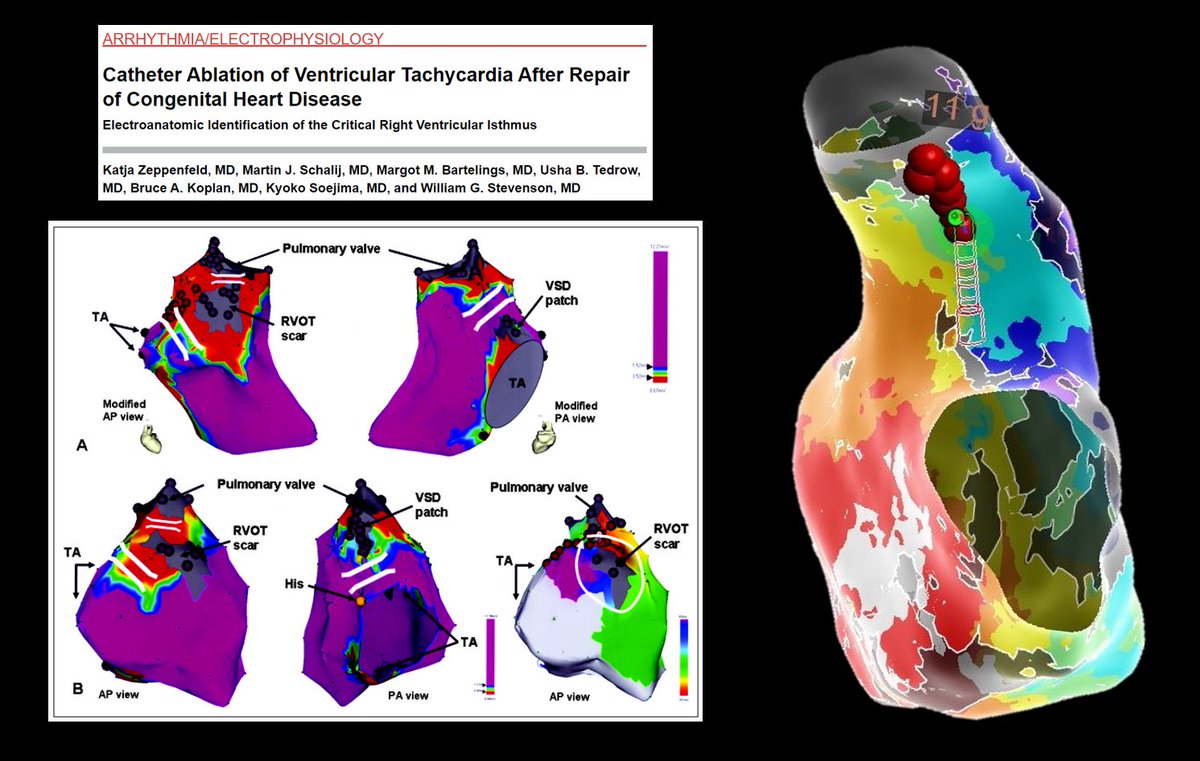
Re-entry around suture lines in a DILV with bidirectional Glenn and modified Fontan using the right atrial wall to create a bridging tunnel between discontinuous pulmonary arteries. #EPeeps #WIC #WomenInEP #ACHD @mhshospital @DanielBenhayon fantastic support from @AbbottCardio @ADAS3D @Mapbastian for pre and intraoperative image guidance.
7
32
5,170
14 Jan 2025
It is amazing to reflect on how many specialties and technologies had to come together to make this case and collaboration happen. At the forefront of this is @FergieLosiniec1 - thank you for being a pioneer and a top-class operator!
14 Jan 2025

Great case of ICE guided LAAO with @medinbox @AbbottCardio support. @medinbox allows for procedural support worldwide between physicians and key specialist that can assist with tips during complex cases. It was super easy to connect. Looking forward to sharing more cases with my peers all around the world. Thanks for the visit! @KahabkaMark @Austin_in_EP @mike_lean @Mapbastian @joel_chic
1
14
1,923
Mike Lean retweeted
21 Dec 2024
Great case of concomitant PVI/ICE guided LAAO. Thanks for the support @BSCCardiology @emilystoicovy @AbbottCardio @mike_lean @Mapbastian @mhshospital #Epeeps
2
4
19
1,853
Mike Lean retweeted

6 Nov 2024
Great heart dissection with the EP fellows at @UABCardiology. Incredible insight from the very knowledgeable cardiac pathologist, Dr. Silvio Litovsky! @AbbottCardio @WilliamMaddoxMD @tommcelderry



6
19
1,697
3 Sep 2024
Hypnotizing local reentry in a stable post-maze tachycardia, with full CL seen on HD Grid.
What is the cause/substrate for this type of AT after a maze procedure?
@AbbottCardio #EPeeps
Case with Dr. Smriti Banthia in Sarasota, FL.
2
26
83
5,737
30 Aug 2024
PVI with #FARAPULSE converted persistent AF into this 310 ms AFL. Also note the anomalous PV on the posterior wall. What is your ablation strategy?
@AbbottCardio #EPeeps
Case with Dr. Dilip Mathew in Sarasota, FL.
10
12
45
6,331
31 Aug 2024
Termination at the suspected critical isthmus. As many of you commented, this probably would have terminated in a few different locations, as it appeared to be roof-dependent.
We continued on to complete the anterior line, posterior wall to include the anomalous vein, and also SVC isolation. Therapy map in next comment.
@forkknifecab_EP @MattMelcherPA @narrowQRS @javadm20 @sigfusgiz @andreilew @Mohamed74057845
1
1
7
1,222
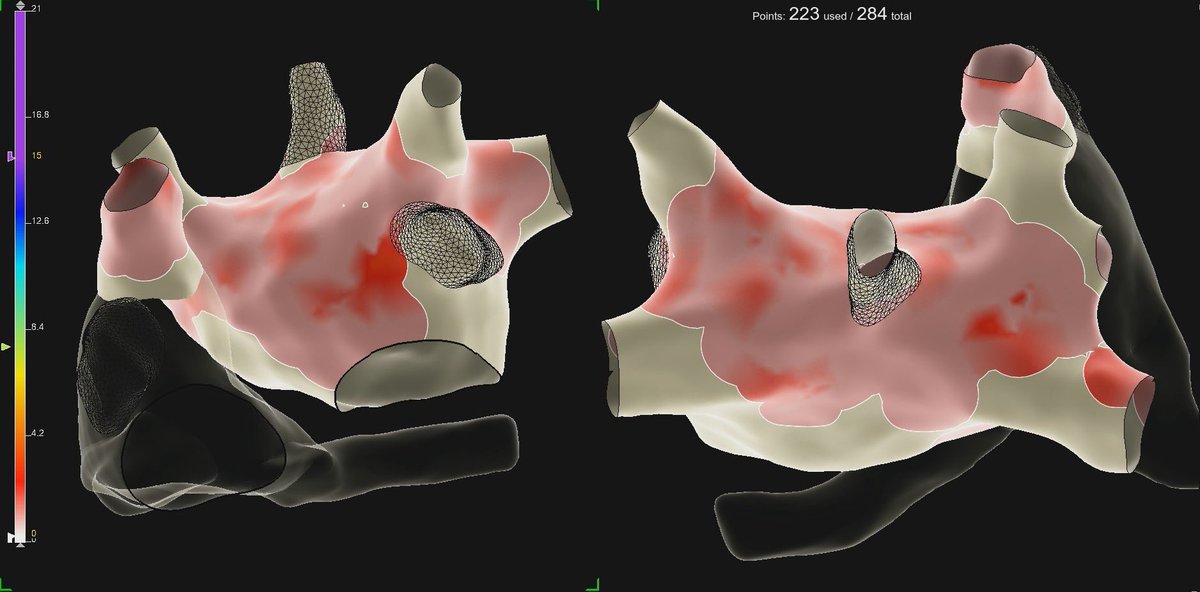
31 Aug 2024
PF Projection Overlap Map of PVI, posterior wall, anterior line, and SVC isolation.
1
1
776
8 Jul 2024
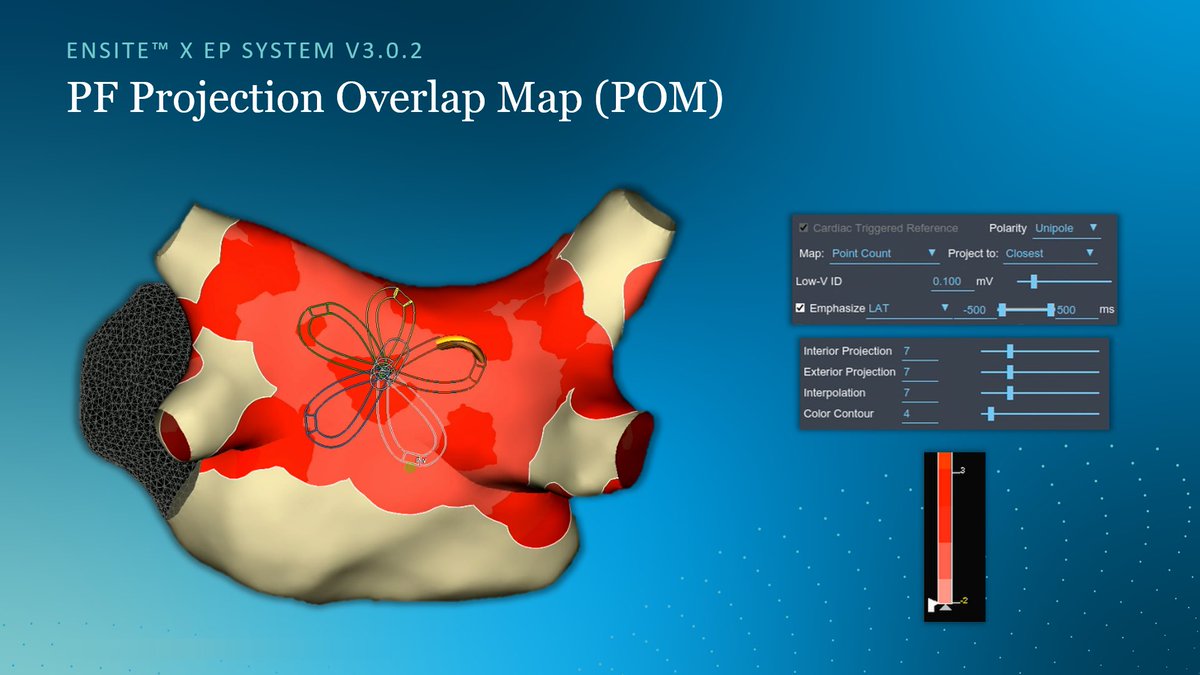
Projection Overlap Map (POM) to show locations with multiple therapy applications in PFA cases.
Here are the map settings we landed on using the “Point Count” map type. Looking forward to seeing what clinical utility this has, and also how the @AbbottCardio teams continue to expand & refine this strategy.
3 Jul 2024

Great fluoroless PFA case completed with @GXMoralesMD of Grandview Medical Center in Birmingham, AL . This time using the new Projection Overlap Mapping (POM) which identifies areas of PF application overlap. Mapping and video courtesy of @DavidSmithAbtEP @mike_lean @AbbottCardio
1
19
48
8,376
Mike Lean retweeted
3 Jul 2024
Great fluoroless PFA case completed with @GXMoralesMD of Grandview Medical Center in Birmingham, AL . This time using the new Projection Overlap Mapping (POM) which identifies areas of PF application overlap. Mapping and video courtesy of @DavidSmithAbtEP @mike_lean @AbbottCardio
1
10
29
11,694
2 Jul 2024
Great thread by @officialdrk12 describing a stepwise approach to mapping and ablating an unstable non-ischemic VT.

What would you do if the VT is too unstable to map or entrain? Let’s look at how understanding VT substrate is paramount in this case.
21
2,318